
Abstract
Objective:
To investigate whether telemetric continuous glucose monitoring (CGM) in hospitalized and isolated patients with diabetes mellitus and coronavirus disease 2019 (COVID-19) is associated with better glycemic outcomes and fewer patient health care worker contacts compared to blood glucose monitoring by traditional point-of-care (POC) glucose testing and to investigate the user aspect of implementing a CGM-system in-hospital.
Materials and Methods:
A randomized controlled exploratory trial was performed on hospitalized and isolated patients with diabetes and COVID-19 from May 2020 until February 2021 at Nordsjællands Hospital, Denmark. Participants were randomized to nonblinded telemetric CGM (as the only glucose monitoring method) or traditional POC glucose testing + blinded CGM. The primary endpoint was time in range (TIR) based on CGM data in both groups. A questionnaire about the user aspect of the CGM system was answered by health care personnel (HCP).
Results:
We included 64 participants in the analysis, 31 in the CGM group and 33 in the POC glucose group. TIR median was 46% for the CGM group and 68% for the POC glucose group (P = 0.368). The mean glucose value for the CGM group was 11.1 and 10.8 mmol/L in the POC glucose group (P = 0.372). CGM was associated with fewer POC glucose measurements (P < 0.001). Out of 30 HCPs, 28 preferred telemetric CGM over POC glucose testing.
Conclusion:
Remote glucose monitoring by CGM did not improve glycemic outcomes compared to traditional POC glucose testing, but was associated with fewer patient-personnel contacts, saving time for HCPs performing diabetes-related tasks. Most HCPs preferred CGM. The study is registered at
Introduction
Continuous glucose monitoring (CGM) is a widely used technology for patients with diabetes in the out-patient setting, providing information on glucose values and fluctuations for optimizing glucose control. CGM is at present primarily used in people with type 1 diabetes (T1DM) and is associated with improved glycemic outcomes, 1,2 but the use of CGMs in hospitalized patients is still experimental. Most studies on CGM for inpatient use have been performed in the intensive care unit (ICU) setting, and only a few studies have described the usage and efficiency of CGM in non-ICU settings. These studies focus on validating the CGM systems' performance and less on the effects on glycemic variables. 3 In general, they show no difference in mean glucose levels when using CGM compared to capillary glucose by point-of-care (POC) glucose testing, although the risk of hypoglycemic events is minimized. 3 –5
In 2019, the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) causing coronavirus disease 2019 (COVID-19) emerged. Due to the COVID-19 pandemic and the transmission risk associated with each procedure with an isolated COVID-19 patient, the use of in-hospital CGM has had a new incentive. Thus, the FDA has approved the temporary use of noninvasive remote monitoring devices, including CGMs, for patients with COVID-19 in the in-hospital setting. 6 CGM could potentially improve the treatment of diabetes in isolated patients and reduce the amount of time spent on bedside glucose monitoring and the risk of transferring contagious infections. Recent studies have shown that being hospitalized with COVID-19 and diabetes is—compared to people without diabetes—associated with a two to three times greater risk of transferal to the ICU, more severe illness such as acute respiratory distress syndrome, and greater risk of in-hospital death. 7 –10 In a recent meta-analysis, diabetes was the most important risk factor for mortality in patients hospitalized with COVID-19. 11 Furthermore, it is known that in-hospital hyperglycemia and hypoglycemia are associated with increased all-cause mortality and morbidity. 3,12 Thus, it is suggested that glucose levels should remain between 4 and 10 mmol/L during hospitalization. 13 Such a goal requires frequent glucose measurements that can be time-consuming, especially when health care personnel (HCP) must use personal protective equipment (PPE) and spend time on cleansing procedures to reduce the risk of spreading infectious particles. A way of reducing this risk might be by using telemetric CGM to transmit glucose data from the patient to a remote surveillance unit outside the patients' room. Finally, more detailed information on glucose trajectories during hospitalization could potentially lead to better clinical decisions on glucose-lowering therapy, thereby improving glycemic outcomes during hospitalization.
The aim of this study was to investigate whether telemetric CGM in hospitalized and isolated patients with diabetes mellitus and SARS-CoV-2 is associated with better glycemic outcomes and fewer HCP contacts compared to blood glucose monitoring by traditional POC glucose testing. Furthermore, to investigate the user-aspect of in-hospital CGM rated by HCPs.
Materials and Methods
Design
A randomized controlled trial was performed in hospitalized isolated patients with diabetes and confirmed COVID-19 from May 2020 until February 2021 at Nordsjællands Hospital, Hilleroed, Denmark. Patients were recruited from three wards, including the Ward of Pulmonary and Infectious Diseases, the Ward of Endocrinology and Nephrology, and the Ward of Cardiology. Participants were randomized to either nonblinded CGM with data accessed remotely or by POC glucose testing in addition to blinded CGM.
