
Abstract
Background:
Technology for patients with type 1 diabetes (T1D), including continuous glucose monitoring (CGM), insulin pumps, and hybrid closed-loop (HCL) systems, is improving, being used more commonly in the pediatric population, and impacts glycemic control.
Materials and Methods:
We evaluated the use of these technologies and their impact on glycemic control among patients with T1D who were seen at the Barbara Davis Center (n = 4003) between January 2018 and December 2020, <22 years old, with diabetes duration >3 months. Data were analyzed by age group and technology-use group defined as multiple daily injection with blood glucose meter (MDI/BGM), pump with BGM (pump/BGM), MDI with CGM (MDI/CGM), and pump with CGM (pump/CGM). Glycemic control was compared using analysis of covariance (ANCOVA) and controlling for diabetes duration, race, and insurance.
Results:
Among 4003 patients, 20% used MDI/BGM (mean hemoglobin A1c [HbA1c] = 10.0%); 14.4% used pump/BGM (mean HbA1c = 10.0%); 15.4% used MDI/CGM (mean HbA1c = 8.6%); and 49.8% used pump/CGM (mean HbA1c = 8.1%). Compared with MDI/BGM patients, MDI/CGM and pump/CGM users had a lower HbA1c and were more likely to reach an HbA1c <7.0% (all P < 0.0001). Among pump/CGM users, 35% used HCL technology (mean HbA1c = 7.6%) and had a lower HbA1c and were more likely to reach an HbA1c <7% than non-HCL users (P < 0.001).
Conclusions:
CGM use was associated with a lower HbA1c in both MDI and pump users. Pump use was only associated with a lower HbA1c if used with CGM. HCL was associated with the lowest HbA1c. Spanish language and minority race/ethnicity were associated with lower rates of pump and CGM use, highlighting the need to reduce disparities.
Introduction
Type 1
In a comparison between the U.S. and European diabetes registries, participants in the European centers were twice as likely to achieve a target of HbA1c <7.5%, demonstrating that more aggressive glycemic control can be safely achieved in this age group. 5 Use of diabetes technologies, including continuous subcutaneous insulin infusion pumps (pump) and continuous glucose monitors (CGM), is associated with lower HbA1c trends. 2,5 Notably, individuals who use CGM have demonstrated even lower HbA1c levels when combined with an insulin pump across all age groups. 2,5,6
Recent advances in diabetes technology offer further potential to improve glycemia. These include the U.S. Food and Drug Administration (FDA) approval of nonadjunctive use of CGM in 2016, 7 the first hybrid-closed loop (HCL) system in 2017, 8 –10 the first factory-calibrated real-time CGM in 2018, 11,12 and a second HCL system approved in 2019. 13,14 The use of CGM in the United States has increased from 7% in 2010–2012 to 47% in 2016–2018. 2 However, few analyses to date have evaluated glycemic trends in U.S. children following widespread rollout of these new technologies. Therefore, we sought to evaluate HbA1c levels by CGM and insulin pump use among pediatric patients with type 1 diabetes (T1D) at a single, large U.S. center.
Methods
This study was approved by the Colorado Multiple Institutional Review Board (IRB). The electronic medical records database at the Barbara Davis Center for Diabetes was queried to identify Colorado residents with T1D seen in clinic at the Barbara Davis Center between January 2018 and December 2020, who at the time of last visit were <22 years old, had a diabetes duration >3 months, and had available HbA1c and diabetes technology data at the same clinical encounter. All patients at our center are offered CGM and insulin pumps, and there are no requirements for them to have failed previous therapy to be eligible for these technologies. Our insulin pump training program is a structured series of three classes. Training for CGM is less structured, and usually consists of a single, 20-min class.
Demographics, HbA1c, pump usage, and CGM usage at the most recent clinical encounter were extracted from the medical record. The practice at our center is to enter CGM and pump use data for the preceding 14 days into the record at each clinic encounter. In cases where the data were not available in the record, our study team manually reviewed every chart and directly extracted the data from the device download systems.
