
Abstract
Background:
Although insulin pump infusion set failures are common, studies assessing the failure rate are limited.
Methods:
Data were analyzed from two clinical trials, in which 263 participants aged 6–72 years used 22,741 infusion sets. The frequency of removal due to prolonged hyperglycemia (continuous glucose monitor measuring >300 mg/dL immediately before removal and >250 mg/dL continuously for at least 2 h before removal with at least 90 min >300 mg/dL out of the prior 120 min) was determined. Differences in failure rates among age groups and infusion set types were evaluated.
Results:
Among 22,741 infusion sets, 748 (3.3%) were removed before 72 h in association with prolonged hyperglycemia. The percentage replaced within 48 h and within 24 h with prolonged hyperglycemia were 1.8% and 1.0%, respectively. Mean duration of continuous time >250 mg/dL before removal was 5.1 ± 3.7 h. Using a less restrictive definition of failure related to hyperglycemia, 1688 (7.4%) sets were removed before 72 h with a glucose level >300 mg/dL at the time of removal. The frequency of insulin set failure with prolonged hyperglycemia was lower in adults ≥18 years old (1.9%) than in those 14–17 years old (5.8%, P < 0.001) or 6–13 years old (4.4%, P = 0.002). The 90° Teflon sets had the highest frequency of prolonged hyperglycemia failure within 72 h (4.0%) compared with the angled Teflon set frequency (1.3%, P = 0.01) or the steel set frequency (1.9%, P = 0.006).
Conclusions:
Based on the data from these 22,741 infusion sets, infusion set changes associated with prolonged hyperglycemia occur on average about four times a year, with the frequency being higher in youth than adults. The frequency also appears to be higher with straight Teflon sets compared with angled Teflon sets and steel sets. Clinical Trials Registration Number: NCT03563313.
Introduction
Although it has long been recognized in clinical practice that infusion set failures occur frequently in insulin pump users, there have been few studies that have evaluated the optimal duration of infusion set wear and the frequency of premature failure. 1 The recommendation to change the infusion set every 2–3 days has been based on anecdotal reports and clinical experience dating back to the early 1980s. 2
Prolonged hyperglycemia due to inadequate insulin delivery is a common reason for early infusion set replacement. 3 Often the source of the problem can be attributed to the initial insertion. 4 Studies specifically evaluating pump infusion sets have reported that 4.6%–15% of infusion sets fail related to hyperglycemia within 3 days of insertion. 4 –6
We utilized data from two completed clinical trials of a hybrid closed loop system to determine the frequency of infusion set changes associated with a preceding prolonged period of hyperglycemia and to assess whether any differences exist in failure rates comparing adults versus youth and comparing different types of infusion sets (steel vs. Teflon and straight vs. angled Teflon).
Methods
The analyses utilized data from two studies, in which participants were using a closed loop system consisting of the Tandem t:slim X2 insulin pump with Control-IQ Technology and a Dexcom G6 sensor. One study included the extension phase (13–58 weeks) of the Control-IQ pivotal trial for participants 14–72 years old 7 and the other was the Control-IQ randomized trial plus extension phase totaling 28 weeks for participants 6–13 years old. 8 In both studies, participants were asked to change their infusion set every 48–72 h. The protocols were approved by a Central Institutional Review Board, and written informed consent and assent for those <18 years old were obtained.
Each participant was categorized based on the type of infusion set used: either use of only one type throughout (90° Teflon, angled Teflon, steel) or multiple types of infusion sets. If multiple types of infusion sets were used, it was not possible to determine when each type was used (therefore, such participants were categorized separately). The specific infusion sets that were included in each category are listed in Supplementary Table S1.
Infusion set changes were identified from pump data downloads. An infusion set change was assumed to have occurred if the pump data reported a completed tubing prime followed by the pump resuming delivery of insulin. For each infusion set changed within 72 h of insertion, the association of the infusion set removal with hyperglycemia was determined provided there was sufficient continuous glucose monitor (CGM) data available during the 2 h before removal (defined as having no more than 15 min gap between readings) and a value present within 10 min before removal.
Classifying the removal as being associated with hyperglycemia required that CGM glucose was >300 mg/dL immediately before removal and was >250 mg/dL continuously for at least 2 h before removal with at least 90 min >300 mg/dL out of the prior 120 min (referred to as “prolonged hyperglycemia failures”). An alternate failure definition required only if the glucose was >300 mg/dL at the time of removal (referred to as “hyperglycemia failures”).
Frequency of failures were computed for a 72-h period, 48-h period, and 24-h period from time of insertion overall, for three age groups (6–13, 14–17, and ≥18 years, old) and for four groupings of infusion set use (sole use of 90-degree Teflon, angled Teflon, or steel; or use of multiple types).