The study was approved by the Regional Committee on Biomedical Research Ethics (#H-20025305) and the Danish Data Protection Agency (#P-2020-303). The trial protocol has been published. 14
Inclusion and exclusion criteria
Patients who fulfilled the following criteria were eligible: People 18 years of age or older, hospitalized with confirmed SARS-CoV-2 infection by real-time PCR (oropharyngeal swab or sputum from the lower respiratory tract), in isolation at the time of inclusion, and a history of diabetes or newly discovered diabetes (during hospitalization) according to WHO recommendation on diagnostic criteria for diabetes. 15 The participants had to be able to communicate with the study personnel and willing and able to comply with the trial protocol. Exclusion criterion was known hypersensitivity to the Dexcom G6 sensor band-aid.
Patients were followed until discontinued isolation, discharge, or transferal to the ICU or other wards not included in the study. Patients with less than 24 h of CGM data were excluded from the analysis.
Identification, informed consent, and randomization
Trough daily screening of patient lists in the participating wards, we identified patients with T1DM, type 2 diabetes (T2DM), New-Onset Diabetes After Transplantation, gestational diabetes, newly discovered DM (not yet classified), and secondary diabetes.
Patients received verbal and written information about the study, and written consent was obtained before any trial-related procedures were performed. Participants were randomized 1:1 into two groups according to randomization lists generated by
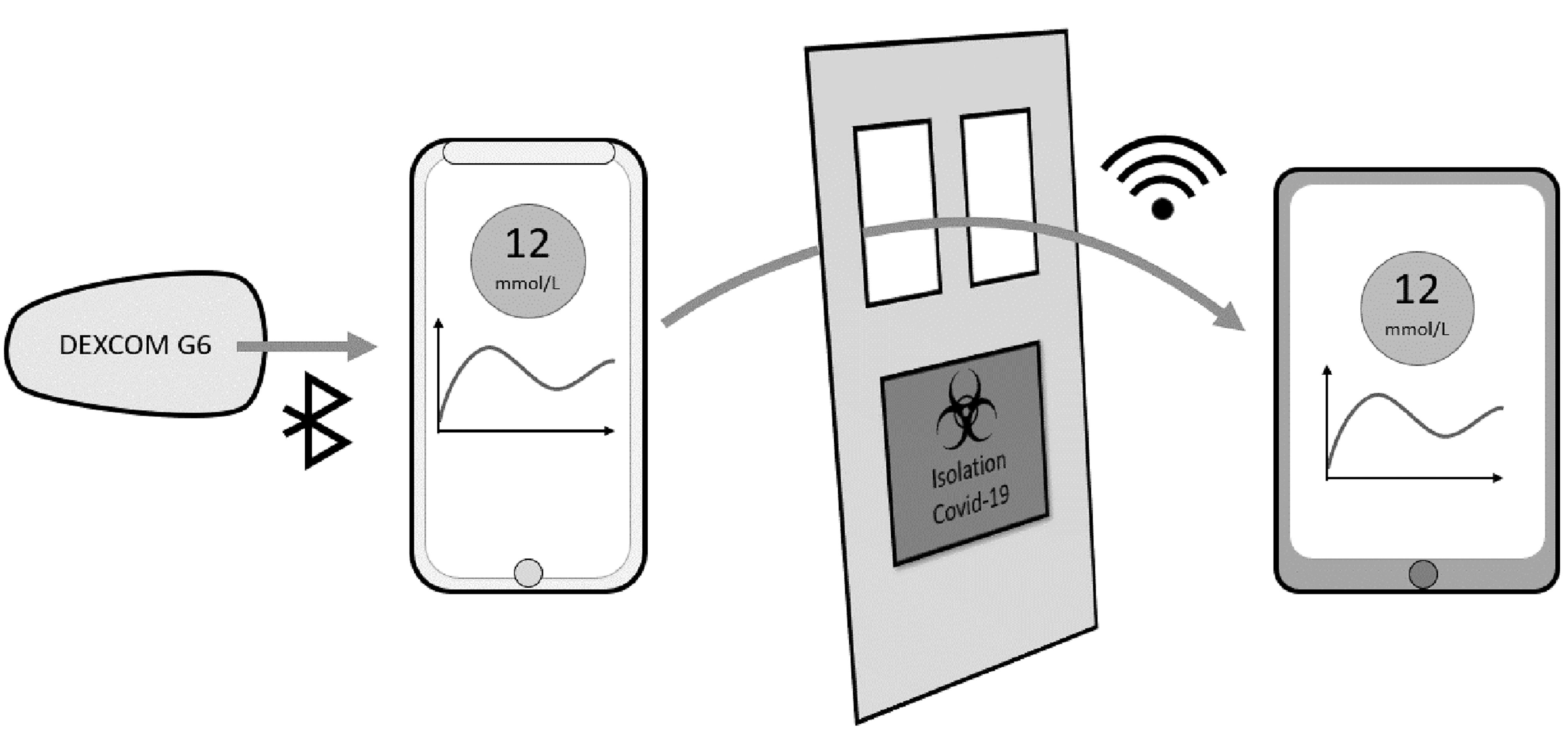
Technical setup of the study. The CGM is mounted on the patient and the glucose data are transmitted via Bluetooth to a smartphone in the patient room. In the nonblinded group, the glucose data were also transferred via. WIFI to a tablet at the HCPs' office. CGM, continuous glucose monitoring; HCP, health care personnel.