If technology usage was unclear at the most recent encounter, we used the preceding encounter. Pump users were defined as anyone who identified themselves as using a pump at their most recent clinic visit. CGM users were defined as patients who used a Dexcom G4, G5, or G6; a Freestyle Libre 1 or Freestyle Libre 2; or a Medtronic Guardian with a nonzero time on CGM in the 14 days preceding the most recent clinic visit. If patients had 0 time on CGM, they were classified as a blood glucose meter (BGM) user.
Patients were split into the following age groups for HbA1c comparison: <6, 6 to <12, 12 to <18, and 18 to <22. Age group cutoffs were modeled after DeSalvo, 2018. 5 Patients were also grouped according to their technology use and defined as follows: multiple daily injection with BGM (MDI/BGM), pump with BGM (pump/BGM), MDI with CGM (MDI/CGM), and pump with CGM (pump/CGM). The pump/CGM group was then further divided into those using HCL technology (defined as nonzero percent time in closed loop in the 14 days preceding the most recent clinic visit) and those using a pump and CGM without HCL.
Note that hypoglycemia prevention systems (e.g., predictive low-glucose suspend and threshold suspend) were not considered HCL for this analysis. Race/ethnicity was categorized as Hispanic, non-Hispanic white, non-Hispanic black, and other. Insurance was categorized as Medicaid, private, military plan, or other for demographic comparison, but categorized as Medicaid or not for purposes of the analysis of covariance (ANCOVA) analyses. Residence was categorized as rural or nonrural according to the Centers for Medicare and Medicaid rural zip code list (
For each of the age/technology use group categories, mean HbA1c and the proportion of participants achieving the current International Society for Pediatric and Adolescent Diabetes (ISPAD) HbA1c target of <7.0% were calculated. 15 We used ANCOVA to compare the mean HbA1c and proportion of participants with an HbA1c <7% between technology groups in each age group while controlling for race/ethnicity, diabetes duration, and insurance (Medicaid or not). The MDI/BGM group was considered the reference group for comparison. Results were presented as means with standard deviations (SDs). P-values were corrected by the Bonferroni method to account for multiple comparisons.
We also used ANCOVA to compare mean glucose, time <70 mg/dL, time 70–180 mg/dL, and time >180 mg/dL in CGM users, with the MDI/CGM group as the reference group, with the two pump/CGM groups (with and without HCL).
Linear regression was used to examine the relationship between CGM use percentage (based on the 2 weeks before the last clinic visit date) and HbA1c while controlling for diabetes duration, race, and insurance (Medicaid vs. not on Medicaid).
All analyses were performed with IBM SPSS Statistics for Mac, Version 27.0. Armonk, NY: IBM Corp.
Results
A total of 4003 pediatric patients with T1D met the inclusion criteria. The demographic features of the population are described in Table 1. The study population had a mean age of 14.5 years, diabetes duration of 6.4 years, and were 52.9% male. Among the whole cohort, 20.4% used MDI/BGM, 14.4% used pump/BGM, 15.4% used MDI/CGM, and 49.8% used a pump/CGM. Of the pump/CGM users, 35.4% used HCL technology. Only 2.6% of CGM users were using a Freestyle Libre FGM device. Of the remainder, 0.4% used a Dexcom G4, 3.9% used Dexcom G5, 78% used Dexcom G6, 11% used Medtronic Guardian, and we were unable to determine which CGM was used in the remaining 4.1%.
Demographic Characteristics Across Technology Use Groups
Mean [SD] or n (%).
Significantly different from the reference group (injections, no CGM) at a P-value of <0.01**, <0.001***.
BGM, blood glucose meter; CGM, continuous glucose monitoring; MDI, multiple daily injection; MDI/BGM, MDI with BGM; MDI/CGM, MDI with CGM; Pump/BGM, pump with BGM; Pump/CGM, pump with CGM; SD, standard deviation.
