
Abstract
Objective:
The safety and impact of the advanced hybrid closed-loop (AHCL) system on glycemic outcome in 2- to 6-year-old children with type 1 diabetes and the diabetes distress of caregivers were evaluated.
Research Design and Methods:
This was an open-label prospective study (n = 35) with historical controls matched by treatment unit, diabetes duration, age, gender, and baseline treatment modality. The inclusion criteria were (1) type 1 diabetes diagnosis >6 months, (2) total daily dose of insulin ≥8 U/day, (3) HbA1c <10% (85 mmol/mol), and (4) capability to use insulin pump and continuous glucose monitoring. The MiniMed 780G™ AHCL in SmartGuard™ Mode was used for 12 weeks. Parental diabetes distress was evaluated with a validated Problem Areas In Diabetes—Parent, revised (PAID-PR) survey.
Results:
No events of diabetic ketoacidosis or severe hypoglycemia occurred. Between 0 and 12 weeks, HbA1c (mean change = −2.7 mmol/mol [standard deviation 5.7], P = 0.010), mean sensor glucose value (SG) (−0.8 mmol/L [1.0], P < 0.001), and time above range (TAR) (−8.6% [9.5], P < 0.001) decreased and time in range (TIR) (8.3% [9.3], P < 0.001) increased significantly, whereas no significant change in time below range (TBR) was observed. At the same time, PAID-PR score decreased from 37.5 (18.2) to 27.5 (14.8) (P = 0.006).
Conclusions:
MiniMed 780G™ AHCL is a safe system and 12-week use was associated with improvements in glycemic control in 2- to 6-year-old children with type 1 diabetes. In addition, AHCL is associated with a reduction in parental diabetes distress after 12-week use.
Introduction
Treatment of type 1 diabetes in young children is challenging since they experience often marked day-to-day and within-day variability in glucose levels as well as high variability in insulin requirements compared with older children with type 1 diabetes. 1,2 Characteristically, young children also have an increase in insulin need during the late evening hours, and reduced need of insulin during early morning hours, making insulin adjustment more challenging. 1,3 Glycemic targets are difficult to achieve, even though insulin pump treatment and continuous glucose monitoring (CGM) is nowadays recommended and frequently used in preschool-aged children with diabetes. 4,5 Owing to these special features, the results from studies of diabetes treatment modalities in older age groups may not be completely adapted to young children with diabetes.
The burden of caregivers is overwhelming, and parents often feel they need to be “on guard” continually monitoring symptoms and glucose values of the child. 6,7 The fear of nighttime hypoglycemia is common, and only 32% of young children's hypoglycemia appear to be recognized with self-monitoring blood glucose measurements. 8,9 Reaching glycemic targets already in early childhood is important since the risk of microvascular complications increases with inadequate glycemic control during the first years of diabetes. 10 In addition, a recent 6-year longitudinal study suggested that total brain, gray, and white matter volumes and cognitive scores are affected by hyperglycemia in early-onset type 1 diabetes. 11
The challenging conflict between high demands of good glycemia and parental well-being may be solved by technology. There are results from both observational 12 and randomized 13,14 studies for hybrid closed-loop (HCL) systems, which in adults and in children older than 7 years have been encouraging, suggesting that an algorithm that automatically doses basal insulin based on sensor glucose (SG) levels improves time in range (TIR) (3.9–10 mmol/L/71–180 mg/dL) without increasing or even decreasing the time spent below range (TBR). 12 –15 This result appears to be maintained at a 1-year follow-up. 12,13 Currently, there are two randomized studies on HCL system-use in younger (<7 years) children, and these studies show promising results: TIR increased without increased time below range. 16,17 Furthermore, nonrandomized and observational studies in children, aged <7 years, have shown similar results. 12,18 –21
The use of Minimed 780G™ system, which gives autocorrection boluses in addition to automatic basal doses when sensor glucose levels are predicted to rise, might aid to ease the challenges with daily insulin treatment and to reach glycemic targets in young children with diabetes. In real-life studies, the MiniMed 780G™ AHCL system has assisted adults and children over the age of 7 years in reaching higher TIR without increasing TBR, and the treatment satisfaction has been better than with sensor-augmented pump (SAP) plus predictive low-glucose suspend (PLGS) pump therapy. 22 –24
In a recent retrospective study, glycemic parameters of pediatric users with the 670G™ HCL or 780G™ AHCL systems were compared. In this study, glycemic targets were reached more often in advanced hybrid closed-loop (AHCL) users than in subjects with HCL. 25 To the best of our knowledge, the Minimed 780G™ system has not previously been investigated in the age group of 2- to 6-year-olds with type 1 diabetes.
The aim of this study was to assess the safety and impact of the MiniMed 780G™ AHCL system on glycemic outcome in 2- to 6-year-old children with type 1 diabetes. In addition, we evaluated the perceived burden of the diabetes treatment on families (termed diabetes distress).
Materials and Methods
This was a nonrandomized prospective single-arm clinical trial with retrospective registry controls. The study was conducted at pediatric diabetes outpatient clinics of Helsinki University Hospital (New Children's Hospital, Jorvi Hospital, Lohja Hospital, and Hyvinkää Hospital). The inclusion criteria were (1) age from 2 to 6 years, (2) TDD (total insulin daily dose) ≥8 U, (3) HbA1c <10%/ < 85 mmol/mol, (4) capability to use insulin pump and the CGM, and (5) time from diabetes diagnosis ˃6 months.
The exclusion criteria were (1) hemophilia or any other bleeding disorder and (2) any reason that in the opinion of the investigator would put the participant at risk (e.g., need for an interpreter during the visits). Eligible participants were identified from the Helsinki University Hospital BCB® diabetes registry in alphabetical order (

Flowchart of the study participants.
