
Abstract

Sensor-augmented insulin pump therapy is quickly moving to various stages of automated insulin delivery (AID) when the insulin pump and the continuous glucose sensor is combined with a control algorithm. 1 According to the recent consensus report for treatment of type 1 diabetes (T1D), AID offers increased flexibility and lower risk of hypoglycemia, but with highest costs between the considered regimens. 2 AID should be suggested for all people if glycemic targets are not met and the person with diabetes wishes to change insulin therapy.
Several studies using different systems of AID have reported that many people with T1D are achieving recommended treatment targets 3,4 with time in range (TIR) being on average slightly >70% with a low time below range 5 and concomitant improvements of patient-related outcomes. 6 –8 Hybrid closed-loop systems are the most effective in achieving better glucose control during the night but continue to require considerable patient effort to minimize glycemic variability and achieve a high TIR 5 and a high time in tight range (70–140 mg/dL for targets closer to the physiological range, according to Danne et al 9 ) particularly related to meals.
Several sodium-glucose cotransporter inhibitors (SGLTi) have been investigated as adjunctive therapy for people with T1D. They provide an insulin-independent approach to lower serum glucose by inhibition of tubular reabsorption from primary urine. There are different substances available: most are SGLT2-inhibitors, but also combined SGLT1 and SGLT2 inhibitors are also under investigation. 10 In this first free-living trial combining low-dose SGLTi with a commercial AID or predictive low glucose suspend (PLGS) in an 8-week randomized controlled crossover trial, Garcia-Tirado et al 11 provide evidence that we can expect the multitude of benefits of SGLTi also in addition to the most advanced form of insulin delivery.
Several T1D trials have shown a 2–4 mmol/mol (0.2%–0.4%) HbA1c improvement without an inherent risk of hypoglycemia, a moderate improvement in body weight (2–3 kg), and systolic blood pressure (3–4 mmHg decrease). 12 –16 The randomized trial achieved on average 80% TIR both with PLGS and AID as the addition of 5 mg daily empagliflozin significantly improved daytime glucose control.
This was also the case in another study using this new dual approach with empagliflozin in an AID setting. It was shown that counting carbohydrates and entering them correctly into the AID device led to a 14% higher postprandial glycemic control measured by TIR. Although empagliflozin added to AID had the potential reduce the need for carbohydrate counting, in line with the study results, it does not allow for the elimination of meal announcement. 17 Previously, a small single-SGLTi-dose randomized control trial in adolescents and young adults with T1D using a full closed loop with two liquid meal challenges showed a similar improvement of 18% TIR in the intervention group with dapagliflozin compared with placebo over 24 h (68% ± 6% vs. 50% ± 13%; P < 0.001).
This improvement was seen also during fasting at night, where AID systems work best (6.2 ± 0.7 mmol/L vs. 7.3 ± 1.7 mmol/L; P = 0.003). 18 As seen in the other SGLTi plus AID trials, daytime postprandial glucose peaks were still observed using full AID setting with and without SGLTi. Of note, in the full closed-loop setting, ketone levels tend to increase with SGLTi before the meal challenges but returned to normal levels within 30 min after the intake of oral carbohydrates and resulting AID.
As a consequence, education for both, people with diabetes and providers, are mandatory. They need to be aware that resolving elevated ketones in people with T1D using SGLTi needs both insulin and glucose. As a prerequisite, a timely detection of elevated ketones is crucial to mitigate the higher risk for diabetic ketoacidosis (DKA) with adjunct therapy with SGLTi. 19 Indeed, there was a case of DKA during an infusion set failure while using empagliflozin in this study and this has also been described during off-label use of SGLTi in AID previously. 20 Treatment with SGLTi may even lead to euglycemic ketoacidosis without hyperglycemia (euDKA) particularly during stress, alcohol consumption, or illness. 21
DKA is potentially life-threatening if not treated adequately and, therefore, remains a challenge globally with numerous emergency room visits and hospitalizations for DKA each year across different health systems and global regions even without the use of SGLTi. 22 Measures of ketone self-monitoring are available and education for taking the appropriate steps for risk mitigation is in place, 18 but it remains doubtful if this would be sufficient to prevent DKA in those people with T1D who choose to use SGLTi.
