
Abstract
We aimed to evaluate the glycemic effect and detect any predictors of improved time-in-range (TIR) in persons with type 1 diabetes after initiating hybrid closed-loop (HCL) treatment with MiniMed 670G in a 12-month retrospective observational study. Before starting HCL treatment, the 62 participants followed a Steno-developed training program; 7 participants (6.5%) discontinued the HCL therapy; the remaining 55 (58% female) had an age (mean ± standard deviation) of 45.6 ± 12.6 years and diabetes duration of 28.2 ± 10.9 years. After 12 months' HCL therapy, glycated hemoglobin A1c decreased from 7.4% +0.7% to 7.1% +0.5%, TIR increased from 59.3% ± 13.5% to 72% ± 9.3%, time in 54–70 mg/dL (3.0–3.9 mM) decreased from 2.4% ± 2.0% to 1.4% ± 1.0%, and time in 180–250 mg/dL (10.0–13.9 mM) decreased from 26.4% ± 8.3% to 20.8% ± 5.5%, all P < 0.001. Improvement in TIR was significantly associated with lower total daily insulin dose, higher amount of total carbohydrate, and more time spent in Auto Mode. Our findings support the promising results on glycemic outcomes seen with HCL treatment.
Introduction
An overall goal of diabetes management is achieving good glycemic control to prevent diabetes complications, thereby minimizing hypoglycemia and reducing diabetes distress. 1 However, despite the technological advances in therapy, most persons with type 1 diabetes (T1D) cannot attain satisfactory glucose levels and risk acute and chronic diabetes complications. 2
The hybrid closed-loop (HCL) system is a technology that automatically adjusts insulin delivery from insulin pumps using real-time data from continuous glucose monitors (CGMs). All closed-loop systems on the market are hybrid systems, where users are required to estimate and enter carbohydrate content for meal bolus insulin. The MiniMed 670G was the first approved HCL system, launched in the United States in 2017 and available in Denmark from January 2019. Randomized controlled trials reveal promising results for HCL systems, improving the time-in-range (TIR) and glycated hemoglobin A1c (HbA1c). 3 –5 However, publications are limited concerning real-world studies on the MiniMed 670G system, 6 –10 and details are lacking the training methods used when initiating the system.
We aimed to evaluate the glycemic effects of 12 month's MiniMed 670G therapy in T1D and determine predictors of HCL-induced changes in TIR. Furthermore, we include a detailed description of our training program for HCL therapy initiation.
Materials and Methods
Study design and participants
We undertook a 12-month retrospective observational study in adults with T1D who changed from their current sensor-augmented insulin pump system (SAP) to MiniMed 670G at Steno Diabetes Center Copenhagen during March 2019–June 2020. All participants attended the locally developed 670G-education program and gave permission to collect data from their electronic medical records and insulin pump uploads before, during, and after 12 months' HCL therapy. Participants were offered an HCL if their current insulin pump's warranty had expired, they usually used carbohydrate counting and the pump bolus calculator, and they had chosen to initiate the MiniMed 670G system.
The functionalities of the MiniMed 670G are extensively described elsewhere. 11,12 The study was conducted according to the Helsinki Declaration and was approved by the Regional Data Protection Agency (P-2020-795).
Training program
Our 670G-training program comprised two group sessions 2 weeks apart, followed by a telephone consultation and a physical consultation. Each session was attended by five to seven participants and three educators specialized in diabetes technology—a diabetologist, a diabetes nurse, and a dietitian. The educational methods combined information sessions, hands-on practice, interactive discussions between participants, and short individual consultations with the educators. See Supplementary Table S1 for the detailed education program.
In the first session (3½ h), a Medtronic employee introduced the MiniMed 670G HCL system from a technical perspective. Then the educators covered practical features, how to operate the system, how to analyze any need for changes in insulin pump settings, and training in carbohydrate counting. The participants programed and started the HCL in Manual Mode (MM). After 1 week, they were instructed in switching to Auto Mode (AM) and completed 3-day worksheets, recording food intake, estimated carbohydrate content, and physical activity.
The second session (2½ h) was 1 week after AM initiation. Uploads and worksheets were analyzed individually, and insulin pump settings and functioning with the HCL were adjusted if necessary. The education focused on advancing skills in carbohydrate counting and managing physical activities, sick days, and so on.