Pump/BGM users were older than the reference group (16.6 [SD 3.6] vs. 15.4 [4.1] years, P < 0.001), whereas MDI/CGM users and pump/CGM users were younger (13.6 [4.7] and 13.9 [4.4] years, respectively, both P < 0.001). Non-Hispanic white patients had the highest rate of CGM (71%) and pump (72%) use and were significantly more likely to use both a pump and CGM combined compared with no technology (P < 0.01), whereas Hispanic (50% CGM and 43% pump use) and black patients (42% CGM use and 32% pump use) were significantly more likely to use no technology than be in the pump/CGM use group (P < 0.001).
Spanish-speaking patients had the lowest pump (31.8%) and CGM (34.1%) use, and among the demographic groups evaluated, and in ANOVA comparing technology group use, they were significantly more likely to use neither pump nor CGM than to belong to any of the technology using groups (all P < 0.001). Technology use did not significantly differ based on rural versus nonrural location. Among patients with private insurance, 74% used CGMs and 74% used pumps, compared with 50% and 48%, respectively, among those who were insured by Medicaid. However, patients with both private and Medicaid insurance were more likely to be in the pump/CGM group than in the MDI/BGM group (P < 0.001).
Mean HbA1c and percentage of participants with an HbA1c <7.0% by technology use and age group are reported in Table 2 and a subgroup comparison of pump and CGM users with and without HCL is shown in Table 3. With all ages combined, the HbA1c was similar between the MDI/BGM and the pump/BGM groups (both 10.0%), whereas it was significantly lower in the MDI/CGM group (8.6%, P < 0.0001) and the pump/CGM group (8.1%, P < 0.0001) than among the MDI/CGM users. Comparing patients who used only use device (pump/BGM vs. MDI/CGM), the MDI/CGM users had a significantly lower HbA1c (10.0% vs. 8.6%, P < 0.0001). Figure 1 shows the mean HbA1c by technology use across the four age groups.
