
Abstract
One hundred years ago, insulin was first used to successfully lower blood glucose levels in young people living with what was then called juvenile diabetes. While insulin was not a cure for diabetes, it allowed individuals to resume a near normal life and have some freedom to eat more liberally and gain the strength they needed to live a more active lifestyle. Since then, a number of therapeutic and technical advances have arisen to further improve the health and wellbeing of individuals living with type 1 diabetes, allowing many to participate in sport at the local, regional, national or international level of competition. This review and commentary highlights some of the key advances in diabetes management in sport over the last 100 years since the discovery of insulin.
Introduction
In January 1922, 14-year-old Leonard Thompson received his first injections of “Macleod serum” (later called Toronto Insulin) that successfully lowered his blood glucose and ketone levels at the Toronto General Hospital. 1 Within a few weeks of insulin treatment, Leonard's weak 5′11″ 65-pound body, which was once fueled by just 450 calories per day and 20–25 g per day of carbohydrate, transformed with daily insulin injections and a caloric intake that was estimated to increase to 2040 kcal per day. 2 Thanks to insulin and a higher caloric intake, although mostly from dietary fat, he was able to start working as a clerk, and live another 14 years in relative good health before being admitted to hospital with influenza and ketoacidosis, where he eventually died, perhaps from insulin overdose and severe hypoglycemia. 3
With the centenary of the discovery of insulin, and recent completion of 2020 Tokyo Summer games in which a number of athletes living with type 1 diabetes (T1D) competed, it is important to acknowledge the many technological advancements that have been developed to support the health and wellbeing of young people like Leonard living with diabetes. That first insulin dose back in 1922 was just the first of many innovations, whether pharmacological, technological, or behavioral, which have allowed many inspiring individuals living with diabetes, who are also competitive athletes, reach the highest level of sport and competition (Fig. 1).
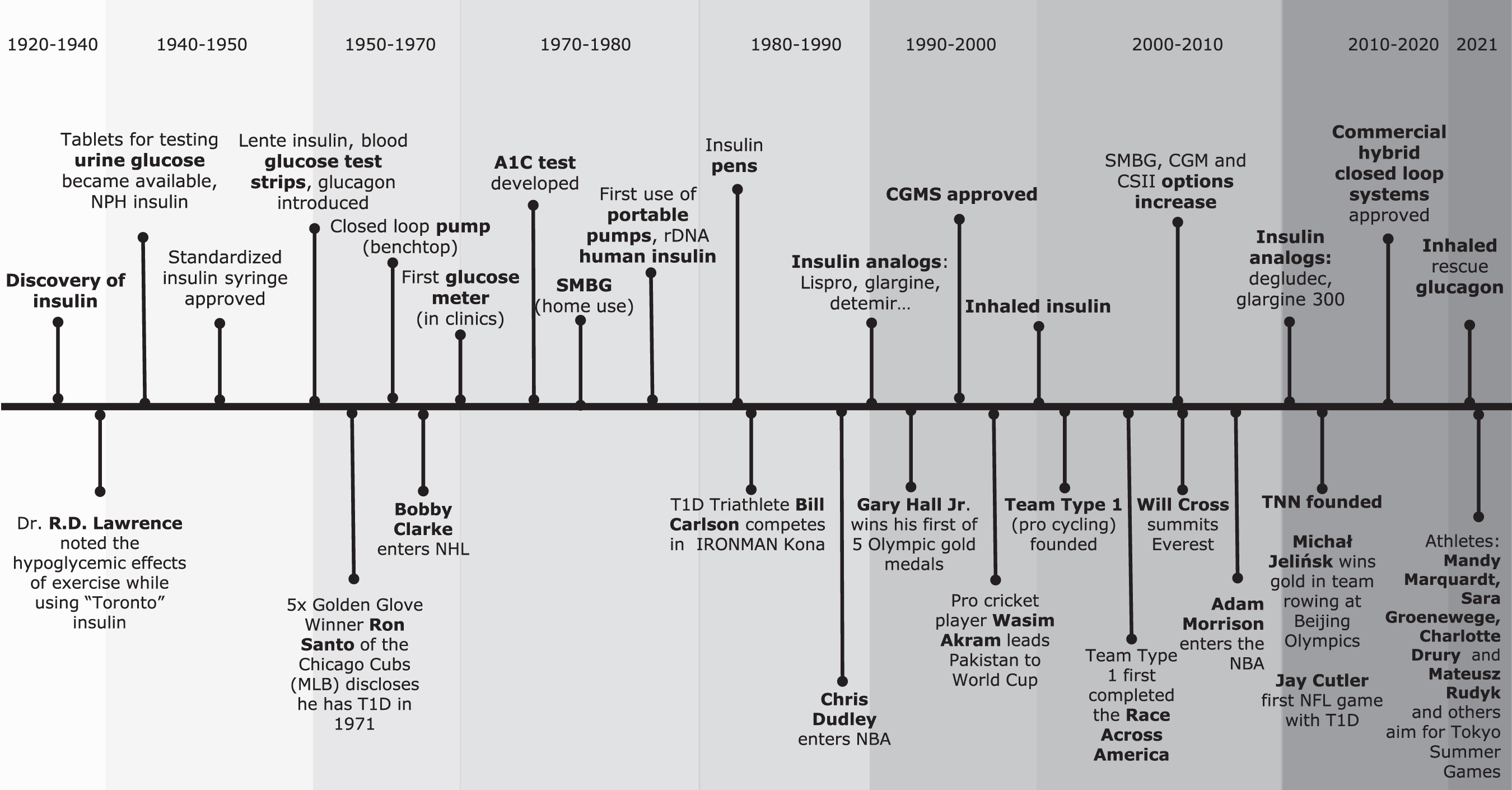
Key diabetes-related discoveries and technological advances along with some major sporting achievements by individuals living with type 1 diabetes over the last 100 years. CGMS = Continuous glucose monitoring system.