Differences in failure rates across age groups, infusion set types, and baseline HbA1c were evaluated using a logistic regression model with age and infusion set type included as categorical covariates and baseline HbA1c as a continuous covariate. The model also included a random intercept term to account for within-subject correlation. Odds ratios (ORs) and 95% confidence intervals (CIs) for pairwise comparisons of age groups and infusion set types and for the effect of a 1 U increase in HbA1c were estimated from this model.
Results
The analysis included data from 263 study participants (123 ≥ 18 years old, 40 14–17 years old, and 100 6–13 years old). Participant characteristics according to age group are shown in Supplementary Table S2.
In the analysis dataset, there were 25,154 infusion set wears. The mean number of infusion sets per participant was 96 ± 44. Mean wear duration was 2.9 ± 1.3 days: 2.9 ± 1.2 days in 6–13 years old, 2.6 ± 1.1 in 14–17 years old, and 3.0 ± 1.3 in those ≥18 years old (Supplementary Table S3).
Among the 22,741 infusion sets with sufficient CGM data for analysis, 748 (3.3%) had prolonged hyperglycemia before removal within 72 h (Table 1). The percentage replaced within 48 and 24 h with prolonged hyperglycemia were 1.8% and 1.0%, respectively. One hundred fifty-two (58%) of participants had at least one removal within 72 h associated with prolonged hyperglycemia. The mean duration of time that CGM glucose was continuously >250 mg/dL before an infusion set change associated with prolonged hyperglycemia was 5.1 ± 3.7 h and consistent among age groups (Table 2). Using a less restrictive definition of failure related to hyperglycemia, 1688 (7.4%) sets were removed before 72 h with a glucose level >300 mg/dL at the time of removal (Supplementary Table S4).
Infusion Set Removal Associated with Prolonged Hyperglycemia
This table only includes infusion set wears with a CGM reading in the 10 min before the infusion set removal and where the gap between CGM readings in the 2 h before the infusion set removal was no more than 15 mins. n = 2413 infusion wears were excluded because they did not meet these criteria.
Defined as infusion set removals meeting the following criteria: (1) CGM >300 mg/dL immediately before the infusion set removal, (2) CGM continuously >250 mg/dL in the 2-h period before the infusion set removal, and (3) CGM >300 mg/dL for at least 90 min of the 2-h period before the infusion set removal.
CGM, continuous glucose monitor.
Time >250 mg/dL for Infusion Set Removals in the Interval 0–<72 h Associated with Prolonged Hyperglycemia
SD, standard deviation.
The frequency of prolonged hyperglycemia failure within 72 h was 1.9%, 5.8%, and 4.4% among those aged ≥18 years, 14–17 years, and 6–13 years, respectively (Table 1, Figs. 1 and 2). After adjusting for infusion set type and baseline HbA1c, the odds of prolonged hyperglycemia failure within 72 h were significantly higher in the 14–17-year-old age group (OR 2.4 [95% CI 1.6–3.7], P < 0.001) and in the 6–13-year-old age group (OR 1.8 [95% CI 1.2–2.6], P = 0.002) compared with the ≥18-year-old age group.

Percent of infusion sets replaced following prolonged hyperglycemia within 72 h of insertion.

Kapalan-Meier curves of time to infusion set removal following prolonged hyperglycemia by age group. Infusion sets removed within 72 hr of insertion that were not associated with prolonged hyperglycemia were considered censored data.
The 90° Teflon sets had the highest frequency of prolonged hyperglycemia failure within 72 h (4.0%) compared with the angled Teflon frequency (1.3%) (OR 2.0 [95% CI 1.2–3.3, P = 0.01) or the steel frequency (1.9%) (OR 1.8 [95% CI 1.2–2.8], P = 0.006) (Fig. 3). Results generally were similar during the first 48 h and first 24 h (Table 1).