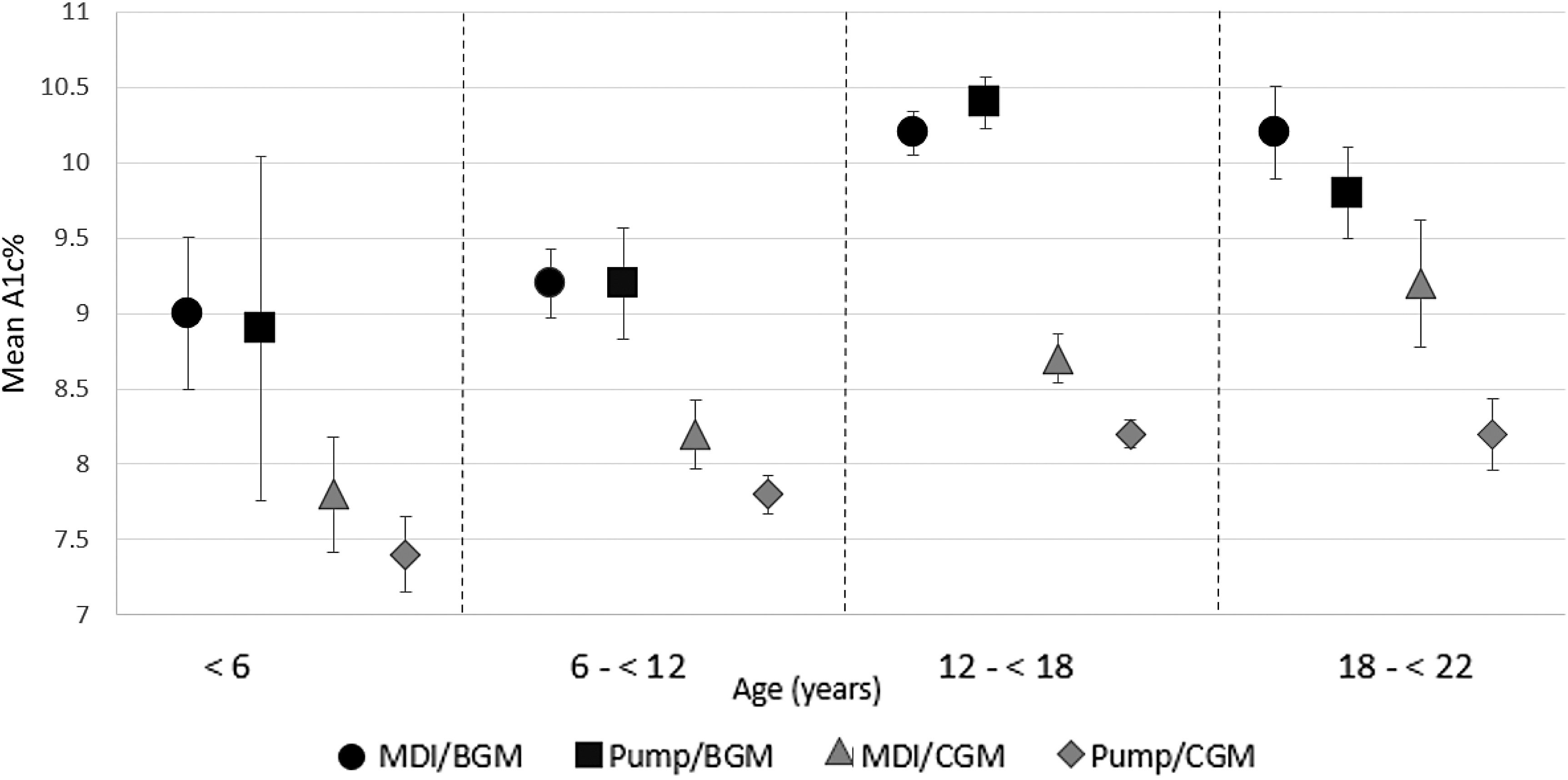
Mean HbA1c by diabetes technology use and age group compared with ANCOVA while controlling for diabetes duration, race, and insurance (Medicaid/not). Error bars represent 95% CI. ANCOVA, analysis of covariance; BGM, blood glucose meter; CGM, continuous glucose monitoring; CI, confidence interval; HbA1c, hemoglobin A1c; MDI, multiple daily injection; MDI/BGM, MDI with BGM; MDI/CGM, MDI with CGM; Pump/BGM, pump with BGM; Pump/CGM, pump with CGM.
Comparison of Mean Hemoglobin A1c [Standard Deviation] and Percent with Hemoglobin A1c <7.0% by Age and Technology Use
% meeting goal defined as proportion of patients with a current ISPAD HbA1c target of <7.0%. Controlling for diabetes duration, race, insurance (Medicaid/not). Significantly different from the reference group (injections, no CGM) at a P-value of <0.05*, <0.01**, <0.001***, or <0.0001****.
HbA1c, hemoglobin A1c; ISPAD, International Society for Pediatric and Adolescent Diabetes.
Comparison of Hemoglobin A1c Between Nonhybrid Closed-Loop Users and Hybrid Closed-Loop Users Among Pump and CGM Combined Users
Mean [SD], % with an HbA1c <7%.
% meeting goal defined as proportion of patients with a current ISPAD HbA1c target of <7.0%. Controlling for diabetes duration, race, insurance (Medicaid/not). Significantly different from the reference group (pump/CGM without HCL) at a P-value of <0.01**, <0.001***, or <0.0001****.
HCL, hybrid closed-loop.
Figure 2 and Table 3 show the mean HbA1c among pump/CGM users, comparing those who did with those who did not use HCL. Patients who were using HCL accounted for 35.4% of pump/CGM users, and they had a lower mean HbA1c than those pump/CGM users who were not on HCL (7.6% vs. 8.3%, P < 0.0001).