New insulin formulations, continuous glucose monitors, sleek new digital insulin pens that track insulin dosing using smartphone-based integration, and “closed loop” automated insulin delivery (AID) pumps now exist and further advances are happening all the time. These and other technical and therapeutic developments help young athletes with T1D, like gymnast Charlotte Drury, track cyclists Mandy Marquardt and Mateusz Rudyk, softball player Sara Groenewege, NHL hockey player Max Domi, and others live a near normal life and compete against their peers. This commentary highlights the evolution of advancements in technologies that support the active and sometimes competitive individual living with T1D.
The Past
As early as 600 BC, the beneficial impact of regular exercise on minimizing the consequences of diabetes and obesity was mentioned by the ancient Indian physician Sushruta (or Suśruta), about 2600 years before insulin was discovered. 4 In the early 1900s, Drs. Frederick, 5 Joslin, 6 and others recommended daily exercise to help control high glucose levels in the urine in young people living with a severe form of diabetes, later termed juvenile diabetes.
After the discovery of insulin and its administration to patients, Dr. Fredrick Banting and his clinical colleagues noted that the treatment improved the strength and stamina of their patients, allowing individuals like 15-year-old Elizabeth Hughes' health to improve enough that she could once again enjoy bicycling and other sporting activities like tennis on regular occasions. Banting stated in his Nobel Lecture that insulin treatment produces “[...] a greater ability to do mental and physical work...” and on this treatment, “the patient gained rapidly in strength, and was soon able to take vigorous exercise.” 7
It did not take long for people to notice that insulin and exercise had similar effects on glycemia—the potency of the hormone was clearly enhanced with a single session of exercise. This was best profiled first in the literature in 1926 by Dr. R.D. Lawrence with his demonstration that his patients with insulin-requiring diabetes (i.e., T1D) required about 50% less bolus insulin (i.e., 8 vs. 16 units of insulin for ∼20 g of carbohydrate) to prevent hypoglycemia when they were engaged in sport or exercise soon after a meal. 8 Lawrence himself was living with T1D and noted that his own insulin needs were reduced on his active days.
