
Abstract
Background:
In the spring of 2020, our research group circulated a worldwide survey with the aim of gathering information on the use and perception of telemedicine in people living with type 1 diabetes at the start of the COVID-19 pandemic. The data suggested that a large number of respondents had rapidly adopted to telemedicine, as in-person visits were not possible, and that this was perceived positively by many. In this study, we conducted a 1-year follow-up to investigate changes in opinions and experiences to telemedicine over the past year of the pandemic.
Methods:
An anonymous questionnaire was distributed through social media (Twitter, Facebook, and Instagram) between May 9 and May 15, 2021, using an open-access web-based platform (
Results:
There were 531 survey responses from 40 countries (Europe 54%, North America 36%, South America 2%, and Africa and Asia 2%). A large percentage of respondents (67%) reported meeting with their health care provider remotely since the beginning of the pandemic, a significant increase compared with the 28% in the 2020 survey (P < 0.001). Eighty-three percent of respondents found remote appointments to be somewhat-to-extremely useful, similar to the 86% satisfaction rate in the previous survey (P = 0.061). Remote appointments were most frequently undertaken through telephone (50%) and video call (45%), which are significant changes compared with those in 2020 (72% and 28%, respectively, P < 0.001). Forty-five percent of respondents in 2021 were likely to consider remote appointments instead of in-person appointments in the future—being significantly lower than the 75% in the initial survey (P < 0.001)—whereas 37% indicated they would not. The majority of respondents (84%) reported no issues in their access to diabetes supplies and medication over the past year.
Conclusions:
This study showed that the use of telemedicine in the form of remote appointments increased during the COVID-19 pandemic in people living with type 1 diabetes, with high levels of satisfaction. However, a remarkable decline took place in the past year in the proportion of patients stating a willingness to continue with remote appointments beyond the pandemic. It seems that a personalized approach is needed since a substantial proportion of respondents in this follow-up still indicated a preference for in-person diabetes care, hence the use of telemedicine should be considered on an individual basis.
Introduction
Rapid advances in technology for the treatment and monitoring of type 1 diabetes (i.e., insulin pumps, smart insulin pens, and continuous glucose monitoring) have facilitated the way in which diabetes-related data can be communicated between patients and their health care practitioners. Whether these technologies can facilitate the widespread use of remote consultations (i.e., telemedicine) is still unclear, 1,2 and a number of concerns about data safety, increased clinician workload, and technical issues with equipment have been highlighted. 3,4 The COVID-19 pandemic forced rapid re-evaluation of telemedicine as in-person health care appointments were not possible for many people during these challenging times.
To assess the use and perception of telemedicine at the start of the pandemic in people living with type 1 diabetes, in the Spring of 2020, our research group circulated a worldwide survey. 5 We assessed the challenges, such as restricted access to health care and/or medical supplies, and the perception of risk in this population, with the aim of improving understanding of behaviors and perception relating to remote health care during the pandemic.
The main findings were that a large number of people living with type 1 diabetes had rapidly adopted to telemedicine or planned to in the near future, and that this was generally perceived positively. Age and education level of the respondents did not appear to influence perceptions of telemedicine, suggesting that telemedicine may be useful for a wide variety of individuals. Interestingly, poor glucose control seemed to negatively affect the perception on usefulness of telemedicine, particularly in men.
The aim of this study was to conduct a 1-year follow-up of our previous survey and to compare the results with the 2020 survey, to investigate possible changes in patients' opinions and experiences and whether they have encountered specific (new) challenges or problems in the past year regarding telemedicine.
Methods
An anonymous questionnaire was widely distributed through social media (Twitter, Facebook, and Instagram) between May 9 and May 15, 2021, using an open-access web-based platform (
Data were first analyzed descriptively and results were stratified according to age (<18, 18–24, 25–34, 35–44, 45–54, 55–64, >65 years), gender, and HbA1c (<7.0%, 7–9%, >9%). The z-test for two proportions was used to compare changes in the use, satisfaction, method, and perception of telemedicine (Table 1) between the initial 2020 survey and the 2021 follow-up survey. All statistical analyses were performed using RStudio (Version 1.1.447, 2018, Boston) and α was set at 0.05; statistical significance was accepted when P < α.
Overview of Demographics and Survey Responses Between the Original Data Set in Spring 2020 and the Present 1-Year Follow-Up
Results are given as mean ± SD where applicable. Note that the responders in the current data set are not the same as those in the previous investigation.
Significant difference compared to the 2020 survey, P < 0.001; NS: nonsignificant difference compared with the 2020 survey.
CGM, continuous glucose monitoring; CSII, continuous subcutaneous insulin infusion; HbA1c, glycated hemoglobin; MDIs, multiple daily injections.