Although real-world data from Germany/Austria have not found DKA cases in people with T1D and SGLTi use, 23 this study shows that the risk for ketosis and ketoacidosis with SGLTi remains. It is unclear if modifications of the closed-loop algorithms alone would be able to mitigate this risk. A major issue appears to be that few people with diabetes are regularly monitoring their ketones because the current methods of testing—whether they are performed through blood or urine testing—appear to be costly or burdensome. 24
Although measuring the ketone β-hydroxybutyrate in blood by finger pricks may allow detection of euDKA if “for cause self-monitoring” is performed, 25 recent progress developing continuous ketone sensing may be the critical step for timely recognition of impending DKA. 26 Recent studies show that continuous ketone monitoring could help prevent DKA. 27 With continuous monitoring, rising ketone levels can be detected early, as a warning of impending metabolic dysregulation, and inform people with diabetes that MEASURES CAN BE TAKEN TO PREVENT THE ONSET OF DKA.
Adding continuous ketone monitoring to a continuous glucose monitoring system eliminates the need for a separate ketone test and would be an ideal complement to safeguard an AID system with and without adjunct therapy with SGLTi. Recently it has been announced that the development of a new biowearable that will continuously monitor glucose and ketone levels in one sensor has secured breakthrough device designation from the U.S. Food and Drug Administration. 28
Last year the WHO published the new 22nd edition of its Model Lists of Essential Medicines to include insulin analogues and SGLT2 inhibitors. 29 The effects of SGLT2 inhibitors for cardiovascular outcomes have been well recognized in people with and without diabetes, and thus these medications should be available and affordable for all. However, despite SGLTi being classified as “essential drugs” for diabetes by the WHO, these are currently not available for T1D. The FDA's Endocrinologic and Metabolic Drugs Advisory Committee have not approved SGLTi for T1D citing lack of adequate data to support evidence for safety (i.e., DKA). Although a limited approval of two SGLTi for those with T1D and a body mass index >27 kg/m2 was granted in Europe, the commercial decision of pullback of the only available product for T1D from the market was taken by the manufacturer. 30