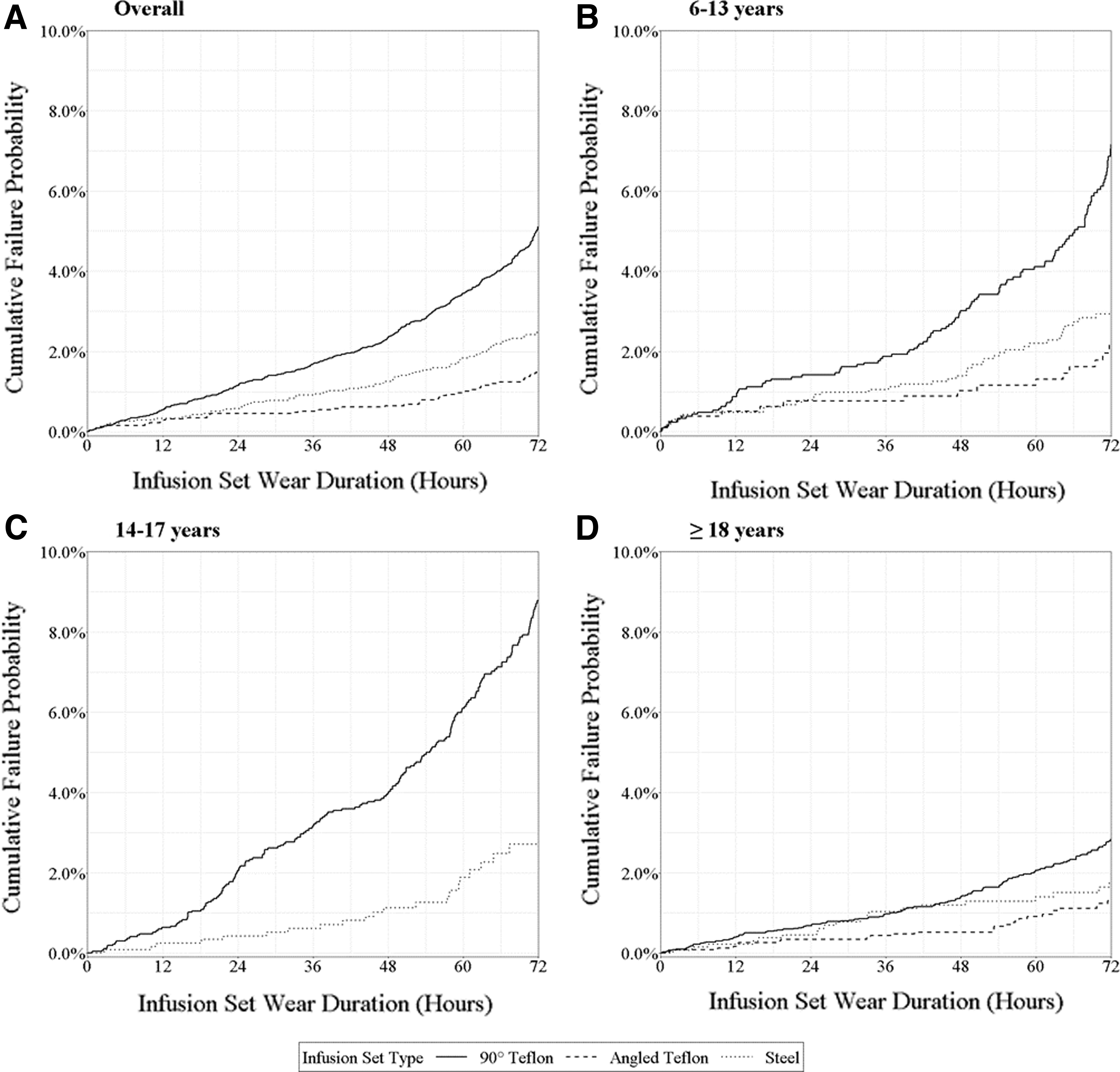
Kaplan–Meier curves of time to infusion set removal following prolonged hyperglycemia by infusion set type and age group. Infusion sets removed within 72 hr of insertion that were not associated with prolonged hyperglycemia were considered censored data.
In addition, higher HbA1c at baseline was associated with higher odds of prolonged hyperglycemia failure within 72 h (OR based on a 1.0% increase in HbA1c = 2.1 [95% CI 1.8–2.5], P < 0.001). When an interaction term for HbA1c by age group was added to the model, higher HbA1c was associated with higher odds of prolonged hyperglycemia failure within all three age groups.
Discussion
In this analysis of more than 22,000 infusion set wears, 7.4% of sets were removed before 72 h associated with a CGM glucose >300 mg/dL and 3.3% met criteria for prolonged hyperglycemia for at least 2 h before removal. Infusion set removals related to prolonged hyperglycemia were substantially lower in adults than in youth and slightly higher in adolescents (14–17 years old) than in younger children (6–13 years old). In addition to age, a higher frequency of hyperglycemia-associated infusion set changes was associated with higher HbA1c levels, suggesting that patient factors may contribute to premature infusion set failures.
Straight insertion Teflon sets were the most commonly used type of infusion set in all three age groups, but they had a higher failure rate than either Teflon sets with an angled insertion or steel sets. The observed prolonged hyperglycemia failure rate was higher in participants who used multiple types of infusion sets, likely related to premature failures with one type of infusion set leading to a switch to another type.