In the 1920s, urine glucose testing and the “symptoms” of high glucose (e.g., frequent urination, dehydration, fatigue, blurred vision, and so on) or low glucose (e.g., a sense of anxiety, tremor, weakness, confusion, and so on) were the only way for individuals with T1D to self-monitor their glucose levels. Dr. Lawrence also found that an afternoon full of exercise made insulin work much more effectively in his patients, thereby resulting in a lowering in their blood glucose levels in the next 24 h, 8 a finding that has repeatedly been confirmed now by using exercise wearables and continuous glucose monitoring (CGM). 9
Yet, 100 years ago, the inability to monitor blood glucose levels during exercise, or even at home, would have made the decision-making difficult. Also of note in Lawrence's early publication 8 was that if regular exercise was undertaken, the individual with diabetes could double his total daily carbohydrate intake (from 48 to 100 g/day in the case study provided) with the same total daily insulin dose (28 units), without producing any glucose in his urine also noting that the patient's body weight would remain relatively stable. 8 The case subject gained muscle mass with regular exercise even though his daily insulin needs dropped. Home self-monitoring of blood glucose (SMBG), first demonstrated in Europe in the 1970s, helped markedly to illustrate the impact of insulin, food choices, and exercise habits on patients glycemia. 10,11
With the advent of intermediate-acting neutral protamine Hagedorn insulin in the 1940s and 1950s, typically given twice per day, and newer basal and bolus analogs in the later decades, it became clear that exercise improved the potency of most forms of insulin and that dosages would need to be reduced on more active days. 12 –18 The introduction of better insulin needles with a higher dose resolution and eventually insulin pens allowed individuals to more conveniently titrate their insulin dose depending on the level of physical activity and carbohydrate intake. Although large benchtop pumps could keep glucose in a targeted range in people living with diabetes by using intravenous insulin and glucose delivery in the 1960s and 1970s, the advent of a portable subcutaneous insulin pump, weighing only 159 g, arose in the late 1970s, which could easily be worn during exercise. 19
With the development of the hemoglobin A1c (HbA1c) test in the 1970s, it was demonstrated in the early 1980s that glycemic control can improve with regular exercise training. 20 This was important, since it soon would be published that diabetes-related complications could be delayed by having good glycemic control by the Diabetes Control and Complications Trial group. 21 In and around that time, increased SMBG was recommended 1 h before exercise, to allow for manipulations to food or insulin, once again just before the activity and then again every 15–30 min during the event. 22,23 Carbohydrate snacking, without taking bolus insulin, was recommended by diabetes care experts who studied the exercise response. 24,25
Increased SMBG and increased carbohydrate snacking at bedtime were also frequently advised to help guard against the high risk for nocturnal hypoglycemia in the active patient. 26 –30 Eventually, algorithms that recommended bolus insulin dose reductions 31,32 or reductions in intermediate acting insulin 17 for exercise were developed and successfully tested. The recent development of even longer basal insulins (i.e., insulin glargine 300 units/mL, insulin degludec) required additional studies to be conducted to determine the benefits and limitations of being active on these ultra-long-acting insulins. 33,34 In general, the benefits of the new ultra-long basal insulin include a flatter basal profile over a 24-h period, but the inability to temporarily reduce circulating levels for periods of prolonged exercise. For those on emerging continuous subcutaneous insulin infusion (CSII) systems, basal rate reduction, sometimes with the complete interruption of basal insulin infusion 16,17 was tested, with varying success on limiting hypoglycemia.
