
Abstract
We retrospectively evaluated outcomes of the Minimed Medtronic 670G system in an academic urban safety-net population of adults with type 1 diabetes, between September 2016 and January 2020. Among 32 patients prescribed the 670G, the majority were female (69%), white (69%), achieved advanced degrees (56%), were commercially insured (94%), and were experienced pump users (84%). Patients who initiated auto-mode demonstrated significant improvement in A1c after 1 year. However, 31% of patients never initiated auto-mode. Black and Hispanic patients comprised 50% of this group, despite similar insurance coverage, diabetes duration, educational level, and prior pump use. Hence, traditional barriers to technology use do not explain these racial/ethnic disparities. Of 22 patients who initiated auto-mode, 5 discontinued within 1 year. The most common reason for discontinuation was frustration with pump–sensor interactions. Future studies identifying barriers to and strategies for increasing use of advanced insulin delivery systems in underserved populations are needed.
Introduction
Hybrid closed-loop automated insulin delivery systems are available as a safe and effective means to improve glycemic outcomes in people living with type 1 diabetes (T1D). However, there is still a paucity of data on the benefit of these insulin delivery systems in underserved patient populations. Boston Medical Center (BMC) is an academic safety-net hospital in Boston, MA. Approximately 60% of our patients are from underserved populations, including racial/ethnic minorities and public insurance beneficiaries. 1 The adult T1D population cared for in the endocrinology clinic includes about 500 patients, of which ∼50% are public insurance beneficiaries.
In line with the reported increasing utilization of diabetes technologies in the United States, 2 adoption of technologies, including continuous glucose monitors (CGMs) and insulin pumps, has been growing in our population, but is still underutilized in the majority of our patients. 1 Given previous reports of improved glycemic control, despite well-documented patient and device interaction challenges, 3 we were interested in evaluating the clinical outcomes of the first widely available hybrid closed-loop insulin delivery system, the Minimed Medtronic 670G system (670G), in a demographically diverse adult T1D population cared for in an academic urban safety net endocrinology clinic.
Methods
We conducted a retrospective observational study, enrolling adult patients (>18 years old) cared for in the BMC endocrinology clinic who were prescribed the 670G between September 2016 and January 2020. We included patients who were shipped the 670G, but did not initiate personal use, despite receipt of the device components, to understand possible barriers to successful initiation. This study was approved by the Boston University Medical Campus Institutional Review Board.
We collected clinical data from the electronic medical record (EMR), which specifically included age, diabetes duration, highest education achieved, race/ethnicity, health insurance type (public vs. commercial), number and type of endocrine clinic visits within 1 year of 670G prescription (physicians, diabetes educators, other providers), total time spent on each visit as documented in the clinical notes, prior pump and/or CGM systems used before initiation of the 670G, baseline A1c (within 6 months before initiating 670G), A1c at 6 and 12 months, mean sensor glucose, time spent in target glucose range (70–180 mg/dL), and percentage time spent in “auto-mode” at the last available clinic visit before chart access.
When data were not available from the EMR, Medtronic CareLink was remotely accessed when possible, to supplement these data. We also reviewed the clinician documentation in all endocrinology clinician notes with particular focus on documentation related to patient perception, satisfaction, or challenges with the system.
Our clinical outcomes of interest were reasons for discontinuing use of the system, differences between A1c and sensor glucose metrics at baseline and at 1 year in those who started auto-mode, in comparison with those who discontinued at any time after initiation within the first year, the impact of demographic factors on system initiation and discontinuation and whether time spent in clinical encounters influenced glycemic outcomes or likelihood of success with the 670G.
The data were analyzed and visualized using Microsoft Excel. Qualitative and quantitative measures were compared for (1) patients who started auto-mode versus patients who never started and (2) patients who discontinued auto-mode within the first year after starting versus patients who continued. We summarized quantitative variables using means and standard deviations, compared differences with two-tailed, two-sample t-test (with a 0.05 significance level). Chart documentation with regard to patients' reflection on their 670G experience reasons for not starting auto-mode and discontinuation over the follow-up period were recorded and coded for qualitative analysis.
