
Abstract
Aims:
To investigate the short-term effects of the first wave of COVID-19 on clinical parameters in children with type 1 diabetes (T1D) from 82 worldwide centers participating in the Better Control in Pediatric and Adolescent Diabete
Materials and Methods:
Aggregated data per person with T1D ≤21 years of age were compared between May/June 2020 (first wave), August/September 2020 (after wave), and the same periods in 2019. Hierarchic linear and logistic regression models were applied. Models were adjusted for gender, age-, and diabetes duration-groups. To distinguish the added burden of the COVID-19 pandemic, the centers were divided into quartiles of first wave COVID-19-associated mortality in their country.
Results:
In May/June 2019 and 2020, respectively, there were 16,735 versus 12,157 persons, 52% versus 52% male, median age 13.4 (Q1; Q3: 10.1; 16.2) versus13.5 (10.2; 16.2) years, T1D duration 4.5 (2.1; 7.8) versus 4.5 (2.0; 7.8) years, and hemoglobin A1c (HbA1c) 60.7 (53.0; 73.8) versus 59.6 (50.8; 70.5) mmol/mol [7.8 (7.0; 8.9) versus 7.6 (6.8; 8.6) %]. Across all country quartiles of COVID-19 mortality, HbA1c and rate of severe hypoglycemia remained comparable to the year before the first wave, while diabetic ketoacidosis rates increased significantly in the centers from countries with the highest mortality rate, but returned to baseline after the wave. Continuous glucose monitoring use decreased slightly during the first wave (53% vs. 51%) and increased significantly thereafter (55% vs. 63%, P < 0.001).
Conclusions:
Although glycemic control was maintained, a significant rise in DKA at follow-up was seen during first wave in the quartile of countries with the highest COVID mortality.
Trial Registration:
NCT04427189.
Introduction
Recent global estimates of type 1 diabetes (T1D) indicate that 40% of the 9 million cases are below the age of 40 years. The prevalence is about 10 times higher in high-income versus low-income countries. 1 The COVID-19 crisis has led to global disruptions in routine models of outpatient and inpatient clinical care. Many diabetes centers shifted to telemedicine, particularly in pediatric diabetology. 2,3 Normal routines for people with diabetes and access to health services have also been significantly disrupted. 4 –6 It is intuitive that such an upheaval should have immediate short-term effects on health outcomes, 7 and registries are well adapted to detect such changes. As the COVID-19 pandemic has been global, registries collecting data from around the world are particularly well suited for such an analysis.
In adults with type 1 or type 2 diabetes, the risk of severe illness or death with COVID-19 is substantially increased compared with the risks in people of the same age in the background population. 5 In contrast, young people with or without T1D are not as severely affected by COVID-19 as adults. 4,8 Early in the pandemic, there was speculation that the crisis may even constitute a paradigm shift in health care delivery for T1D, as the young generation is more likely to use diabetes technology which may be an advantage. 2 While there is no doubt that the absolute risk of fatal or critical care unit-treated COVID-19 will mostly reflect the efficacy of mitigation measures in countries and the respective stage of the pandemic, 7 little is known on the short-term effects of the COVID-19 crisis in vulnerable populations like children with T1D worldwide. 9
The international SWEET (Better Control in Pediatric and Adolescent Diabete
Materials and Methods
This analysis was based on data from the international, prospective, multicenter diabetes SWEET registry. SWEET (NCT04427189) was approved by the Ethics Committee of Hannover Medical School and is associated with the AUF DER BULT Diabetes Center for Children and Adolescents, Hannover, Germany, which coordinates the SWEET collaboration. Each center must meet specific entry criteria showing diabetes expertise and compliance with the International Society for Pediatric and Adolescent Diabetes (ISPAD) clinical practice guidelines. The local Institutional Review Boards of the participating centers approved the pseudonymized data collection.