Materials
The CGM system consisted of a Dexcom G6 (Dexcom, Inc., San Diego, USA) sensor, which can last for ∼10 days and a Dexcom G6 transmitter (battery time of 3 months). We used an iPhone 7 (Apple, Inc., Cupertino, USA) to connect with the Dexcom G6 app and an iPad 7 (Apple, Inc.) in the HCP's office for remote monitoring. The Dexcom G6 system was inserted on the abdomen and measures interstitial fluid glucose values every 5 min and did not need to be calibrated, although it requires a 2-h warm-up period after insertion before data collection can begin. No extra POC glucose measurements were done during the 2-h warm-up period. Due to insufficient testing, the Dexcom G6 is not approved to wear during magnetic resonance imaging (MRI) or computed tomography (CT) scan. The CE Marking confirms that the Dexcom G6 system meets the Essential Requirements of the Medical Device Directive MDD 93/42/EEC as amended by 2007/47/EC. Data were transferred automatically from the Dexcom G6 app on the iPhone 7 to a glucose data system (Diasend® by Glooko).
Diabetes management
The participants' diabetes was managed by usual care at the discretion of nurses and medical doctors at the different departments. Usual care includes an option to call specialized nurses trained in diabetes management at the Department of Endocrinology and Nephrology. The investigators were not involved in the management of diabetes.
Technical support
In the CGM group, nurses were instructed to use the iPad at their office to replace POC glucose testing. Furthermore, all nurses were instructed to remove the Dexcom G6 in case of discharge, CT, or MRI scan or transfer to other wards than the four wards included in this study. The investigators turned off all audible threshold alarms on iPads and iPhones in both the blinded and nonblinded CGM group except for one mandatory threshold alarm (set by Dexcom) for acute hypoglycemia ≤3.1 mmol/L (≤56 mg/dL).
Data collection
Clinical data collection
Clinical and demographic variables registered from medical records included age, gender, ethnicity, body mass index (BMI), blood pressure and pulse at inclusion, glycated hemoglobin, plasma glucose, C-reactive protein, and POC capillary glucose. Comorbidities such as hypertension, cardiovascular disease, diabetic complications (micro- and macrovascular diseases), chronic obstructive pulmonary disease, and cancer were registered. Further, glucose-lowering medication before admission and corticosteroid therapy before and during admission was registered. Data regarding insulin administration were also registered.
Time spent on PPE
The investigators measured the time spent putting PPE on and off by observing primarily nurses experienced in handling PPE during their work. HCPs were instructed to act as usual to make the time-measurements as true to reality as possible. PPE included gown, gloves, filtering face-piece respirators mask (FFP3 NRD), and face shield. Data were collected throughout the inclusion period.
User satisfaction of telemetric CGM
A user satisfaction survey about telemetric CGM was developed as a nine-point questionnaire, including three optional explanatory comment sections, and distributed to the HCPs that participated in patient care in the present study after the study was completed. The nine-point questionnaire was validated through reviewing by two independent parties followed by a pilot test on a subset of HCPs. During the data collection process, answers were checked for cohesion between answers to positively phrased and negatively phrased questions and found consistent.
Primary endpoint
The primary endpoint was time in range (TIR), defined according to international standards for outpatients 13 and measured as the percentage of time per day within glucose range of 3.9–10.0 mmol/L (70–180 mg/dL). TIR was calculated as a mean percentage of the isolation period wearing active CGM and is reported for full days as well as for night (23; 07) and day (07; 23) separately. Furthermore, the number of periods patients had 24 h continuously with 100% of glucose values in TIR are reported.
Secondary endpoints
Secondary endpoints included additional glucose outcomes based on CGM data such as time above range (TAR) defined as glucose values >10.0 mmol/L (>180 mg/dL), time below range (TBR) defined as glucose values <3.9mmol/L (<70 mg/dL), median, interquartile range (IQR), mean, glycemic variability reported as the coefficient of variation (CV), and standard deviation (SD). Dexcom G6 does not display glucose values above 22.2 mmol/L or below 2.2 mmol/L. Therefore, estimates of the mean, median, CV, and SD were based on an imputation model for the censored values. The number of POC glucose tests in the two groups were reported and used to estimate the number of saved patient-personnel contacts in the CGM group.
Furthermore, we report the mean number of times correction insulin was administered during the inclusion period, sensor performance as hours with “no data” in total, in-hospital death, length of hospital stay (days), need of respiratory support, intensive care, and patient status after 60 days.
Tertiary endpoints
Time spent putting on and taking off PPE and the results from the HCP questionnaire for categorical questions—the three optional explanatory comment sections—are not reported but will be available on reasonable request.