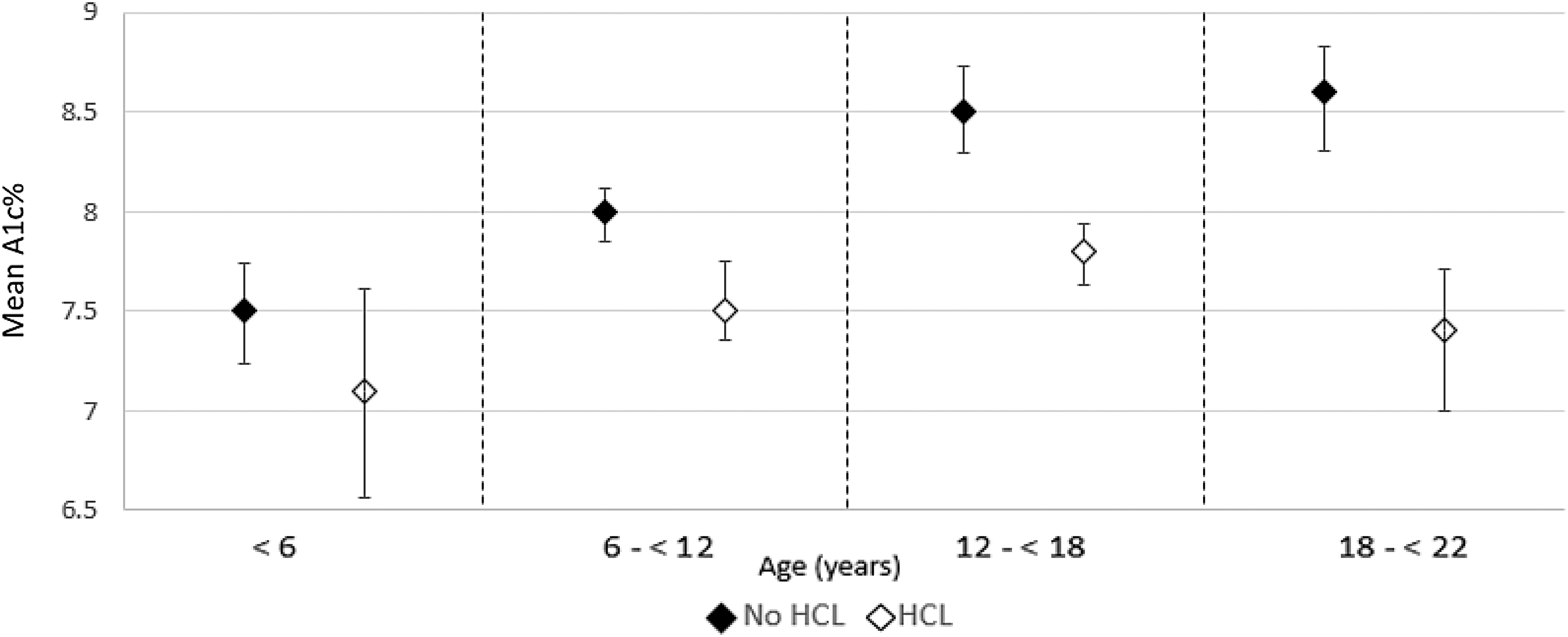
Mean HbA1c compared between pump/CGM users without HCL and pump/CGM users with HCL using ANCOVA and controlling for diabetes duration, race, and insurance (Medicaid/not). P-value is <0.0001 for comparisons within the 6 to <12, 12 to <18, and 18 to <22 years groups, but >0.05 in the <6-year age group. Error bars represent 95% CI. HCL, hybrid closed-loop.
In the entire study population, 17.6% of patients reached an HbA1c of <7%. A significantly larger proportion of patients had an HbA1c of <7% in the MDI/CGM and pump/CGM groups compared with the reference group (P < 0.0001). Pump without CGM use (pump/BGM group) was not associated with a difference in reaching an HbA1c <7% when compared with the MDI/BGM reference group. Patients who used HCL were significantly more likely to meet an HbA1c <7.0% (29.9% of the HCL group vs. 19.4% of the non-HCL pump/CGM group, P < 0.0001).
Comparison of CGM metrics between the CGM/MDI and CGM/pump groups is shown in Supplementary Table S1. Time <70 mg/dL was reduced overall in the HCL group compared with MDI/CGM and pump/CGM without HCL use (2.1% vs. 2.4% and 2.8%; P < 0.05). Mean glucose and time >180 mg/dL were lower and time 70–180 mg/dL was higher in both pump/CGM groups than in the reference group. These differences were consistently significant across all age groups in the comparison of HCL users with the reference group.