The Present
The development of diabetes-related technologies has been moving at an increasingly rapid pace in recent years as researchers aim to improve all aspects of diabetes patient care, including glucose time in range, risk of complications, psychological challenges of living the disease, and all the management decisions that need to be made. New insulin formulations, methods of insulin delivery, and various wearable technologies now make exercise safer and easier to track for the person living with diabetes. However, due to a shifting society toward more sedentary behaviors and more sitting time, many individuals perform less physical activity than in previous generations. 35
For many people living with T1D, a fear of hypoglycemia is a barrier to exercise. 36 A large proportion of people living with either type 1 or type 2 diabetes do not engage in the American Diabetes Association recommended 150 min of weekly activity. 37,38 This is unfortunate since regular exercise has many benefits for individuals living with diabetes, including increased insulin sensitivity, improved lipid profile, enhanced psychosocial health and well-being, and potentially better weight and glucose control. 39,40
With today's knowledge related to the health benefits of regular exercise, people of all ages with diabetes should prioritize being physically active. Some individuals living with diabetes compete at the highest level in sport, while others with the disease may be less confident to engage in sport and exercise because they feel it presents a challenge to their glucose control. 41 –43 Indeed, current technologies such as CGM and AID systems with exercise “modes” are now being used by individuals with T1D to lead a more active lifestyle with improved glucose stability. 44,45
Compared to adults, the use of technology to assist with the management of glucose in children and adolescents presents additional challenges, due to greater spontaneity associated with unpredictable play. Adolescents and young adults with T1D still have difficulty maintaining their glycemic targets, even when CGM and CSII technologies are used. 46 The failure to achieve targets in this segment of the population is likely because of a combination of physiologic and psychosocial factors 47,48 and various sociodemographic and other barriers limit uptake and/or access to diabetes-related technologies in youth with the disease. 49 Hybrid closed loop systems help youth with T1D better manage their glycemia, particularly in the overnight setting, but the spontaneous nature of their activities may limit the capacity of insulin-only systems to manage their glycemia during the day. 50
A structured approach to pediatric exercise management, using technology enhancement, may help improve glycemic targets during and after exercise. 51 At present, a large observational study of youth with T1D in North America by the Jaeb Center for Health Research will help determine if current technologies enhance glycemic control around exercise in adolescents with T1D. 52
CGM technology was first used in 1999, as a blinded unit primarily for clinic usage, with the use of real-time CGM units now demonstrating clear improvement in HbA1c levels in patients living with T1D. 53 The widespread use of either real-time CGM or intermittently scanned continuous glucose monitoring (iCGM) is on the rise in North America and Europe, 54,55 largely because of increased user acceptance, enhancement in user experience by incorporating visual data displays alarms and alerts and other features, data sharing capabilities, improved comfort or wearability, and a greater access to the technologies. 56
Randomized controlled trials and clinical studies demonstrate the utility of using CGM while leading a physically active lifestyle, making it a preferred tool for glucose monitoring in the active patient 57 –61 —a far cry from the early days of urine glucose testing. In general, compared to SMBG, CGM is associated with more time in range and a reduced risk for hypoglycemia overall, 62,63 and new actionable guidelines now exist to help individuals with diabetes use CGM more effectively during exercise. 37 CGM has increasingly made diabetes and glycemic management easier by allowing the individual to track in near real-time their unique glycemic responses to various forms of exercise. It also reduces the number of times an active patient needs to stop their activity to perform a glucose measurement and it provides more retrospective data on glucose levels to refine the athlete's insulin and nutritional feeding strategies.