We report the number of hypoglycemic events defined according to the current international consensus as level 1 with glucose values ≤3.9 mmol/L (≤70 mg/dL) for 15 min or more, level 2 < 3 mmol/L (<54 mg/dL) for 15 min or more, and level 3 as severe hypoglycemia requiring external assistance for recovery. 16
When correction insulin was prescribed (usually five times a day), a nurse had to decide whether to administer insulin or not and if so at what dosage, based on the glucose readings at that given time from either CGM or POC glucose testing. We report, in mean percentage, how often a correct decision was made in each group and compare them. We also report if dosage of correction insulin was prescribed correctly based on participants' weight. Incorrect decisions were defined as not administering insulin when needed or as administering an incorrect dosage in relationship to the insulin regime prescribed. Calculation of correct decisions was based on the prescribed units of correction insulin.
Statistical analysis
A preplanned sample size analysis based on the primary endpoint showed that a total of 62 patients should be included to detect a 10% difference in the primary endpoint with a SD of 14 (based on data from our research group and previous studies) to obtain a power of 80% with a type I error of 5.0%. With an expected drop-out rate of 15%, we planned to include 72 patients. This was achieved with a total of 64 patients included for the primary analysis.
All analyses were based on participants with ≥24 h of CGM data, and only data from the period of isolation was analyzed. Between-group comparisons were performed by Wilcoxon rank-sum test or independent t-test for continuous variables and chi-squared test or Fischer's exact test for categorical variables. Assessments of normality were performed by visual inspection of histograms and QQ-plots. The threshold for statistical significance was set to P = 0.05, and statistical tests were all two-sided. Secondary outcomes were adjusted for multiplicity by the Bonferroni method.
The Dexcom G6 sensor has an upper detection limit of 22.2 mmol/L. Hence CGM trajectories for participants with measurements above that value will be right censored. As right censoring leads to a downward bias, a nonparametric imputation model for the censored values was performed. The complete trajectories for all participants having censored observations were modeled by latent Gaussian Processes with the Matern 5/2 covariance function. 17 The likelihood of each CGM observation was modeled by independent normal distributions conditional on the latent process contributing with the density function for the observed values and the survival function for the censored values. The posterior mean of the latent process was used in the subsequent analyses. Zero mean half-t distributions with three degrees of freedom and a variance of 2.5 were used as priors for the variance and length scale parameters of the latent process and the residual variance of the observations. The model was implemented in TensorFlow Probability 18 and fitted using Hamiltonian MCMC with four parallel chains and 5000 iterations for each.
The daily CGM mean and IQR profiles for each group were estimated by a regression model using the Box-Cox Cole and Green distribution 19 with cyclic cubic P-splines for each of the three parameters.
Validation of the imputation model
Figure 2 (left) shows an example of a CGM trajectory from a participant featuring right censoring and the associated posterior mean and 95% posterior probability interval. To validate the imputation model for the censored CGM observations, we compared the imputed values to POC glucose measurements taking at the same time. For each participant with censored CGM values, we identified all time points during admission where a simultaneous POC glucose was taken. Figure 2 (right) shows a scatter plot of these simultaneous POC glucose and CGM measurements against each other. Fully observed pairs are shown as circles, pairs with a censored CGM measurement are shown as black squares, and red squares show the corresponding imputed CGM values (95% posterior probability intervals shown as vertical lines). The dashed black line shows the identity line (slope = 1) corresponding to perfect agreement on average. Fitting a linear regression line using the censored observations gave a slope of 0.795 (95% confidence interval [CI] = [0.710–0.880]), while a linear regression fitted to the imputed observations (shown as the red line) gave a slope of 0.984 (95% CI = [0.953–1.021]).

The left panel shows a random example of the observed CGM data from a single participant and the imputed censored values. The right panel shows the agreement between the imputed CGM values and POC glucose measurements taken at the same points in time. POC, point-of-care.
Results
From May 13th, 2020, until February 8th, 2021, we identified 165 patients admitted to Copenhagen University Hospital—North Zealand with both diabetes and COVID-19, requiring isolation. Eighty-eight patients fulfilled all inclusion- and no exclusion criteria and signed the informed consent form. Forty-eight were randomized to the CGM group and 40 to the POC glucose group. One patient withdrew consent before the CGM was mounted. Figure 3 illustrates a flowchart of enrollment of participants and how many eligible participants we excluded due to discharge, discontinued isolation, uncertainty about DM diagnosis, communication barriers, and so on. Sixty-four patients were included in the final analysis (34 in the CGM group and 30 in the POC glucose group). Baseline characteristics can be seen in Table 1. In total, the number of days the patients were hospitalized and included in the study was 924 days. The excluded participants did not differ from included participants in relationship to age, gender, BMI, DM type, or comorbidities (data not shown).