As of December 2020, the SWEET registry includes 76,854 participants and 883,207 visits from 100 diabetes centers worldwide. The SWEET database combines data from distinct sources. Data are collected locally through clinical databases, electronic health record systems, the standardized SWEET-DPV-documentation software (
Criteria for inclusion in this analysis were centers with data from individuals with T1D aged ≤21 years in May–June 2019 as well as May–June 2020. A total of 22,820 patients from 82 centers were available for this analysis (Supplementary Fig. S1). Data from eligible children and youths with T1D from these centers were aggregated for each subject during the observation periods.
Data on cumulative deaths per 1 million people due to COVID-19 during the first wave (March–June 2020) were retrieved from the COVID-19 Data Repository by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (
Outcome variables
Glycemic control was assessed by hemoglobin A1c (HbA1c) measured locally in each center. To adjust for differences between laboratories, the multiple of the mean method was used to standardize local HbA1c mathematically. Daily insulin dose is expressed as U/kg/day. Insulin therapy was classified as pump therapy or injection therapy. Any use of continuous glucose monitoring (CGM, either real-time or intermittent scanning device) was analyzed.
To adjust for age, gender, body mass index (BMI), and height, standard deviation score (SDS) values were calculated using the international pediatric reference data from the World Health Organization (WHO) (
Statistical analysis
Descriptive data are presented as median with quartiles or percentages. The Wilcoxon test was used to compare continuous variables, and the chi-squared test was used for binary variables. SWEET centers were stratified into quartiles of COVID-19 cumulative deaths per 1 million people. Linear repeated measurement models with an autoregressive covariance structure were used for continuous outcomes and logistic regression models for binary outcomes. Regression models were adjusted for age (categorized into <6, 6–<12, 12–<18, ≥18 years), sex, and diabetes duration (categorized into <2, 2–<5, 5–<10 and ≥10 years).
In addition, an interaction term between time period and COVID-19 cumulative death categories was included to all models. To rule out those differences in data collection-biased results, we calculated the difference in the number of individuals in 2020 versus 2019 and added this to our main model in a sensitivity analysis. Results are presented as adjusted means or frequencies together with 95% confidence intervals. A two-sided P-value <0.05 was defined as statistically significant. P values were corrected for multiple testing using the false discovery rate method. All analyses were performed with Statistical Analysis Software 9.4 (SAS, SAS Institute, Inc., Cary, NC).
Results
A total of 22,820 patients with T1D ≤21 years of age from 82 centers were available for the period May/June and 21,820 individuals for the control period August/September (Supplementary Fig. S1). To investigate the impact of the first wave of the COVID-19 pandemic, aggregated data per person with T1D ≤21 years of age were compared from centers in May/June and August/September of 2019 and 2020 (Table 1). In 2019 and 2020, respectively, data were available from 16,735 versus 12,157 children with T1D. Overall, the unadjusted clinical data between both time points were comparable regarding gender, age, T1D duration, BMI-SDS, and insulin dose. On average, the COVID-19 cohort had a slightly lower HbA1c, more insulin pump and less CGM use, lower rates of severe hypoglycemia, and a higher frequency of DKA.
Clinical Characteristics of Pediatric Type 1 Diabetes Patients <21 Years Given as Median (Q1, Q3) or Percentage Documented in 2019/2020 (May–June) or August/September Respectively
May–June.
August–September.
Kruskal–Wallis test for continuous variables and chi-squared test for binary variables, adjustment for multiple comparisons with false discovery rate.
BMI, body mass index; CGM, continuous glucose monitoring; CSII, insulin pump; DKA, diabetic ketoacidosis; HbA1, hemoglobin A1c; SDS, standard deviation score.
To distinguish the added burden of the COVID-19 pandemic on health care delivery, the centers were divided into quartiles of first wave COVID-19-associated mortality in their country (Table 2). Compared to the same period in 2019, 27% fewer patients were reported to the registry in May/June 2020 and 8% fewer patients were documented for August/September 2020, with wide variations between centers. The average percent change in patient data uploads was not associated with the quartile of COVID-19 mortality (Table 2).