The integration of CGM technology with sensor-augmented insulin pumps help to automatically reduce insulin delivery after exercise, 64 while several hybrid closed-loop systems are being tested and showing efficacy in various exercise settings, according to a recent meta-analysis. 65 CGM systems have been demonstrated to help both professional and recreational athletes with T1D track glucose levels before, during, and after exercise and send alerts when glucose is trending toward hypoglycemia allowing them to minimize hypoglycemia. 66 –68 CGM allows for data amalgamation and sharing, enabling the individuals' care team, trainer, or parent to better monitor glucose levels in the context of sport and competition. However, some drawbacks of using CGM technology for exercise exist at present. The main challenges include accessibility, wearability, skin irritations, information overload, or the visualization of having diabetes and the deterioration in sensor accuracy during exercise. 69 –74
Compared to CGM measurements made during rest, CGM during exercise deteriorates slightly for a number of reasons, including body fluid shifts, temperature changes, and rapid changes in glucose flux between tissues. 75 To date, no head-to-head studies of CGM accuracy during exercise from the various CGM manufacturers have been published. However, in a limited number of exercise studies, where either CGM or iCGM is used and comparisons were made against a reference method for glucose concentration, the mean absolute relative difference (MARD) was higher during exercise with iCGM (i.e., Abbott Libre 1) (19.6%; 95% confidence interval [CI] 9.7%–29.6%) compared to the real-time CGM units from Medtronic (11.7%; [9.3%, 14.2%]) or Dexcom (14.1%; [11.3%, 17.0%]). 76
The observed rise in MARD during exercise in all sensors, compared to sensor MARD during rest, is likely primarily related to the 15- to 20-min lag time in glucose equilibrium between the blood stream and the interstitial space when glucose levels are changing rapidly. 69,77
While we see CGM as useful technology for exercise, some individuals with diabetes simply do not want to have sensors and transmitters on body during sports and exercise for a variety of reasons related to invasiveness, comfort, cost, and accuracy. 78 Overall, CGM is likely valuable for most “athletes” living with T1D if they perceive that the benefits outweigh drawbacks, even when used independently of an AID system. While accuracy challenges exist at present, we feel that the latest systems are likely accurate enough for on-the-spot decision-making and for use with closed-loop systems during exercise. 37,76
Digital smart pens and insulin infusion devices (i.e., pumps) have also improved the resolution and tracking of insulin delivery and may make insulin adjustments for exercise easier. 79 AID systems now have preprogrammed “exercise” settings, which include higher glycemic targets and individually tailored to the user's unique insulin sensitivity. 80 A recent meta-analysis demonstrated the efficacy of AID systems in a variety of exercise settings. 65 Exercise wearables may be helpful for overcoming some of the physical activity challenges around glucose management and have the ability to assess physical activity patterns over time. These devices can now be equipped with accelerometers and photoplethysmography sensors to assess pulse rate, and increasingly, people use such devices to monitor their heart rate, energy expenditure, and the overall intensity of daily movements. 81
Individuals with T1D can also use these devices to recognize patterns between daily activities and their blood glucose, 82 with emerging technology, such as the new Fitbit and OneTouch Reveal™ having visual syncing ability. 83 Merging data from exercise wearables, blood glucose, and insulin delivery systems may be particularly useful for active people with T1D, since this should allow for better data visualization for the individual, their diabetes care team, and perhaps their coaches and/or trainers. 84 In addition, these devices may be useful in showing users their activity/goal achievement, 82 which for some may provide additional motivation to live an active lifestyle.
The Future
Improving glycemia and reducing the burden around decision-making for exercise and sport is likely to remain as a major hurdle for individuals living with T1D. 85 Sometimes, it appears that technology can increase patient burden for some active adolescents with T1D. 86 However, the pace at which new and improved diabetes-related technologies are being developed and implemented to help reduce the emotional cost of the disease is astonishing. Unfortunately, regulatory hurdles are sometimes a barrier for emerging diabetes-related technologies 55, and some individuals have elected to use noncommercial “do-it-yourself” systems to manage their glycemia around sport with some success. 87 We suspect that incremental advances in closed-loop technologies that support glucose control during sport and exercise will continue to evolve over the next several years.
Currently, when commercially available AID systems are set to “exercise” mode, they do not fully protect against hypoglycemia unless they are actuated well in advance of exercise. 65,80,88,89 Supplemental carbohydrate can be taken with AID systems with exercise when the activity is unplanned, 90 but we feel that the addition of solubilized glucagon just before or during the exercise, via dual hormone pump 91,92 or as a stand-alone injection, 93 would be another major advancement.