After 2 weeks in AM, participants uploaded the pump data for analyzes. If the participant or diabetologists deemed it necessary, an additional telephone consultation was scheduled. A second physical consultation was arranged with a diabetologist a month after the 670G-system start. Thereafter, participants followed the outpatient appointment plan and continued their everyday activities.
Data
Clinical data
Data on age, gender, diabetes duration, weight, body mass index (BMI), and HbA1c were extracted from the electronic medical records. If available, weight and BMI data were collected at four timepoints after HCL start. HbA1c data were obtained before and at five timepoints after HCL start (Table 1).
Glucose Control, 670G Characteristics and Settings at Baseline and During the First Year with 670G Hybrid Closed-Loop
Baseline; 1–6 months before 670G. Results are presented as mean ± SD; P-values represent changes from baseline to the five timepoints; 1–3, 3–5, 12–16, 20–28, and 52 weeks after 670G.
BMI, body mass index; CIR, carbohydrate–insulin ratio; HbA1c, glycated hemoglobin A1c; NA; TAR, time above range; TBR, time below range; TDD, total daily insulin dose; TIR, time-in-range; SD, standard deviation.
Pump settings and CGM data
The main study results cover 14 days' upload: percentage of time spent in AM (%), time in CGM range 70–180 mg/dL or 3.9–10 mM (TIR), time below 70 mg/dL or 3.0 mM (TBR1), time below 54 mg/dL or 3.9 mM (TBR2), time above 180 mg/dL or 10.0 mM (TAR1), time above 250 mg/dL or 13.9 mM (TAR2), total carbohydrate intake (grams/day), bolus/basal (%), total daily insulin dose (TDD) (IE), insulin activity (h), and carbohydrate–insulin ratio (CIR) divided into breakfast (06:00–11:00), lunch (11:00–17:00), and dinner (17:00–20:00).
Pump and CGM data before HCL initiation were extracted from Diasend (Glooko, CA) and Carelink Professional (Medtronic, CA), depending on the device.
Data after HCL initiation were collected from Medtronic Carelink Personal (Medtronic, CA). Data were collected at five points: 1, 2–4 weeks’, 2–4, 5–7, and 12 months' HCL therapy.
Statistical analyses
Statistical analyses were performed with the SPSS software for Windows, version 22.0 (IBM Corp., Armonk, NY) and SAS 9.4 M5 (SAS Institute, Inc.). Analyses included standard descriptive statistics of the population. Data are presented as mean with standard deviation (SD) or percentage. Paired t-test and linear mixed model with random intercepts were used to compare insulin pump data and clinical data from baseline to the five timepoints.
Results
Participants
The MiniMed 670G training course included 62 participants; 4 (6.5%) stopped using MiniMed 670G during the study because of pregnancy (n = 1) or dissatisfaction with the system [n = 3: difficulties managing glycemia around exercise (n = 1) and increasing HbA1c levels after HCL start (n = 2)]; 3 (4.8%) were excluded from the data set due to missing data (Supplementary Fig. S1). The remaining 55 participants (58% female) were included in the data analyses—mean ± SD age 45.6 ± 12.6 years and mean duration of diabetes 28.2 ± 10.9 years. Before MiniMed 670G, 31 participants (50%) used a MiniMed 640G, 28 (45%) a Paradigm 522/722/554/574 and 3 (4.8%) an Animas pump; 10 (16.1%) participants used FiAsp® (Novo Nordisk, Bagsvaerd, Denmark), 2 (3.2%) Humalog® (Eli Lilly, Indianapolis, IN), and 43 (69.4%) NovoLog® (Novo Nordisk) in the pump. At the time of data extraction, 37 of the 55 participants had used the 670G pump for 12 months (Supplementary Fig. S1).
Glycemic and metabolic effects
From baseline to study end, HbA1c decreased from 7.4% +0.7% to 7.1% +0.5%, TIR increased from 59.3% ± 13.5% to 72% ± 9.3%, TBR1 decreased from 2.4% ± 2.0% to 1.4% ± 1.0%, TBR2 decreased from 0.5% ± 0.8% to 0.3% ± 0.5%, TAR1 decreased from 26.4% ± 8.3% to 20.8% ± 5.5%, and TAR2 from 11.5% ± 8.5% to 5.8% ± 4.6% (all P < 0.001) (Table 1 and Fig. 1). No changes were seen in TBR1 (P = 0.54) and BMI (P = 0.34) during the treatment period (Table 1).