Stratification by COVID-19 Cumulative Deaths per 1 Million People Between March and June 2020 Divided into Quartiles
May–June.
August–September.
SWEET, Better Control in Pediatric and Adolescent Diabete
Across all country quartiles of COVID-19 mortality, HbA1c and rate of severe hypoglycemia remained comparable to the year before the first wave, while DKA rates increased significantly in the centers from countries with the highest mortality rate in the period May/June (Fig. 1, Table 3). Glycemic control assessed by HbA1c tended to be better (estimated mean difference: Q1: −1.4 mmol/mol (−0.13%), Q2: −2.1 mmol/mol (−0.19%), Q3: −1.8 mmol/mol (−0.17%), and Q4: −0.9 mmol/mol (−0.09%) during the lockdown in May/June (Fig. 1) although not reaching statistical significance (P-value of interaction term >0.05).
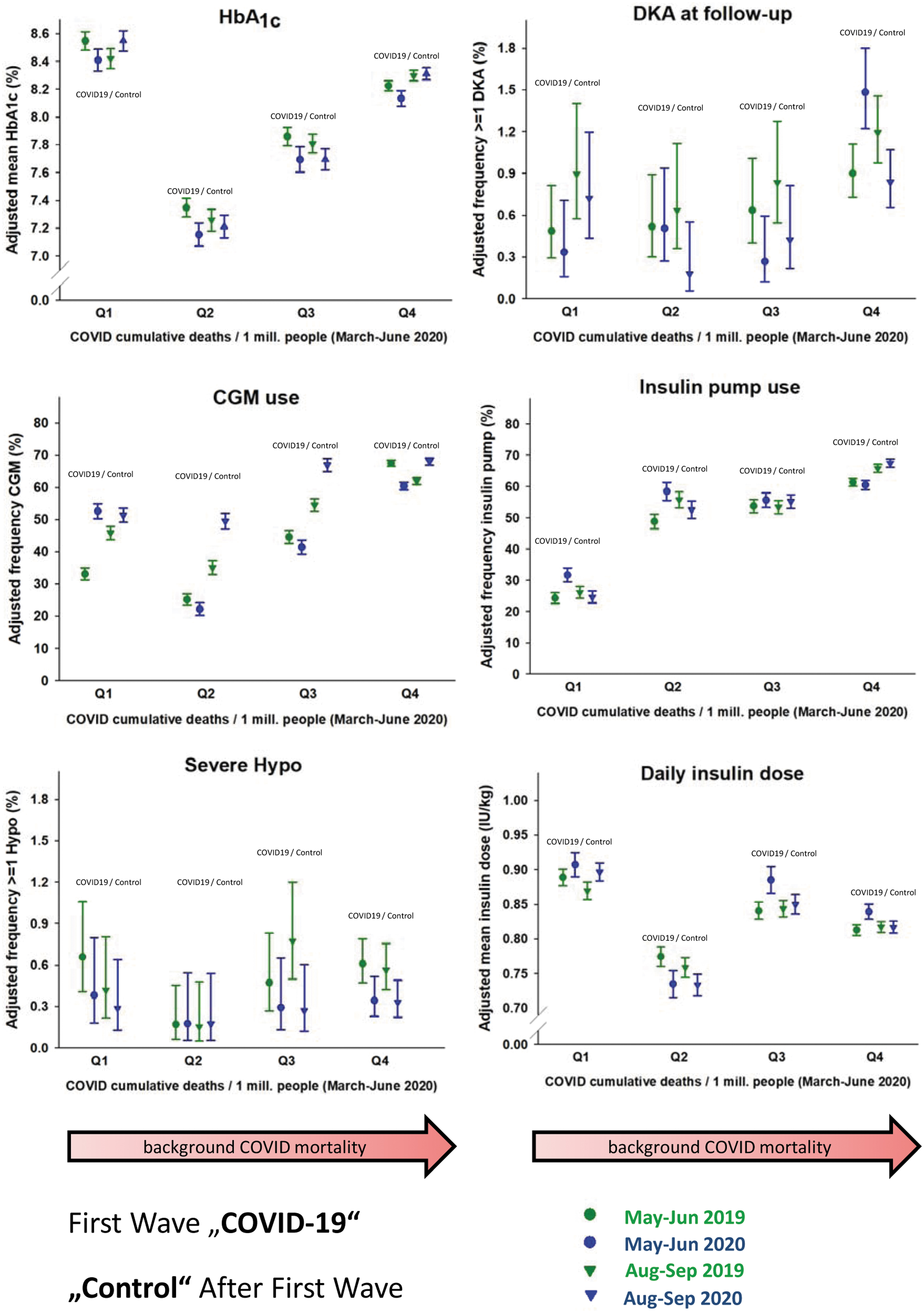
Adjusted comparison of glycemic control, DKA rates, rates of severe hypoglycemia, insulin doses, and proportion of patients on insulin pump or CGM between four time periods May/June and August/September in the year before the COVID-19 pandemic (green circles and triangles) and during/immediately after the first wave (blue circles) or well after the first wave (blue triangles), presented in COVID-19 mortality rate quartiles (Q1 being lowest mortality rate). Results are presented as adjusted means or frequencies together with 95% confidence intervals. Linear or logistic regression models were used adjusted for sex, T1D duration, and age. CGM, continuous glucose monitoring; DKA, diabetic ketoacidosis; T1D, type 1 diabetes. Color images are available online.
Adjusted Clinical Parameters of Patients with Type 1 Diabetes <21 Years Compared for the Same Time Period in 2019 and 2020 (May–June) by Country Quartiles According to COVID-19 Deaths