Time <70 mg/dL was lower in the pump/CGM with HCL group than in the MDI/CGM group, but not for the pump/CGM group not on HCL compared with the reference.
Linear regression showed a significant correlation between the increasing CGM use percentage among CGM users and a lower HbA1c while controlling for diabetes duration, race, and insurance (P < 0.001). There was a standardized beta weight of −0.331, meaning the variance in CGM use percent accounts for 33.1% of the variance in HbA1c. Among those with nonzero CGM use, HbA1c decreased by 0.25 for every 10% (or around 2.5 h/day) increase in CGM use percentage.
Discussion
This analysis is one of the first large, real-world, U.S. cohorts of pediatric patients with T1D evaluating HbA1c trends since the FDA approved the nonadjunctive CGM use and HCL technology. These data demonstrate that patients across the pediatric age span who used a CGM have improved glycemic control compared with patients who did not. Moreover, although insulin pump use without CGM was not associated with improved glycemia compared with patients who did not use either device, patients who use insulin pumps along with CGM did achieve a lower HbA1c and better CGM metrics compared with the reference groups. The differences in HbA1c were statistically significant in each of the age groups evaluated.
This study's finding that patients using CGM with or without an insulin pump had a lower HbA1c than those not on CGM is consistent with other research. 5,6,16 However, the relationship between insulin pump use and HbA1c has not been as consistent, with insulin pump use without CGM not appearing to add any benefit to HbA1c in our study or in a recent study evaluating outcomes in the U.S. T1D Exchange and German/Austrian Diabetes-Patienten-Verlaufsdokumentation (DPV) registries. 5 On the contrary, one recent study from the multinational Better Control in Pediatric and Adolescent Diabetes: Working to create Centers of Reference (SWEET) group, which includes many of the DPV centers and our center, reported that patients using insulin pumps without CGM had a lower mean HbA1c than those using CGM without an insulin pump. 6 Further study should be done to understand how factors such as culture, prescribing practices, and diabetes education approaches may affect these outcomes.
Patients who use HCL had a mean HbA1c 0.7% lower than those using an insulin pump and CGM but without HCL, and 10% more of these patients achieved an HbA1c of <7%, a 54% relative increase in patients meeting the goal. Although these differences in the relatively small subgroup of patients <6 years of age (n = 105) were not statistically significant, the trend and magnitude of difference were similar to the other age groups. Interestingly, even when controlling for diabetes duration and other factors, the lowest mean HbA1c (7.1%) and the highest percentage of patients achieving an HbA1c <7% (40%) were observed in children <6 years of age who use HCL technology, which is the age group in which the U.S. diabetes professionals were targeting the most permissive HbA1c targets until 2014. 17,18
The greatest difference in HbA1c with the addition of HCL to pump and CGM use was observed in patients 18 to <22 years of age, where use of HCL more than doubled the likelihood of achieving an HbA1c <7%. This is an especially encouraging finding for young adults who are in many cases just beginning to live and manage their diabetes independently. Together, these findings provide meaningful information to aid in counseling patients on the benefits of currently available technology.
There was a clear dose/response benefit with usage time on CGM, further underlining the importance for these devices to be user-friendly, comfortable, and convenient to wear, easy to prescribe, and adequately covered by commercial and public insurance plans. Unfortunately, despite the fact that people younger than age 22 insured by Colorado's Medicaid and Medicaid expansion program (CHP+) have had access to CGM technology since at least 2016, only 50.3% of these patients used CGM, whereas 73.9% of privately insured patients used CGM. The percentage of CGM use was also lower among Hispanic and black patients than in non-Hispanic white patients. In addition, despite the fact that our clinic has a robust, culturally sensitive, Spanish language Latino Clinic that strongly encourages patients to use these technologies, only 34.1% of Spanish-speaking patients in this study used CGM. Several studies have found racial and insurance disparities regarding technology use and glycemic control consistent with our data. 19 –21
It is noteworthy that non-Hispanic white race/ethnicity, private insurance, and English language were all significantly associated with a greater likelihood of being in the pump/CGM group compared with MDI/BGM, whereas Hispanic or non-Hispanic black race/ethnicity, Medicaid insurance, and Spanish language were significantly associated with the opposite pattern. Clearly, more has to be done to increase access to and acceptability of insulin pump and CGM technologies in these groups.