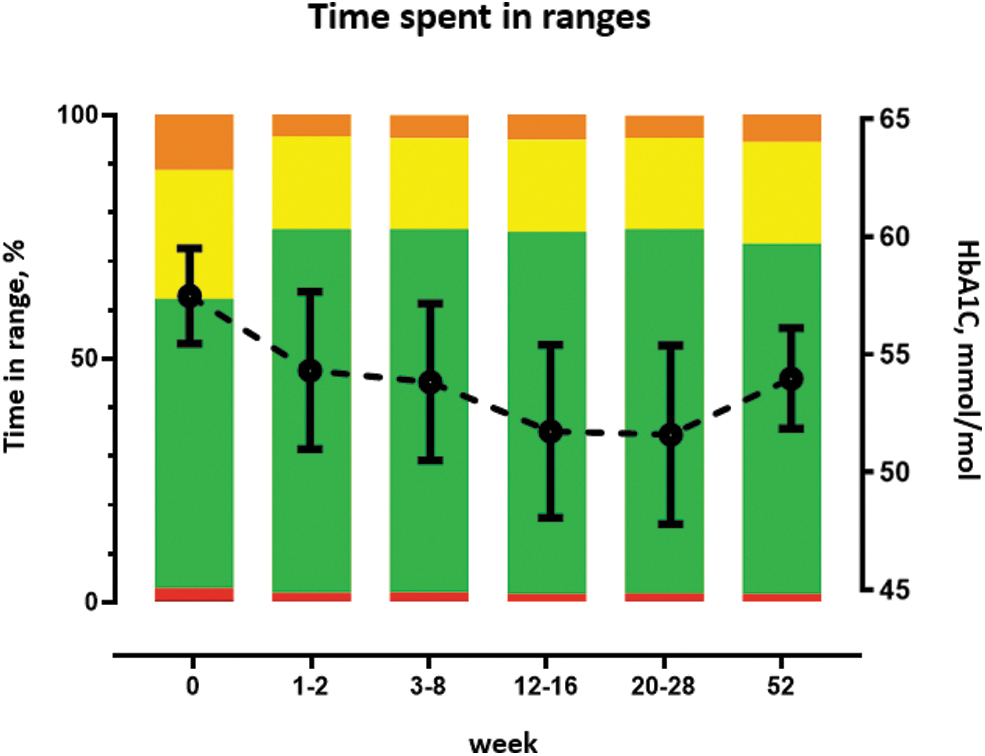
Time spent in ranges at baseline (1–6 months before 670G), and at the five timepoints during the first year with 670G HCL. HCL, hybrid closed-loop.
Change in settings
Changes in insulin pump settings during the observational period appear in Table 1. The following parameters changed significantly: percentage of bolus insulin increased, CIR for all meals was lower, and insulin action time was lower. In addition, the amount of carbohydrate entered into the system increased and meals per day decreased.
Predictors of improved TIR
The multivariable analysis showed that the TIR increased 0.21% (95 CI%: 0.10–0.34) per 1 unit decrease in TDD (P < 0.001), by 0.05% (0.01–0.08) per 1 g increase in carbohydrate intake (P = 0.02) and increased by 0.15% (0.06–0.23) per 1% increase in time in AM (P = 0.001). No association was found between change in TIR and changes in percentage of bolus/basal insulin, insulin action time, and meals per day (Supplementary Table S2).
Discussion
This real-world clinical observational study demonstrated that initiating MiniMed 670G together with a 6-h training course resulted in improvements in HbA1c of 0.43% (4.7 mmol/mol) and in TIR of 12% to 72% after 12 months' treatment. This supports results from shorter real-world studies. 5 –9 A recent 12-month study of data from European Carelink adult users starting MiniMed 670G showed a comparable achievement of 72% TIR 10 and an increase from baseline of ∼9%. Our results showed an even higher increase in TIR from baseline to 12 months, supporting that any increase in TIR partly depends on the baseline value, which was lower in our population than in the registry study.