While it is possible that in some instances, the hyperglycemia could have been due to a cause other than infusion set failure and the infusion set could have been removed for a reason other than hyperglycemia, it seems unlikely that this was the case for very many of the 413 infusion set changes associated with prolonged hyperglycemia that were made less than 48 h from insertion. More likely, our estimate of a 3.3% infusion set failure rate due to hyperglycemia is an underestimate since an additional 4.1% of infusion sets were removed before 72 h with a glucose level >300 mg/dL that did not meet our definition of prolonged hyperglycemia and some of these undoubtedly would have had sustained hyperglycemia if the infusion set had not been changed.
In addition, all participants were using an AID system, which would have minimized the occurrence of prolonged hyperglycemia if the infusion set was functioning.
While the percentage of infusion sets replaced within 72 h associated with hyperglycemia is low, it still represents about four failures per year on average for each pump user based on our prolonged hyperglycemia definition and 9 per year based on an association with hyperglycemia alone. This number of failures is meaningful considering that with each prolonged hyperglycemia failure, the mean time above 250 mg/dL exceeded 5 h and each episode carries the risk of development of diabetic ketoacidosis.
The clinical impression that infusion set failures due to hyperglycemia are common is supported by survey and observational study data. A type 1 diabetes (T1D) Exchange survey found that 86% of 243 adults with T1D using an insulin pump reported having at least one early infusion set change due to hyperglycemia in the prior 3 months and 40% reported having three or more such events per 3 months. 9 Rabbone et al. 3 reported results of an observational data collection study on 1046 youth with T1D (99% of whom were using Teflon infusion sets—78% with 90° insertion, and 22% with oblique insertion), in which the failure rate associated with hyperglycemia can be estimated to be ∼7%. The failure rate was higher with straight insertions than oblique insertions, consistent with our findings.
There are a few clinical trials conducted to evaluate infusion set wear in pump users with T1D, which provide data that can be used to estimate the failure rate due to hyperglycemia within the first 3 days of wear. Patel et al. conducted a randomized crossover trial to compare Teflon versus steel infusion sets (Teflon: Quick-set with 90° angle vs. Steel: Sure-T, 90° angle) in 20 study participants aged 12–41 years. 4 Failure due to hyperglycemia required blood glucose >300 mg/dL and (1) not decreasing by at least 50 mg/dL an hour after a correction bolus or (2) a blood ketone level >0.6 mmol/L.
During the first 3 days, none of the steel sets failed while 15% of the Teflon sets met this failure definition, all on the first day and with kinking identified on removal. Thrasher et al. reported the frequency of infusion set occlusions defined as plasma glucose ≥300 mg/dL with failure to reduce the glucose level by at least 50 mg/dL within 60 min by insulin bolus via the pump in 27 adults using their own insulin pumps and infusion sets. 6 Assuming sets were changed on average every 3 days, the failure rate with hyperglycemia meeting the above definition can be estimated to be 4.6%. Freckman et al. evaluated two soft cannula infusion sets (Accu-Chek FlexLink and Accu-Chek FlexLink Plus) in 80 adults. 5
Mean time of infusion set wear was 2.5 days and ∼8% of infusion sets were removed early due to hyperglycemia. Thus, the prior literature suggests that the infusion set failure rate within 72 h impairing insulin delivery and resulting in hyperglycemia is 4.6%–15%. Using a definition of glucose >300 mg/dL at the time of set change, our results fall in this range, while using our definition of prolonged hyperglycemia, our results fall below this range. However, even with this definition, we may still be underestimating the frequency of infusion set failures since our cohort comprised hybrid closed-loop users, some of whom might identify infusion set failure at lower glucose levels.
A strength of this study is in the large number of infusion set wears included in the analyses. Although the analysis utilized data from clinical trials, it seems likely that the data are consistent with real-world experience, since the infusion sets were the same types used in usual care outside of a study. Our dataset included infusion sets used just with the Tandem t:slim X2 insulin pump, but there is no indication that the infusion set failures were related to the pump per se and a similar failure rate would be expected with any pump using these infusion sets. One limitation, although unlikely to impact the results due to the strict criteria that were used, is that we have made an assumption, when prolonged hyperglycemia was present, that this was the reason for infusion set change. In addition, unlike studies formally designed to evaluate infusion set failure rates, we did not include elevated blood ketone levels in our criteria for infusion set failure.
Based on the data from 22,741 infusion sets, infusion set changes associated with prolonged hyperglycemia occur on average about four times a year, with the frequency being higher in youth than adults. The frequency also appears to be higher with straight Teflon sets compared with angled Teflon sets and steel sets.
Footnotes
Authors' Contributions
L.G.K., J.W.L., and R.W.B. researched data and wrote/edited the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Supported through the Jaeb Center for Health Research.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.