Hierarchical linear and logistic regression models were used to adjust for age (categorized), gender, and diabetes duration (categorized).
Results are presented as estimated mean (interquartile range). COVID-19*time period refers to the P-value of interaction term between time period and COVID-19 cumulative death categories.
A significant joint impact on clinical parameters (DKA, insulin dose, and percentage of pump and CGM use) was present between quartiles of COVID-19 deaths and time period (P-value of interaction term <0.05). Higher COVID-19 burden was also associated with less CGM use and higher daily insulin dose in May/June (Q3 and Q4). After the lockdown (August/September), DKA rates returned to baseline, insulin dose was similar between 2019 and 2020, while CGM use increased significantly in all quartiles of COVID-19 burden (Fig. 1, Supplementary Table S1)
The results on all outcomes remained similar after additional adjustment for the difference in the number of individuals in 2020 versus 2019 (shown for the main outcome (DKA rate) in Supplementary Fig. S2).
Discussion
Corresponding to reports of increased rates of DKA at diagnosis of T1D as a sign of delayed access to care, 13,14 a significant rise in DKA was found among patients with established T1D in the quartile of countries with the highest COVID-19 mortality returning to baseline after the conclusion of the first wave. This may reflect the impact on general health care delivery in these countries. There was a dramatic reduction in pediatric diabetes clinical care in May/June 2020 across the globe, reflecting a widespread trend that did not differ between regions according to COVID-19 mortality. We must prepare now for future societal and global crises that threaten to disrupt routine, outpatient care.