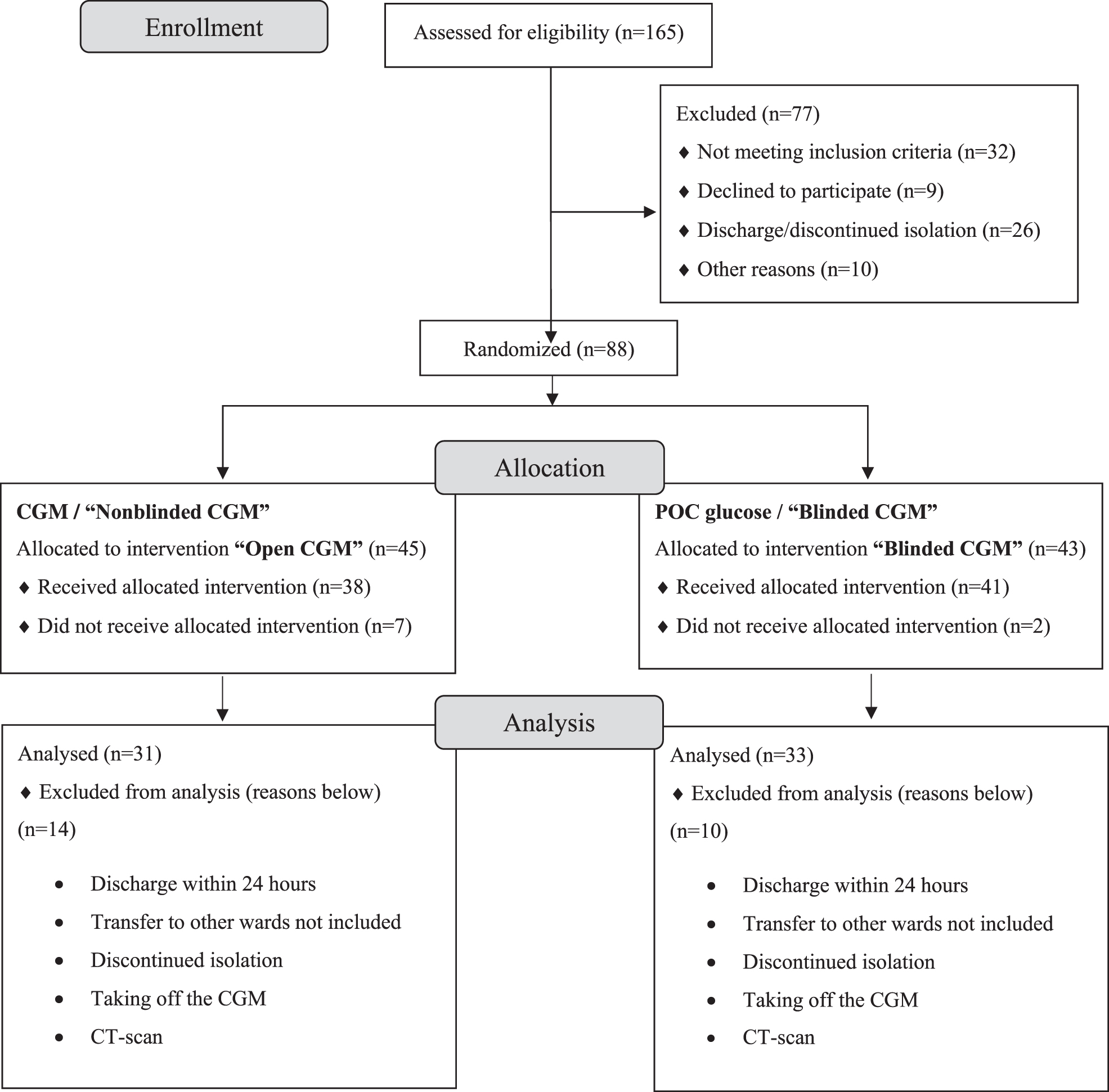
Flowchart diagram of enrollment of participants. CT-scan, computed tomography scan.
Demographic and Clinical Characteristics of Participants Included in the Final Analysis in the Nonblinded Continuous Glucose Monitoring Group and Blinded Continuous Glucose Monitoring/Point-of-Care Glucose Group at Baseline
Bold values represent statistically significant P-values.
BMI, body mass index; CGM, continuous glucose monitoring; COPD, chronic obstructive pulmonary disease; CVD, cardiovascular disease; HbA1, hemoglobin A1c; NODAT, New-Onset Diabetes After Transplantation; P-glucose, plasma glucose; POC, point-of-care; SD, standard deviation.
In the CGM group, 54.8% were males compared to 66.7% in the POC glucose group. The median age (range) was 76 (30–93) years in the CGM group and 72 (43–91) years in the POC glucose group. The POC glucose group had a statistically significant higher BMI than the CGM group (P = 0.029). No significant differences were found between the two groups regarding other baseline characteristics. Most patients in both groups had T2DM (67.7% in the CGM group and 69.7% in the POC glucose group), and most patients were taking antidiabetic medications before admission (64.5% in the CGM group and 66.7% in the POC glucose group). A high number of patients received glucocorticoids (GC) during admission primarily due to COVID-19 treatment protocols 20 (83.9% in the CGM group and 69.7% in the POC glucose group).
Primary endpoint
We did not find a difference in TIR between the groups. In the CGM group TIR median (Q1, Q3) was 46% (15%, 75%) and in the POC glucose group 68% (14%, 84.5%) (P = 0.368) (Table 2).
Primary, Secondary, and Tertiary Outcomes
Significant values in bold.
Other than nasal oxygen.
ICU, intensive care unit; TAR, time above range; TBR, time below range; TIR, time in range.
The number of 24 h periods 100% in TIR for all patients together were 32 (11 in the CGM group in 5 participants and 21 in the POC glucose group in 10 participants [P = 0.948]).