Results
In the overall cohort, there were twice as many female (n = 22) as male patients (n = 10), and the majority were white (n = 22, 69%). Table 1 displays the demographic characteristics of our cohort. Thirty-two patients received the 670G but only 22 patients (69%) initiated auto-mode. Hispanic (16%) and black (16%) patients were in the minority, despite constituting 60% of our patient population with T1D. The mean age of study participants was 36 ± 8.59 years and the mean duration of diabetes was 20 ± 6.9 years, without significant differences between patients who never started auto-mode and those who initiated auto-mode (Table 1).
Demographic Background Among All Study Participants, Participants Who Never Started Auto-Mode and Who Started Auto-Mode
SD, standard deviation.
In addition, 18 of the 32 patients (56%) had achieved an advanced educational degree (defined as master's and/or doctoral level) and the vast majority of patients were not first-time pump users (n = 27, 84%). The majority (n = 30, 93.75%) were supported by commercial health insurance. When comparing the two groups (starting auto-mode vs. not starting) there were important differences in demographic characteristics between them. There was a higher percentage of white (77% vs. 50%) and highly educated patients (59% vs. 50%) in the group who initiated auto-mode. There was also a higher mean baseline A1c in the group who did not start auto-mode (A1c 8.58 vs. 7.60).
Patients who successfully initiated auto-mode spent more time in pump education on average (total minutes spent with CDCES, 139 vs. 90 min) without any difference in the total number of pump education visits, average duration of endocrinologist visits, or total combined endocrinology clinical visits (physicians/nurse practitioners and diabetes educators). Patients who started auto-mode demonstrated a significant improvement in A1c at 1 year follow-up, whereas those who never started auto-mode demonstrated worsening A1c over the same period (1-year A1c 7.11 vs. 9.10, P = 0.0212), despite similar time spent in CDCES clinical care before pump initiation (total minutes spent with CDCES, 40.31 vs. 40.18).
Of the 22 patients who initiated auto-mode, 5 patients discontinued auto-mode in the 1 year follow-up period, despite more time spent on pump education (183 vs. 123 min) and similar average pump education visits (2.7 visits vs. 2.5 visits). Importantly, A1c and sensor-derived glucose metrics improved in those who continued in auto-mode (mean A1c at baseline vs. 1-year, 7.08 vs. 7.47), as well as those who discontinued before 1-year follow-up (mean A1c at baseline vs. 1-year, 8.14 vs. 7.20.) Figure 1 shows that significantly more white patients started auto-mode and completed 1 year of ongoing use, in comparison with nonwhite patients.
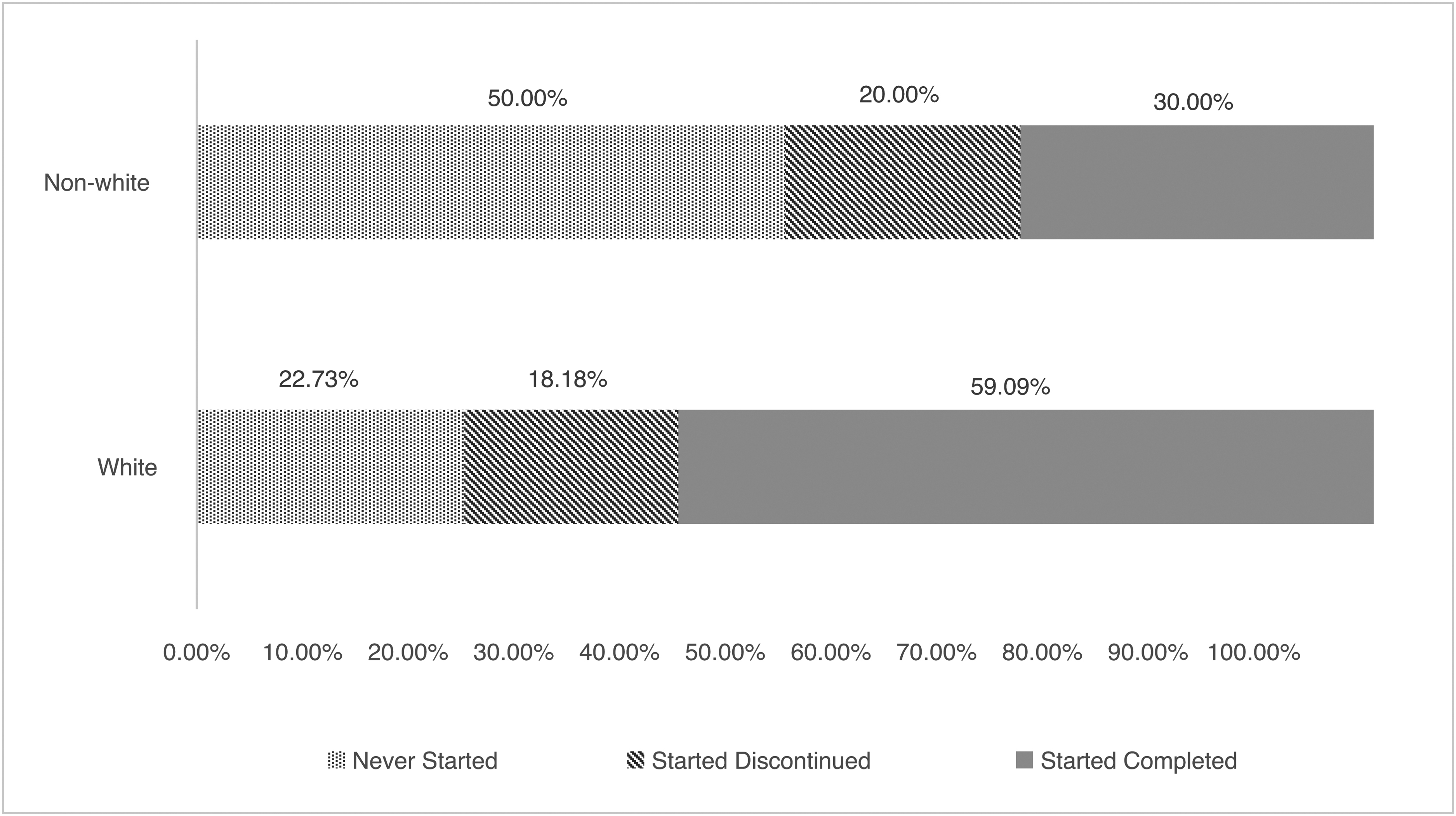