This unmet need for adjunct therapy to insulin with AID goes well beyond glycemic outcomes. In people with type 2 diabetes, treatment with SGLTi is proven not only beneficial for cardiovascular outcomes and kidney disease 31 but also with benefits for heart failure in those without diabetes. 32 Indeed, improving cardiovascular outcomes appears to be a “class effect” characterizing SGLTi in general. 33 Experts agree that particularly individuals with early onset of T1D have a high excess risk for negative cardiovascular outcomes. 34 It is likely that an additional focus on cardioprotection might be warranted even in those that are achieving glycemic targets with AID.
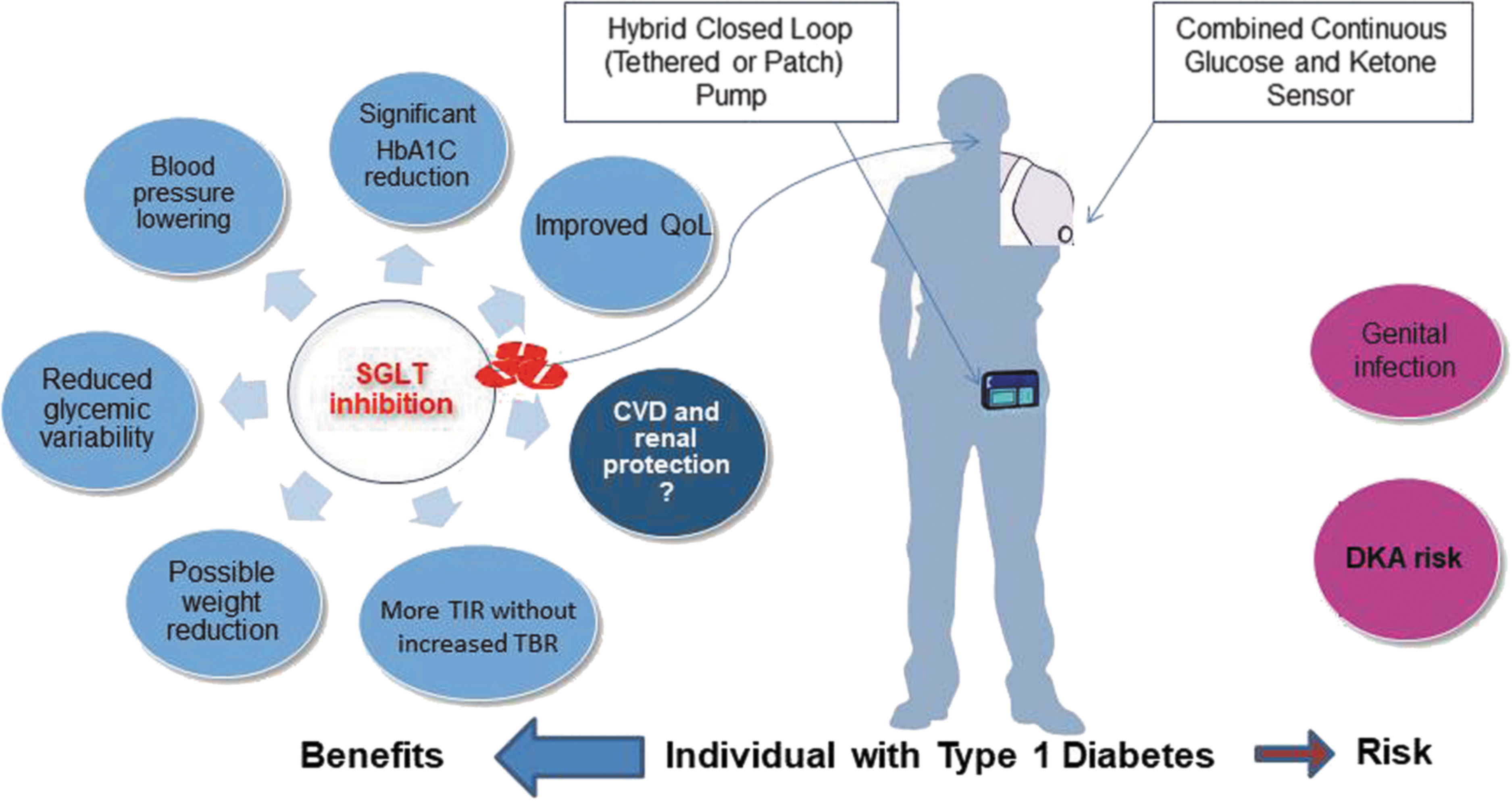
Although the article of Garcia-Tirado et al 11 underlines the glycemic advantages of low-dose SGLTi for glycemic outcomes in T1D on top of those achievable with current commercially available hybrid closed-loop pumps, the long-term cardiovascular benefits may be even far more important for people with T1D (Fig. 1). Better means to detect elevated ketones are on the horizon but studies elucidating the mechanisms underlying the development of DKA during SGLTi in T1D are urgently needed. Hopefully the unmet need of adjunct therapy with an “essential diabetes medicine” for people with T1D will become a safe therapeutic option with and without access to AID in the not too distant future.
Balancing risk and benefit of sodium-glucose cotransporter inhibitors-supported automated insulin delivery-therapy of type 1 diabetes when timely ketone monitoring is in place.
Footnotes
Authors' Contributions
T.B. wrote the first draft of the article; T.D. and T.B. both revised and approved the final version.
Author Disclosure Statement
T.B. reports speaker fees, consulting honoraria or research support from AstraZeneca, Ascensia Dexcom, Medtronic, Novo Nordisk, Roche, Sanofi, and Ypsomed. Since 2021, he is a member of the Expert group for medical devices of the European Commission. T.D. has received speaker's honoraria and research support from and has consulted for Abbott, AstraZeneca, Boehringer, Dexcom, Lilly, Medtronic, Novo Nordisk, Roche, Sanofi, and Ypsomed, and is a shareholder of DreaMed Ltd.
Funding Information
No funding was received for this article.