Previous analyses of the SWEET group revealed that before the pandemic at diagnosis of diabetes, 6% of children experience DKA with coma, 37% DKA without coma, and 57% no DKA, with variations between countries. 15 DKA during follow-up is usually associated with poor glycemic control 16 and findings of maintained glycemic control and increased DKA rates may appear counterintuitive. With the dramatic decrease in outpatient clinic attendance and widespread use of telemedicine in 2020, is it possible that there was a bias to measure HbA1c in children with better glycecmic management. However, the present pediatric COVID-19 observations on glycemic control are in agreement with adult data that use of technology allows maintaining glycemic control during the first wave of COVID. 17 –19 In contrast, DKA is an acute complication, and there are reports also from other areas that pediatric patients have been reluctant to seek emergency treatment during the pandemic. 20,21
Differences in glycemic control and use of diabetes technology existed between countries represented by COVID-19 categories before the pandemic, likely reflecting differences in health-care delivery 10 and heterogeneity in reimbursement. 22 The proportion of patients who reported using diabetes technology (insulin pumps and CGM) increased in countries with lower COVID-19 mortality, where pre-COVID use was also lower. This could reflect either the facility of reporting in those newly engaged in technology and/or lacking resources among those dealing with starting and maintaining diabetes technology during high COVID-19 burden. Using technology may have enabled electronic distant review. 2,3 As patients on insulin pumps and CGM generally tend to have better glycemic control than those without, 11 the lower HbA1c during the lockdown would argue against the notion that such patients did not receive clinical care during the pandemic. Inability to receive supplies (CGM, pump, insulin) could cause that, but indications that prescriptions and supplies were disrupted in SWEET centers were not reported.
Likely, the stay-at-home orders led to improvements for some kids (parents more on top of management when they were at home) or worsening for others (lack of exercise, unsupervised time as essential workers left their adolescent children at home, poorer diet choices). A trend toward an increased insulin dose, possibly reflecting a lack of physical exercise or increased eating due to stress, more access to food when doing school from home online during the lockdown, was observed in association with high COVID-19 burden (Q3 and Q4), while insulin dose was similar between 2019 and 2020 in these quartiles in the control period (Fig. 1, Table 3).
Compared to the same period in 2019, fewer patients were reported to the registry in May/June 2020 and in the period August/September 2020, with wide variations between centers. However, the difference between 2020 and 2019 was smaller in the control period August/September compared to May/June. These patterns could suggest both inability to access outpatient care during the lockdowns 23 and/or data collection challenges during the immediate crisis. However, the results on all outcomes remain similar when the calculated difference in the number of individuals in 2020 versus 2019 was added to our main model.
It will be important to examine these questions in subsequent COVID-19 waves. Nevertheless, it may be difficult to validate the present findings with longer follow-up because death rates from COVID-19 did not correlate similarly between countries over the course of the pandemic. Therefore, the categorization into quartiles of COVID-19 death categories might differ substantially over time. Hopefully, the centers were better prepared for subsequent waves, so possibly this association with DKA could be limited to the initial impact of COVID-19. At any rate, it is reassuring that the DKA rates returned to baseline 3 months after the lockdown.
Particularly in those countries with a high COVID-19 mortality, special emphasis should be put on maintaining access to diabetes technology through measures like online pump and CGM starts via telemedicine. 2,3 Reduced restrictions around the use of video conferencing technology for medical care, increasing use of diabetes devices that capture relevant data and can be uploaded remotely, and the increased use of video conference software in daily life will all help promote high quality, remote care. However, these effects may not be as strongly experienced in poorer countries and among socially disadvantaged groups for whom these technologies are not as widely available. It remains to be seen if such measures also would be able to contribute to preventing the rise of DKA observed in those countries with the highest COVID-19 mortality.
Of note, CGM use increased significantly in all quartiles in the months after the lockdown and before the start of the second wave. Possibly the positive experience with telemonitoring and telemedicine during the lockdown has contributed to this. Recent SWEET analysis before the lockdown indicated that lower HbA1c and fewer DKA episodes were observed in subjects using a pump, CGM, or both. 24 The widespread use of diabetes technology in this cohort of pediatric patients with T1D appears associated with the sustained good glycemic control maintained during the first wave of the COVID-19 crisis.