Comparison of black and Hispanic (nonwhite) and white patients starting on the 670G, including discontinuation before 1 year follow-up (started discontinued) and remaining on the system 1 year after starting (started completed).
The documented reasons for never starting auto-mode (10 patients) include sensor functionality and device frustration concerns, including failed sensors, excessive sensor alerts, sensor inaccuracy, frequent auto-mode exits, “never able to get it to function consistently,” life and family stressors, and transfer to other health care facilities. The reasons for discontinuation of auto-mode in the five patients included health insurance changes, frustration with pump–sensor interactions (n = 4), changes in health unrelated to diabetes, and transition to another pump or CGM (n = 2).
Discussion
Our analysis of patients' experience with the 670G highlights the prevailing disparities in diabetes technology use in underserved populations. A 2017 analysis from our clinic showed that among 227 adults with T1D, 30% were using CGM and 26% were using insulin pumps. This analysis also showed that white patients were more likely to be using any diabetes technology in comparison with black and Hispanic patients. Specifically, 35% of white patients were using an insulin pump and CGM combined, in comparison with only 4% of black and 9% of Hispanic patients. 1 In contrast to the 670G cohort reported in this study, in our adult clinic population, people living with T1D accounts for only 10% of our diabetes population, of which only 50% are commercial insurance beneficiaries. The mean A1c of our larger T1D cohort is also higher (9%).
From our data, it is difficult to determine whether certain patients may have been more likely to have been offered 670G technology than others, although this is certainly plausible. Nonetheless, most of our underserved population is still not receiving the potential benefits of advanced automated insulin delivery systems. Given the limited use of diabetes technology in our population, implementation of automated insulin delivery systems, such as the 670G, holds the potential for significant benefit, but also requires significant educational resources and support.
People living with T1D using the first commercially available hybrid closed-loop system in a safety net hospital are highly educated, well insured, predominantly white, female, and experienced pump users. Patients who initiated the 670G had significant improvement in A1c and reasonable 1 year adherence to the system (77% remained in auto-mode at 1 year follow-up), which is comparable with Lal et al., who reported that 67% of their 84 patient cohort remained in auto-mode at 1 year. 3 Importantly, the significant decrease in A1C in patients who initiated and continued auto-mode over a 1 year period provides additional, real-world confirmation that using a hybrid closed-loop system is correlated with improved overall blood glucose control.