Results
There were 531 survey responses from 40 countries (Europe 54%, North America 36%, South America 2%, and Africa and Asia 2%). Thirty percent of respondents were from the United States, 21% from the United Kingdom, and 14% from Switzerland. Sixty-nine percent of respondents were women, and 31% men, with 51% of respondents aged 25–44 years. The mean HbA1c of all respondents was 6.7% ± 0.9%, and time since type 1 diabetes diagnosis was 20 ± 13 years. Fifty-eight percent of respondents were on insulin pump therapy, and 42% used multiple daily injections. The majority of respondents (83%) perceived themselves to be in a good to excellent pre-existing health condition.
However, 48% reported to have additional medical complications besides type 1 diabetes with thyroid disease (25%), depression (11%), coeliac disease (9%), and asthma (7%) the most commonly reported. Forty-five percent of respondents reported to have concomitant diabetes complications such as mild-to-severe retinopathy (20%), hypertension (15%), diabetic neuropathy (5%), diabetic nephropathy (1%), and vascular complications (4%). Moreover, 9% experienced respiratory complications requiring medications over the past 6 months with asthma being the most reported (47%). Sixty-one percent of respondents had been tested for COVID-19 since the start of the pandemic, with 5% of respondents testing positive, none of whom were hospitalized.
The comparison of the main findings from this data set and that collected in 2020 is given in Table 1. A large percentage of respondents (67%) reported meeting with their health care provider remotely since the beginning of the COVID-19 pandemic, being a significant increase compared with the 28% in the 2020 survey (P < 0.001). A further 4% of respondents, who have not yet had a remote appointment, planned to have a remote appointment in the future (Fig. 1). Concerning satisfaction rates, 83% of respondents found remote appointments to be somewhat-to-extremely useful, similar to the 86% satisfaction rate in the previous survey (P = 0.061).
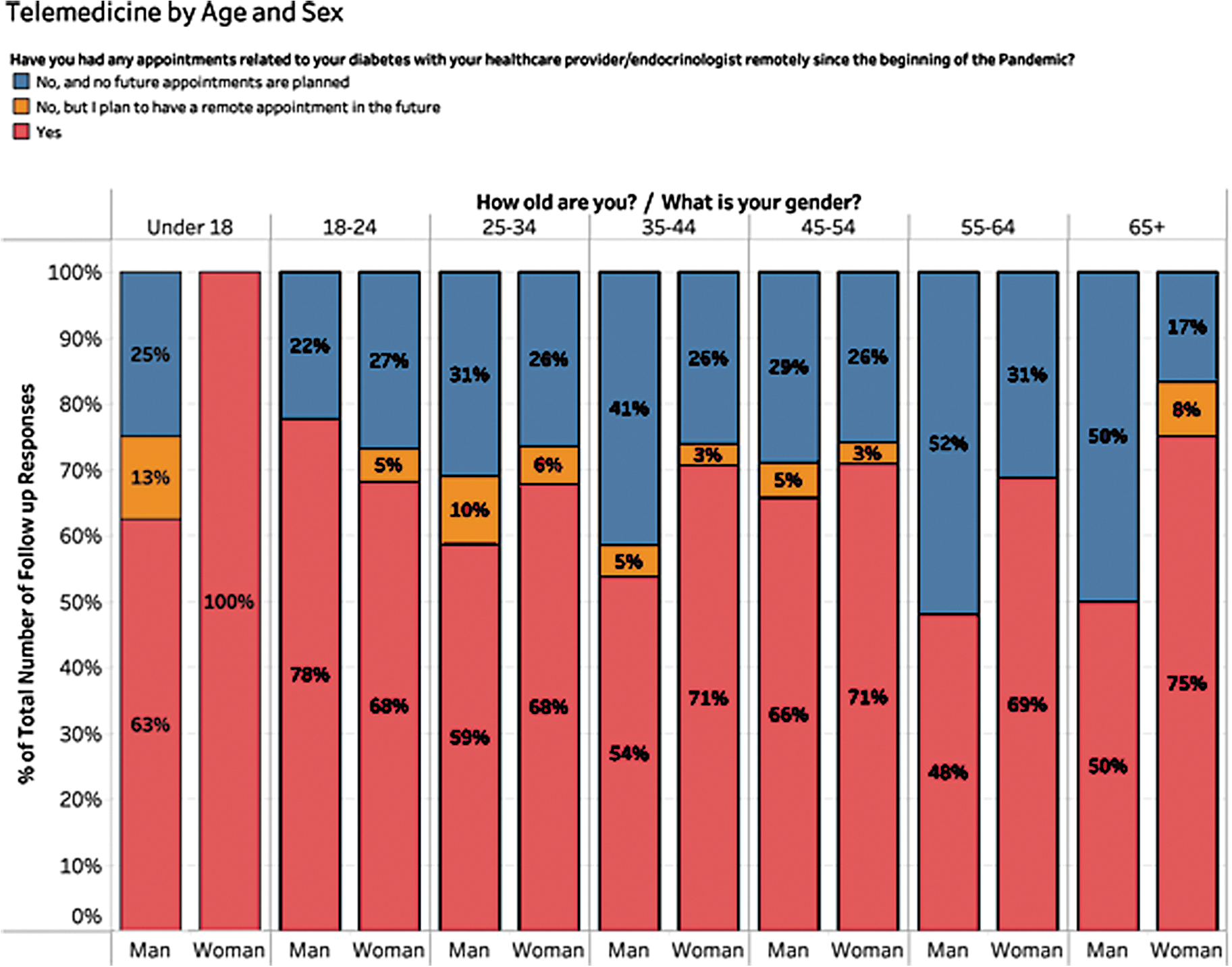
Telemedicine use by age and gender, in response to the following question: “Have you had any appointments related to your diabetes with your health care provider/endocrinologist remotely since the beginning of the pandemic?” (Blue: “No, and no future appointments are planned”; orange: “No, but I plan to have a remote appointment in the future”; red: “Yes”). Color graphics are available online.