Furthermore, this information may be important for the recent controversy about COVID-19 vaccine prioritization for type 1 and type 2 diabetes. 25 Thus far, this discussion relies almost exclusively on the adult diabetes outcome data. 5,26 –28 In one of the few studies to have analyzed COVID-19 outcomes in children with diabetes, only 8 of 40 patients were younger than 18 years of age, 29 so that the extrapolation of adult data to pediatrics needs to be cautioned. 10 In adults, the risk of fatal or critical care unit-treated COVID-19 is increased by 2.4 times in T1D and 1.4 times in type 2 diabetes. 30 People with recent admissions history for hypoglycemia and diabetic ketoacidosis have an increased risk of severe or fatal disease. 30
Some countries, such as Germany, have therefore categorized people with type 1 and type 2 with an HbA1c ≥7.5% in the prioritization group 3 containing those people with the most serious comorbidities. 31 In the United States, the Centers for Disease Control and Prevention currently categorize type 1 and type 2 diabetes differently in terms of risk for severe illness from COVID-19. 32 So far, vaccines are approved in many countries only for those older than the age of 16 years. If vaccines would be approved for children, these data may argue that children with T1D should also be prioritized. As our data show that this age group is prone to a high risk of the potentially life-threatening acute complication of diabetic ketoacidosis during times of high COVID-19-related burden, this should be recommended even without reference to glycemic control.
Our study has limitations: the two compared periods have partial differences in populations. As participation in SWEET is limited to larger centers with multidisciplinary care, 11 the participating centers cannot be considered representative for a country or region and important information like issues with access to primary care, emergency rooms, or fear of going there as well as problems with availability of insulin, test strips, or possible socioeconomic influences were not available. Nevertheless, this real-world data analysis of the worldwide impact of the COVID-19 pandemic on pediatric T1D indicates that children cared for in large pediatric diabetes centers maintained glycemic control during the challenges of the first wave of the COVID pandemic. Possibly the widespread use of diabetes technology contributed to this. The major concern relates to the observed rise in DKA in those countries with the highest COVID-19 mortality. Future analysis of subsequent waves will elucidate if measures such as the increasing use of CGM in the time after the lockdown prevented a reoccurrence of COVID-19-associated increased DKA rates.
Footnotes
Authors' Contributions
All authors contributed to the study concept and design. T.D. and S.L. supervised the study. S.L. analyzed the data. All authors participated in data interpretation. T.D., M.d.B., and E.T.R. drafted the first version of the article. The final article was reviewed and approved by all. T.D. is the guarantor of the study and takes full responsibility for the work as a whole, including the study design, access to data, and the decision to submit and publish the article.
Acknowledgments
We thank the following for their support of this work: Katharina Fink for the data management as well as Andreas Hungele and Ramona Ranz for the DPV software (all Ulm University, Germany), Katharina Klee (Kinderkrankenhaus Auf der Bult, Hannover, Germany) and Reinhard Holl (Ulm University, Germany) for their invaluable support. Finally, we thank all participating centers of the SWEET network, especially the collaboration centers in this investigation (see ![]() below).
below).
Author Disclosure Statement
T.D. has received speaker's honoraria and research support from and has consulted for Abbott, AstraZeneca, Boehringer, DexCom, Lilly, Medtronic, Novo Nordisk, Roche, Sanofi, and Ypsomed and is a shareholder of DreaMed Ltd. E.T.R. is the Site Principal Investigator for a Phase 3 clinical trial sponsored by AstraZeneca. P.B. has received speaker's honoraria from Sanofi, Novo Nordisk, Lilly, Abbott, and Vitalaire. K.D. has received speaker's honoraria from Abbott, Novo Nordisk, and Sanofi. S.L., M.d.B., G.T.A., Y.E., M.K., B.S., M.S.P., and A.C. declare that there is no duality of interest associated with their contribution to this article.
Funding Information
SWEET is a registered nonprofit charity in Hannover, Germany. It is financed through membership fees of the participating centers (based on income of country of residence according to the World Bank) and corporate members. We acknowledge with gratitude the support from the following SWEET e.V. corporate members—in alphabetical order: Abbott, Boehringer Ingelheim, DexCom, Inc., Insulet, Eli Lilly & Co., Medtronic Europe, Sanofi.
Supplementary Material
Supplementary Table S1
Supplementary Figure S1
Supplementary Figure S2
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.