Secondary endpoints
The results for all secondary endpoints are shown in Table 2. In the CGM group, median (Q1, Q3) TAR was 52.0% (24.0%, 85.0%), and for the POC glucose group, 31% (15.5%, 86.0%) (P = 0.386). Median TBR (Q1, Q3) in the CGM group was 0.0% (0.0%, 0.0%) and for the POC glucose group, 0.0% (0.0%, 0.5%) (P = 0.603) (Table 2). The median of mean glucose (Q1, Q3) for the CGM group was 10.7 (8.6, 13.6) mmol/L and for POC glucose group, 8.7 (8.1, 13.6) mmol/L (P = 0.372). Glucose daytime mean (SD) in the CGM group was 11.9 (3.3) mmol/L and 11.3 (2.7) mmol/L in the POC glucose group (P = 0.309). Glucose nighttime mean (SD) in the CGM group was 9.7 (2.4) mmol/L and 9.7 (2.0) mmol/L in the POC glucose group (P = 0.603). Mean (IQR) glucose values during day and night for the CGM group and the POC glucose group are illustrated in Figure 4, right panel. The glycemic variability reported as CV mean (SD) was 29.8% (10.7%) in the CGM group and 25% (9.3%) in the POC glucose group (P = 0.047). After adjusting for multiplicity, this result was no longer significant. The median of SD (Q1, Q3) for the CGM group was 3.1 (2.2, 3.7) and for the POC glucose group, 2.3 (1.6, 3.1) (P = 0.013). After adjusting for multiplicity, this result was no longer significant. There was a statistically significant difference between the groups in the number of POC glucose tests per day with a median (Q1, Q3) in the CGM group of 0.6 (0.0, 1.1) and 3.0 (2.5, 4.6) for the POC glucose group (P < 0.001) that was still significant after adjusting for multiplicity. There was no difference between the groups regarding the length of stay, need for respiratory support, admission to ICU, in-hospital death, or 60-day survival (Table 2).

Imputed CGM data for each calendar day for all 64 participants hospitalized with diabetes and COVID-19 infection randomized into the CGM (left) and POC glucose (middle) groups. The right panel shows the mean and IQR. COVID-19, causing coronavirus disease 2019; IQR, interquartile range.
Hypoglycemic events
Based on CGM readings, there was a total of 44 hypoglycemic events in the CGM group, whereas the POC glucose group had 40 hypoglycemic events (P = 0.156). In both groups, there were five level 2 events and no level 3 events. In the POC glucose testing group only 50% (20 events) were also caught on POC glucose measurements.
Correction insulin administration
There was no difference in the frequency of correction insulin administration between the groups (P = 0.163). A correct decision regarding administration of correction insulin was made in the CGM group in median (Q1, Q3) 79.0% (65.8%, 87.3%) of times and in the POC glucose group in 92.9% (71.4%, 100.0%) of times (P = 0.034). Participants had a correct dose of insulin prescribed in 57.8% of times, 18.8% had an incorrect dose prescribed (4.7% too high and 14.1% too low), 12.5% had correction insulin prescribed without any weight documented, and 10.9% did not have any correction insulin prescribed at all.
Time spent on PPE
These calculations are based on 46 observations. Mean (range) time spent putting on PPE was 1.9 (1.2–3.2) min and mean (range) time spent taking off PPE was 1.7 (0.5–2.8) min. The mean time spent on PPE was 3.6 min. The number of POC glucose tests mean (SD) per day was 3.5 (1.5) in the POC glucose group and 1.0 (1.2) in the CGM group (P < 0.001). Thus, in the CGM group, the personnel did 2.5 fewer POC glucose tests per day, translating into a potential to save ∼9 min spent on PPE per day per patient from remotely monitoring glucose with CGM instead of POC glucose testing (Table 3).
Time Spent on Personal Protective Equipment When Visiting Coronavirus Disease 2019 Positive Isolated Patients
Values collected throughout the pandemic, primarily on experienced HCPs used to handle PPE in the Ward of Pulmonary and Infectious Diseases.
COVID-19, coronavirus disease 2019; HCP, health care personnel; PPE, personal protective equipment.
User satisfaction of telemetric CGM
A total of 30 HCPs answered the user satisfaction questionnaire, and 100% of the questionnaires were completed. The mean number of individual patients that an HCP had cared for in the study period was 5.2 (range 2–15). Two HCPs answered that they had cared for “>15” individual patients and thus were not included in calculating the mean for this single question. The mean number of patients an HCP had cared for in the CGM group was 3.8 (range 1–15). The overall satisfaction level with the CGM system was high. Despite some reported CGM-system difficulties (lost signal, iPad problems), 28 out of 30 preferred to use a telemetric CGM system over the standard POC glucose testing method. Twenty-eight out of 30 rated that the CGM system had made their work easier (Fig. 5).