Fifty percent of remote appointments were completed through telephone and 45% were completed through video call, showing a significant shift in method of telemedicine compared with those in 2020, when telephone and video calls were used by 72% and 28% of respondents, respectively (P < 0.001). Forty-five percent of participants were likely to consider remote appointments instead of in-person appointments in the future, which is remarkably lower than the 75% in the initial survey (P < 0.001). In 2021, 37% indicated they would not consider remote appointments after the pandemic (other answers: 17.6% responded neutral and 0.4% did not respond).
Of the participants who reported having their appointments through telephone, 51% stated that they were likely to consider remote appointments in the future. A similar percentage of those having their appointment through video call (52%) stated that they would consider remote appointments in the future. Of the participants using multiple daily injections to manage their diabetes, 35% stated that they were likely to continue with remote appointments whereas 53% of respondents using continuous subcutaneous insulin infusion (CSII) were likely to continue with remote appointments. In European countries, 38% of respondents were likely to consider remote appointments in future. In North American countries, 51% of respondents were likely to consider remote appointments in the future.
The majority of respondents (84%) reported having no issues in their access to diabetes supplies and medication over the past year. Within the 12% who reported having difficulties in accessing diabetes-related supplies, continuous glucose monitors (6%), insulin (5%), and testing strips (3%) were the diabetes-related devices most difficult to access during the COVID-19 pandemic.
Discussion
We conducted a 1-year follow-up of our previous survey 5 to assess the use and perception of telemedicine, and the change herein, in people living with type 1 diabetes one year after start of the COVID-19 pandemic lockdowns. Comparing the results of the two surveys, some interesting differences could be noted. In 2021, there was a significantly greater percentage of respondents reporting having remote appointments with their health care provider compared with that in 2020, and most respondents who had experienced remote appointments found them useful in 2021—at similar levels to the 2020 survey.
There was a significant increase in the use of video calls as the delivery method of remote appointments in 2021. Despite the increase in the prevalence of remote appointments between the surveys, the willingness to consider remote appointments in addition to, or instead of, in-person appointments in the future remarkably decreased. This suggests that the extent to which telemedicine is implemented should likely be considered on an individual basis, with perhaps potential for a hybrid of in-person and remote appointments.
The greater proportion of respondents in the follow-up survey who had had at least one remote appointment for routine diabetes care (67%) compared with the original survey (28%) is not an unexpected finding, since a substantial percentage of real-life consultations were cancelled last year. Moreover, a large proportion of respondents found their remote appointments to be useful in both the original (86%) and the follow-up study (83%), showing that there are opportunities for implementing telemedicine in the future in patients with type 1 diabetes.
Even before the COVID-19 pandemic, discussions as to how digital diabetes technologies and telehealth protocols could facilitate the widespread use of telemedicine in type 1 diabetes had taken place. 6 However, the COVID-19 pandemic forced a rapid acceleration of this process, as we report here. A recent review by Danne et al. 7 found that telemonitoring of glucose data has been valuable for many individuals with access to this technology. However, there are still significant hurdles before this can be applied to everyone, such as access to the technology and education around such services.
It is important to acknowledge the difference in the way these appointments had been conducted, with a greater percentage of respondents stating that their appointment had now taken place through video calls (45%) compared with those 1 year before (28%), whereas in the previous year more people spoke to their health care provider over the phone. The use of video call consultations in telemedicine has previously been found to be a feasible and acceptable method in pediatric and young adult type 1 diabetes populations. 8 –11
Two case reports of individuals with new onset type 1 diabetes conducted by Garg et al. 11 of how telemedicine was used effectively and safely in combination with in-person patient education provide detailed information that supplements our findings. Their case reports, in combination with our large data set showing that many people have used telemedicine, suggest that telemedicine can be used safely and effectively by people living with type 1 diabetes.