It is important to highlight that 31% of patients who received the 670G failed to initiate auto-mode, even though 80% were experienced pump users with 50% holding advanced educational degrees. This group spent less time on pump education and had a 1% higher baseline mean A1c in comparison with the group who initiated auto-mode. Over the 1 year follow-up period, 2 of the 10 patients who were not initially successful were able to begin auto-mode.
In comparison with the prospective observational study conducted at Stanford by Lal et al., 3 far more of our cohort failed to initiate auto-mode at onset (31% vs. 1%). However, in those who successfully initiated auto-mode in our cohort, there was a 10% lower discontinuation rate at 1 year follow-up. Combining these two studies, closed-loop discontinuation rates of 23%–33% are significantly higher than previously reported insulin pump discontinuation rates of <10% in children and adults. 4 –6
Both studies report that the major reason for discontinuation was related to poor patient experience about pump and CGM interaction. In addition, patients from both studies who discontinued auto-mode tended to have higher initial A1c levels. However, patients who discontinued before 1 year in our cohort showed an improvement in 1-year A1c in comparison with baseline (8.14 vs. 7.20), whereas patients who discontinued auto-mode before 1 year follow-up in the Stanford study reported no change in A1c (8.3 vs. 8.3).
It is concerning that nearly a third of our patients who received the 670G were not able to successfully initiate auto-mode. In comparison with those who initiated auto-mode, the groups were similar in all domains, except that 50% of those who never started were of Hispanic or black ethnicity, compared with 23% of the group who initiated auto-mode. Notably, in both groups >90% were commercially insured and >50% held advanced educational degrees. Previous publications from our clinic have reported that although nearly 20% of black patients had an annual household income in the highest bracket, none in this income bracket used any form of diabetes technology.
These data are consistent with the knowledge that organizational context and structure influences medical technology allocation and decision-making processes and strongly suggests that features of a pump education system that relate to patient identification and eligibility, as well as addressing implicit or structural biases should be prioritized along with a focus on the refinement and development of objective pump initiation criteria.
Many studies, including “real-world” diabetes technology studies, have reported improved clinical outcomes. These improved outcomes could potentially be explained by recruitment of highly motivated engaged populations who are being cared for in large diabetes centers with extensive clinical infrastructure and experienced personnel. However, many patients living with T1D around the world, do not have ready access to these centers of excellence and creative solutions to enhance technology uptake to a broader population being cared for in community practice is clearly needed. Addressing these issues will further progress toward the goal of effectively preparing more patients for successful transition to advanced insulin delivery systems. 7,8
Qualitative aspects of our chart review highlighted that despite limited insurance barriers to obtaining the 670G, many patients experienced difficulties with obtaining necessary pump supplies for several months. This contributed to a delay in auto-mode initiation. Although, this challenge was never cited as a reason for ultimately failing to start auto-mode or discontinuing auto-mode altogether. The most frequently cited reason both for failing to start auto-mode and for auto-mode discontinuance was frustration with sensor functionality and the resulting need to respond to multiple alarms.
Our analysis is limited by its retrospective study design, as well as the small sample size (n = 32), which limits statistical power and generalizability. In addition, selection bias and referral bias need to be taken into consideration.
Given the potential for significant clinical benefit of automated insulin delivery systems in varied patient populations, future studies identifying barriers to and testing strategies for increasing use of advanced insulin delivery systems in underserved populations are needed.
Footnotes
Authors' Contributions
D.S., S.M., L.B., and A.P. were responsible for study design, protocol implementation, and data collection. Z.J. performed the initial analysis and wrote the first draft of the article. D.S., A.P., L.B., and E.B. contributed to data interpretation and reviewed/edited the article. Z.J. and D.S. reviewed the final draft and take full responsibility for the accuracy of the data reported. All authors read and approved the final article.
Acknowledgments
The authors would like to thank all the clinicians, study staff, and patients in the original study for their participation.
Author Disclosure Statement
D.S. has received research support through his institution from Novo Nordisk, Mylan Pharmaceuticals, and CURAVIT Clinical Research. All other authors have no conflicts of interest to report.
Funding Information
No funding was received for this article.