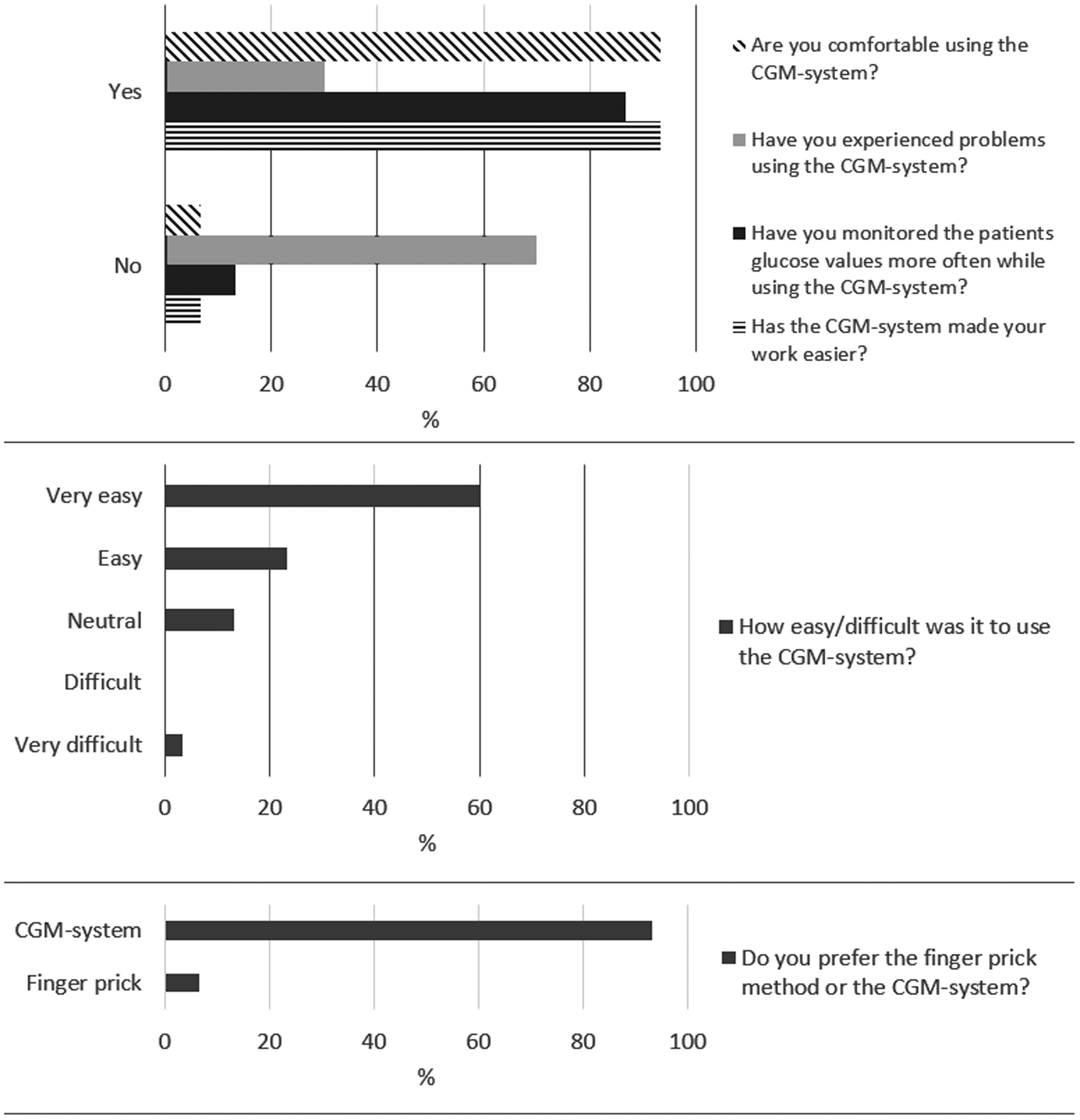
Bar charts showing results from 30 HCPs' answers to a CGM-system user satisfaction questionnaire. Explanatory comments not shown. Results are shown in percentage of participants.
Discussion
In this randomized study, we investigated whether telemetric CGM in hospitalized and isolated patients with DM and COVID-19 was associated with better glycemic outcomes and fewer patient-HCP contacts than blood glucose monitoring by traditional POC glucose testing. We found that implementing remote glucose monitoring with CGM is possible and with high user satisfaction rated by HCPs. We also reported a reduced number of patient contacts with the purpose of measuring glucose. We did not find any difference in glycemic variables between patients being monitored remotely with CGM or by POC glucose testing. Although we did not find a difference in hypoglycemic events between the groups based on the CGM readings in this study, we found that 50% hypoglycemic events were missed by POC glucose testing alone.