Future systems that integrate historical physical activity pattern recognition to automatically place a closed-loop system in an exercise mode sooner than patient-initiated actions, which are in early development, 94 should further reduce hypoglycemia risk. Future systems that also automatically adjust the insulin to carbohydrate ratio for the bolus insulin before, during, and/or after exercise may also be useful. 95
Ongoing research will determine if new technologies can improve glycemic management and perhaps even exercise performance in people living with diabetes. Future studies should build on work already demonstrating that wearables might be useful for integration with AID systems to “signal” changes in activity patterns, with additional information on the intensity and type, to further contextualize the exercise event. 96 –100 Wearables can easily track patient's daily physical activity patterns using step counts, heart rate, and/or accelerometry to better inform prandial and “basal” insulin needs, which could be also be integrated into future AID systems. 95,99,101 –104 Recent proof of concept studies have demonstrated that wearables, along with machine learning, trained on rich data sets, and other sophisticated engineering tools, can potentially identify historical physical activity patterns 94 and quantify exercise type and relative exercise intensity. 105
These innovative approaches should allow for robust physiological and behavioral data capture and integration of these data into clinical decision-making for therapy optimization and for on-the-spot decision-making for AID systems to change the insulin and/or glucagon delivery rate or alert the user to initiate carbohydrate feeding to maintain percent time in range (see Fig. 2 for a concept drawing).
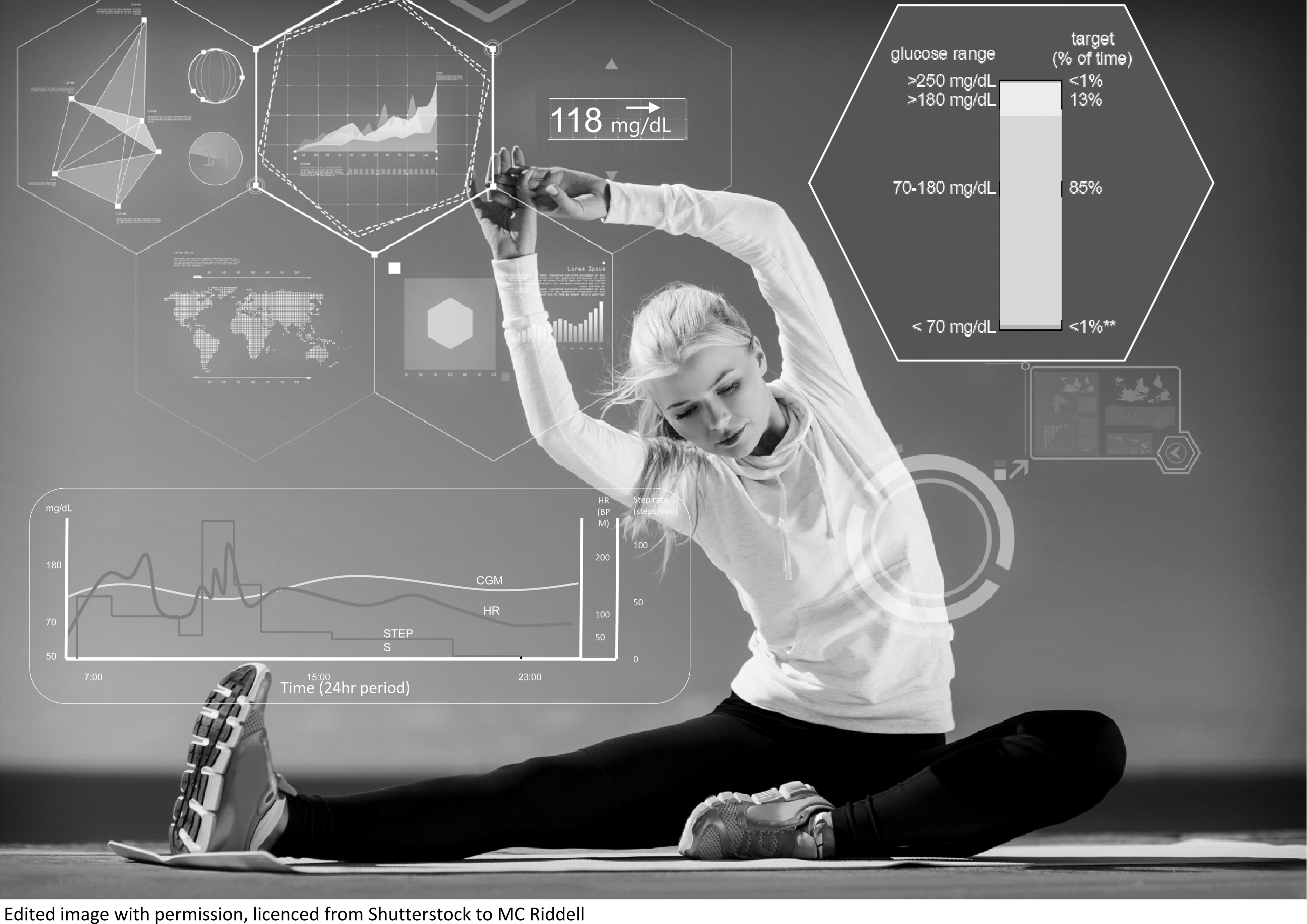
A concept image of the possible future integration of activity wearables, lifestyle pattern recognition software, CGM data reports and automated hormone delivery systems. CGM = continuous glucose monitoring.