TBR and TAR decreased from baseline and met the treatment goals 13 after 1 week of HCL use, remaining stable for 12 months. Similar to the MiniMed 670G pivotal trial 14 and the European Carelink study, our real-world clinical study detected a clinically relevant decrease in HbA1c to 7.1% (54 mmol/mol). Furthermore, our study provides specific modifiable factors for the glycemic improvements achieved with the MiniMed 670G system. This new knowledge is relevant for clinical use.
The main predictors of increased TIR were lower TDD, a greater amount of total carbohydrate, and more time spent in AM. We found no significant change in TDD over time despite a 20-g increase in the total amount of carbohydrate per day from baseline to 12 months. This suggests the participants improved their carbohydrate counting, supported by a higher bolus percentage. For pump settings, CIR was reduced for all meals and insulin action time was reduced after initiating HCL therapy. The reduction in CIR is shown in studies with HCL in adolescents, reporting a CIR reduction of 20%. 15 –17
However, it is questionable whether the amount of carbohydrate at baseline, in this study, is representative of the amount of carbohydrate eaten. After 1–3 weeks' HCL therapy, the mean amount of carbohydrates increased by 50 g per day. Therefore, participants were more likely to have optimized their carbohydrate counting skills due to the carbohydrate counting training than to have changed their diet. 18,19 However, no questionnaire or qualitative data were collected for this purpose. Nevertheless, this emphasizes the importance of patient training run parallel with HCL system initiation for a successful start, especially since a higher amount of carbohydrate entered into the pump is a predictor of TIR improvement.
This is supported by findings in McAuley et al. where the HCL group underwent intensive education in carbohydrate counting, diabetes self-management and CGM use (configuration and responding to alarms). Their results showed similar glycemic improvements with TIR increased by 15%–70% and HbA1c decreased by 0.4% [4.0 mmol/mol]. 5 In addition, McAuley et al. measured diabetes-specific well-being and diabetes-specific quality of life. Both increased significantly in the HCL group compared with the control group reflecting current clinical practice. The third identified predictor of an increase in TIR was time spent in AM; on average, our participants spent 90% during the 12 months' observation. This agrees with previous studies similarly demonstrating the importance of a high percentage of time in AM. 10,20,21
The strengths of this study were the length of the observation period and the low dropout rate. Other studies have reported sensor problems as the main reason for discontinuing the 670G HCL pump. 17,22 Our participants were not specifically asked to report sensor problems, but the prolonged time in AM and a dropout rate <7% indicate few problems with the sensors. One possible explanation is that participants initiated HCL from SAP; therefore, all had sensor experience.
The study has some limitations. It is a single-center study without a control group. As the follow-up was during the Covid-19 pandemic, some outpatient visits were canceled and some data were missing, but this was accounted for in the statistical analyses. The study group was representative of the Steno Diabetes Center Copenhagen's insulin pump population (n = 1500) regarding age, gender, and HbA1c 23 ; however, the number of previous users of a Medtronic pump system was higher among our participants in the present group, which may have led to the impression of few sensor problems. Moreover, the study group were first-movers on this technology and might have been particularly motivated for a successful outcome. This could also be a selection bias regarding the low dropout rate. We did not evaluate the training program itself, but similar studies conclude the importance of training and education of HCL users and have not found differences between different programs regarding glycemic outcome. 5,14,16,22,24
Conclusion
This 12-month clinical observational study confirms the promising improvement in glycemic outcomes seen in the initial trial, shorter observational studies, and a Carelink registry study with this first-on-the-market HCL pump: MiniMed 670G. Predictors of the improvement in TIR are low TDD, higher amount of total carbohydrate, and increased time spent in AM. These factors could be key when initiating 670G HCL therapy—and maybe other HCL systems. Our results also suggest changing the insulin pump settings to lower insulin action time and lower CIR along with a planned relatively short patient training program.
Footnotes
Authors' Contributions
S.S.J. and K.N. planned the study. S.S.J. wrote the article. E.H., A.G.R., and K.N. reviewed and edited the article. S.S.J. collected data. A.G.R. and S.S.J. conducted the statistical analyses.
Acknowledgments
The authors thank the participants for consenting to use of their data.
Author Disclosure Statement
K.N. received funding for her institution for participating in advisory boards from Medtronic and Novo Nordisk and for lecturing from Sanofi, Novo Nordisk, Medtronic, and Dexcom. Her institution received funding for studies she performed from Zealand Pharma, RSP Systems, Novo Nordisk, Medtronic, and Dexcom.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.