Remarkably, although a greater percentage of respondents stated that they had undertaken at least one remote diabetes appointment in the follow-up survey, a lower percentage of respondents (45%) reported a willingness to have remote appointments in the future compared with those in the original survey (75%), suggesting that many patients still prefer in-person appointments. Although the response rate was lower in the follow-up survey, these findings suggest that the ideal ratio of telemedicine to in-person visits in type 1 diabetes care still needs to be investigated, 12 and is likely to vary considerably between individuals. Unfortunately, comparing regional differences is difficult to infer with confidence given the lower number of responses in many countries.
However, we were able to note differences between Europe and North America. In European countries, 38% of respondents were likely to consider remote appointments in future. In North American countries, 51% of respondents were likely to consider remote appointments in the future. Interestingly a much larger percentage of those in North America were using CSII than those in Europe (80% in North America vs. 45% in Europe). Although we cannot say for certain that this accounts for the higher percentage of respondents from North America stating that they would continue with remote appointments, we may perhaps speculate that the greater uptake of diabetes technology (in the form of CSII) contributed to the greater openness to telemedicine. Further research is needed to clarify this.
The strength of this study comes from the ability to collect data from a reasonably large number of individuals in a short timeframe. This knowledge will help to understand the state of diabetes care and inform implementation of remote health care in the future. We feel that the results of this survey are very timely, as clinics are trying to understand the balance of in-person versus telemedicine visits for diabetes as COVID-19 restrictions are progressively relaxed. 7 Although the 2021 survey showed a considerably lower response rate than the initial survey (531 vs. 7477 respondents), the demographics of the respondents were similar, with women, adults aged 25–34 years, and people with good levels of glycemic control and good pre-existing health being the most common respondents in both of the surveys (Table 1).
A possible explanation for this could be that the initial uncertainty and fear at the beginning of the pandemic was markedly reduced, next to acceptance of the COVID-19 situation and life that was slowly returning to “normal” as restrictions were being eased in the first half of 2021. In addition, it may be that people are fatigued by COVID-19 in general, or by the number of surveys that have been circulated in the past year related to COVID-19. Thirdly, the survey for the present follow-up was open for just 2 weeks compared with ∼10 weeks in 2020. Although the sample size was substantially lower in the 2021 survey, the power for the comparative analysis was sufficiently high (β = 0.984; based on post hoc power analysis for z-test for two proportions), allowing us to detect significant differences in the responses between the two surveys (Table 1).
Other limitations include that our data are limited to those completing the survey and thus people who have access to the internet and technology that may not be representative to everyone living with type 1 diabetes. Lastly, the dominance of responses from the United States, United Kingdom, and Switzerland likely represents the social media presence of our research team being strongest in those three countries. During this follow-up study, we did not alter the way in which our survey was distributed, as this would make it more difficult to compare the results with those of the original survey in 2020.
This study showed that the use of telemedicine in the form of remote appointments increased in people living with type 1 diabetes during the COVID-19 pandemic, with high levels of satisfaction. However, the comparison of the two surveys' data also highlighted a remarkable decline in the past year in the proportion of patients stating a willingness to continue with remote appointments beyond the pandemic.
It seems that a personalized approach is needed since a substantial proportion of patients in this follow-up still indicated a preference for—and some of them possibly need—in-person diabetes care. Therefore, the extent to which telemedicine is implemented in the future should likely be considered on an individual basis, and there are still areas to be improved within the delivery of telemedicine for people living with type 1 diabetes.
Footnotes
Authors' Contributions
S.N.S., F.Y.F., T.Z., M.L., and C.S. contributed to the design of the study and data collection. S.N.S., F.Y.F., S.H., J.P., and C.S. analyzed and interpreted the results. S.N.S., S.H., J.P., and C.S. prepared the first draft of the article and all authors reviewed and approved the article. C.S. is the guarantor of this study and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data.
Acknowledgments
The authors thank Fitzalan Crowe, Alice Podenzana, and Cordelia Trümpy for their help and enthusiasm helping to raise awareness of the study through social media. We are also grateful to Alice Podenzana and Christina Lyko for their help with translating the survey.
Data Sharing
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics
The study was performed in accordance with the Declaration of Helsinki and the regulations of the local ethical committee.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by the Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism Bern research fund. S.N.S. is part funded by the Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, Bern University Hospital and Team Novo Nordisk Professional Cycling Team. F.Y.F. is funded by Team Novo Nordisk Professional Cycling Team.