Two recent reviews describe eight non-ICU CGM studies, all focusing on validating CGM systems during hospitalization. 3,5 Both show that CGM systems are precise during hospitalization and improve detection of hypoglycemic events but state the lack of randomized nonblinded CGM studies investigating whether CGM can improve hospitalized patients' glycemic outcomes. Recently, the first randomized controlled study in insulin requiring patients with T2DM hospitalized in non-ICU ward investigating the effect of real-time CGM compared to standard POC glucose testing found that there was better glycemic outcomes in the CGM group. 21 The set-up included activation of hyper- and hypoglycemic alarms, a standardized insulin protocol (discontinuation of previous antidiabetic medications at inclusion) and monitoring of CGM trends by an advanced practice nurse that collaborated with doctors to optimize therapy in the CGM group only. However, confirmatory POC glucose testing was also performed before insulin administration in the CGM group. A pilot study in non-ICU settings in 2018 found an improved TIR with nonblinded CGM (TIR for blinded CGM 54% and TIR 69% for nonblinded CGM), although they did not reach statistical significance due to small sample size (n = 16). 4 In contrast to our study, they used audible alarms to inform HCP when glucose values deviated from euglycemic levels, contributing to the positive effects on TIR when using nonblinded CGM.
The use of alarms and/or support by specialized staff may explain why these studies were able to show an effect in contrast to ours, which did not use alarms, systematic education, or specialist assistance and did not have a study-related treatment protocol. Thus, the implementation of CGM cannot stand alone, but needs to be supported by optimized treatment decisions. On the contrary, this real-life study was a direct comparison of CGM versus POC glucose without the addition of other interventions. Other smaller studies have previously confirmed the feasibility of using CGM for hospitalized patients with COVID-19. 22,23
Glucose data from our study, including TIR, TAR, and mean and median glucose, show that the glycemic outcomes, in general, were poor during hospitalization. In a large retrospective observational study, Bode et al. also found that hospitalized patients with diabetes and COVID-19 had poor glycemic outcomes with only 59.9% of blood glucose measurements in the euglycemic range (n = 451). 24 The variation of glucose levels during the day was, as expected, higher during the daytime (higher intake of carbohydrates) and lower during nighttime. Treatment with GCs could also have influenced the variation as the effect of GCs on glucose values usually wears off during the night if the GC is prescribed in the morning. 25 However, a post hoc analysis in this study showed no statistically significant difference in TIR between patients with or without GC treatment between groups. Hyperglycemia is associated with poor outcomes in hospitalized patients with infections, including pulmonary infections. 26
In this study, HCPs were instructed to use the CGM data in the CGM group instead of POC glucose measurements. In the user satisfaction survey, the HCPs stated that they looked at the tablet with CGM data on it more often than they would have done a POC glucose test; however, correction insulin was not administered more often. We found that there was a significant difference in the percentage of correct decisions made regarding correction insulin administration in the two groups, where nurses more often made a correct decision in the POC glucose group. This could have influenced the results of the glycemic outcomes in favor of better regulation in the POC glucose group. The reason for administering less insulin in the CGM group is unclear. A potential explanation is that HCPs in the wards were less familiar with CGM data and thereby less comfortable with administering full insulin doses. This deserves further attention in future studies.
Using telemetric CGM was, as expected, associated with fewer POC glucose tests. The POC glucose tests per day were two to three doubled in the POC glucose group compared to the CGM group. Thus, telemetric CGM has the potential to save time from HCPs' workload, save PPE resources, and potentially reduces the spread of infectious particles in the hospital. Considering 3.6 min spent on PPE when visiting an isolated patient means that HCPs could save up to 9 min/day per isolated diabetes patient if CGM is used instead of POC glucose testing and if the HCP does not have other reasons to go in the patient room. If local guidelines were followed more strictly with five daily glucose measurements, this could save up to 18 min of HCPs' time on PPE per diabetes patient. In addition, time consumption for the actual POC glucose measurement and cleansing procedures should be taken in account, but so should time to mount the sensor and time spent documenting sensor values in the electronic patient journal. These findings are important as time sparing for HCPs is crucial during a pandemic situation.
Strengths and limitations
The strength of this study is the high number of participants (compared to earlier studies), the randomized design, and the use of clearly defined and clinically relevant endpoints. However, our study has some limitations, including not using CGM alarms and not providing a treatment protocol. This could minimize the chance of detecting the full potential of in-hospital CGM.
Conclusion
This study demonstrated that remote monitoring of glucose by use of CGM, without alarms, as a stand-alone intervention in hospitalized isolated patients with diabetes and COVID-19 has the potential to reduce workload and is preferred by HCPs but did not improve glycemic outcomes compared to traditional glucose measurements by POC glucose testing. The addition of GCM alarms and education of HCPs may improve glycemic outcomes. Larger studies investigating the impact of CGM combined with other interventions to optimize the effect of the technology on glycemic outcomes for hospitalized people with diabetes are needed.
Footnotes
Acknowledgments
We thank research nurse Charlotte Irene Hansen for the invaluable help regarding data entry. We thank Glooko for providing Diasend® free of charge during the study period.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author Disclosure Statement
C.K.K., N.A.W., M.T.O., A.K.J., B.L., and A.M.D. have no competing financial interests exist. U.P.-B. has served on advisory boards and received lecture fees from Novo Nordisk and Sanofi. P.L.K.: has received speakers fee from Sanofi A/S, Novo Nordisk A/S and AstraZeneca A/S.
Funding Information
The Novo Nordisk Foundation (Grant No. NNF20SA0062872) and Grosserer L.F. Foghts Foundation provided funding for the study.