The findings of this study can be compared against several other recent real-world studies. The device-associated trends are similar to those documented by Foster with the T1D Exchange Registry data that ran through 2018. 2 The analysis presented here updates those findings to account for changes with factory-calibrated and nonadjunctive CGMs providing the majority of sensor data. This analysis also enables subanalysis for HCL use, which had just begun during the T1D Exchange data period analyzed by Foster.
Breton and Kovatchev have published a recent large analysis of Tandem Control-IQ data from the Tandem t:connect server. 22 The Breton article demonstrates similar time-in-range data for HCL school-aged children, and a higher time-in-range for adolescents while also providing excellent time-in-range data for adults and elderly adults. Our analysis adds to this picture with data on children 2–5 years old, which was not presented in the Breton analysis. This analysis also includes biological HbA1c measurements that are not available via device-only data from t:connect. Da Silva recently published a similar registry analysis for 4120 Medtronic 780G users across Europe, South Africa, and Qatar. 23 This HCL system is conformitté Européenne (CE) marked for people 7–80 years old, although age data were not available for the Da Silva analysis.
The Da Silva analysis demonstrated higher time-in-range values than for this analysis, likely as a result of a predominantly adult population. Notably, initiation of HCL was associated with a 12.1% increase in time-in-range, which is similar to the 14.8% difference seen in this analysis for HCL versus pump/CGM without HCL.
The strengths of this study include the large patient sample, use of the conservative Bonferroni method to correct for multiple comparisons, data completeness, and the fact that this is one of the first studies evaluating real-world outcomes by technology use since the recent advances in the field.
The limitations include the retrospective, single-center design that may reflect local practices rather than national trends. Also, we did not have reliable data available to report incidence of diabetic ketoacidosis or severe hypoglycemia in our cohort. Unlike research registries such as the T1D Exchange and DPV, we did not have access to socioeconomic factors such as parental education level and family income. These are important factors that should be considered when aiming to increase technology use.
In conclusion, this study demonstrates that pediatric patients with T1D are more likely to have a lower mean HbA1c and achieve an HbA1c goal of <7% if they use CGM technology, pump and CGM technology combined, or HCL technology, with the HCL group achieving the best glycemic control. These results can inform patient counseling regarding technology use and choice to achieve the best clinical outcomes. In addition, racial, language, and insurance disparities in technology use continue to exist and should be examined further to identify how best to address barriers to technology use given the clear benefit in glycemic control.
Footnotes
Authors' Contributions
A.S. researched the data, performed the statistical analyses, and drafted the article. M.S. and G.T.A. researched the data and reviewed and edited the article. G.P.F. researched the data, reviewed the article, and contributed to the discussion. G.P.F. and G.T.A. are the guarantors of this work and, as such, had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Acknowledgment
We thank Bing Wang for database support. These data have been presented in a virtual poster format at the ISPAD meeting in October 2021.
Ethical Approval
This study was determined by the Colorado Multiple IRB (20-2686) to meet the criteria for exemption from IRB review (category 4, secondary research). All criteria were met for a full waiver of Health Insurance Portability and Accountability Act of 1996 authorization.
Author Disclosure Statement
G.P.F. conducts research sponsored by Medtronic, Dexcom, Abbott, Tandem, Insulet, Lilly, and Beta Bionics and has been a speaker/consultant/advisory board member for Medtronic, Dexcom, Abbott, Tandem, Insulet, Lilly, and Beta Bionics. A.S., M.S., and G.T.A. have no conflicts of interest to report.
Funding Information
Supported by the University of Colorado Diabetes Research Center Clinical Resources Core NIH, NIDDK grant P30-DK116073 and the National Institute of Diabetes and Digestive and Kidney Diseases, NIDDK grant 5T32DK063687-17.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.