In the future, we feel it may be important to have accurate and discrete ways of tracking and objectively quantifying daily exercise volumes and intensities using body-worn sensors in some subpopulations of patients living with diabetes. However, the current accuracy of some of the exercise wearables remains a concern, with generally poor accuracy particularly for the assessment of energy expenditure, 106,107 especially as exercise intensity increases. 108 As such, the integration of energy expenditure metrics may hinder their integration with future AIDs. If these problems are fixed and physical activity metrics are integrated into AID and CGM systems, a clearer picture of health can be seen by the person with T1D and their health care provider.
Some other future advancements that would help the active patient will likely be the commercial release of dual hormone systems, that may be integrated with wearables, that can clearly work synergistically to lower the risk for exercise-associated hypoglycemia and improve time in range. 91
Machine learning approaches are increasingly being harnessed to incorporate decision support into many medical settings 109 –111 and a number of applications have already been developed to provide decision support to people with diabetes. 112 –115 The increasing use of health-based mobile computing and increasing availability of CGM or flash glucose monitoring, particularly in developed countries, has created an opportunity for development of automated decision support systems for people with T1D. 112,113 Such decision support systems can be provided to a person with T1D either through a health professional who provides the recommendations or directly to the patient using a smartphone app that automatically generates recommendations. These applications may provide far more frequent insulin dosage adjustment recommendations with less frequent physician visits.
A final area for technology advancement should be the continued development of smart phone applications that assist with insulin and carbohydrate decision-making with exercise in active individuals. Smart-phone apps, such as “mySugr” and “bant” that provide some personalized feedback on overall diabetes management by tracking meals, physical activity, weight, and glucose data, should continue to evolve by using more sophisticated technologies such as accelerometers to better track activity levels and integrate this information to the ambulatory glucose profile. Others in development, such as “ T1Exercise” and “acT1ve” apps that use exercise advisor algorithms, should be tested for safety, efficacy, and user satisfaction in larger clinical trials. 116,117 Moreover, the consensus-based clinical recommendations for the use of CGM in exercise to better inform insulin dose adjustments and carbohydrate intake rates 37 should be tested in large and more diverse populations of children and adults with T1D.
Summary
The first insulin injection given 100 years ago was a great achievement in the history of medicine and is a dramatic example of rapid translation of discovery in basic science into benefit for patients. 118,119 However, this marked just the beginning of the many technological advances that have been made over the last century to support the active person living with diabetes. While we acknowledge that many individuals did well long before the diabetes technology revolution, others have embraced these technologies and because of that realized their athletic dreams. Future work should continue to focus on trying to merge these technologies to further enhance and synergize the evolution of these incredible technologies.
Footnotes
Authors' Contributions
M.C.R. did the literature search. All authors contributed to the original draft of the article and edited the revised article. All authors approved the final submission.
Author Disclosure Statement
M.C.R. has received consulting and/or advisory board fees from Zucara Therapeutics, Zealand Pharma, Indigo Diabetes, Supersapiens, Novo Nordisk, Insulet, Medtronic, Eli Lilly, and Sanofi. D.S has no disclosures. S.N.S. is employed by Team Novo Nordisk Professional Cycling Team.
Funding Information
D.S. is a recipient of the Natural Sciences and Engineering Research Council of Canada Undergraduate Student Research Award.