The protocol also included a retrospective control population (n = 35) that was also derived from the Helsinki University Hospital BCB diabetes registry. These registry controls fulfilled the same inclusion and exclusion criteria and were matched with prospective participants regarding treatment unit, diabetes duration, age, gender, and baseline treatment modality. To receive well age-matched control data, registry control data were derived at two time points in 12-week interval (data mainly from years 2019, 2020, and 2021). The baseline characteristics of the study population and historical controls are shown in Table 1.
Baseline Characteristics of 2- to 6-Year-Old Children with Type 1 Diabetes Who Underwent Treatment with the Minimed 780G™ System and Historical Controls
Mean (SD).
iCGM, intermittent glucose monitoring; MDI, multiple daily injections; rtCGM, real-time continuous glucose monitoring; SD, standard deviation.
The children with type 1 diabetes used an AHCL pump (MiniMed 780G™ system with SmartGuard™ Medtronic, Northridge, CA, USA) during the study period. MiniMed 780G™ is an insulin pump that doses insulin automatically to subjects' subcutaneous tissue every 5 min based on SG values. The SmartGuard™ feature uses meal information, SG readings, and SG target values to control basal insulin delivery. In addition, the system can automatically deliver a correction bolus to correct a high SG reading. The MiniMed 780G™ insulin pump requires a minimum of eight units and a maximum of 250 U/day to operate using the SmartGuard™ feature. 26 The system is currently not indicated for children under the age of 7 years, and the use of the MiniMed 780G™ system in this study was off label.
The families were trained to use the device by Medtronic's local representatives (technical issues), diabetes nurses, and clinicians (dosing and other medical issues). If the family had been on a SAP, PLGS, or HCL treatment previously, training included one 3-h session either remotely (through Microsoft Teams™) or at the outpatient clinic. If the family had no previous experience with pump treatment, they first wore CGM for 2 weeks, and thereafter a 3-day visit to the hospital day ward was arranged to learn the basics of insulin pump treatment. This 3-day stay in the hospital day ward is standard clinical practice at our center for those with no prior pump treatment experience.
CGM parameters and insulin doses were collected from Carelink Clinical™ Therapy management software, where the data from the insulin pump and CGM were downloaded either automatically through MiniMed™ Mobile or by child's caregivers. Clinicians and diabetes nurses monitored the safety of the treatment by frequent contacts with caregivers (pump downloads and phone call or My Chart App in Epic system), first twice a week until 3 weeks and thereafter every 2 weeks until 3 months.
Contacts were more frequent compared with the usual clinical protocol (remote contacts on week 1 and 2 and outpatient visit 1 and 3 months after the AHCL initiation), to confirm the safety of the patients and for quick optimization of pump settings. HbA1c (Afinion2™; Abbott) was measured by a diabetes nurse from the fingertip as a point-of-care test in run-in phase and at the 12-week visit. We used 14 days' data to calculate the glycemic metrics at baseline and at 12 weeks, as recommended at International Consensus on Time in Range. 27
Height and weight were measured in run-in phase and at the 12-week visit. Diabetes distress was evaluated in run-in phase and at 12-week visit by the Problem Areas In Diabetes—Parent, revised (PAID-PR) survey, which is a standardized 18-question questionnaire evaluating different areas (e.g., sleep and worry) of parental diabetes-induced stress. 28 Higher PAID-PR scores (range 0–100) indicate more diabetes distress.
The settings of the SmartGuard™ system were initially chosen cautiously to avoid hypoglycemia: target glucose was set at 6.7 mmol/L and active insulin time at 3.5 h. Carbohydrate ratio for breakfast was counted with the 360-rule (360/TDD = carb ratio) and for other meals using the 400-rule (400/TDD = carb ratio), based on Medtronic R&D simulation data. SmartGuard system settings were changed according to instructions for clinicians (Supplementary Appendix SA1), the clinicians were, however, not forced to follow up the instruction form, thus changes upon clinical decision were allowed.
The primary endpoint was the change in TIR during follow-up compared with the start of the run-in phase and with AHCL start (end of run-in phase). Secondary endpoints were the changes in safety (number of severe hypoglycemia and diabetic ketoacidosis [DKA]), HbA1c, TBR, mean SG, standard deviation (SD), coefficient of variation (CV) of SG, glycemia risk index (GRI), and rate of diabetes distress during follow-up. TIR and TBR in the treatment arm at 3 months were compared with those in the control group. The outcome measures were compared with glycemic variables in manual mode (PLGS) before starting the AHCL.
The study protocol was approved by the Finnish Medicines Agency (FIMEA) and the Ethics Committee of Helsinki University Hospital. A research permit was also obtained from Helsinki University Hospital. The principles of Good Clinical Practice and the Declaration of Helsinki were followed.
Statistical and power analyses
Based on previous studies, we estimated that a significant difference in the increased TIR between the AHCL treatment and the manual mode would be 10% and the SD 13%. Taking these into account and a 90% power to detect a difference between the modalities with a type 1 error rate of 0.05, we calculated that 35 children with type 1 diabetes are needed to complete the protocol. We estimated the dropout rate to be <3%; thus, we recruited 38 participants.
Statistical analyses and data preparation were performed with SPSS® statistic for Windows (version 25; Chicago, IL, USA). The data are presented as mean (SD) unless otherwise mentioned. The changes in the main outcome measures were analyzed with paired samples t-test between 0 (i.e., baseline) and 12 weeks and reported with standardized mean difference (SMD) and t values. SMD (i.e., Cohen's d) indicates the effect size and values 0.2, 0.5, and 0.8 can be considered small, medium, and large effect.
Since this was not a randomized controlled trial, the provided t and P-values should be considered as approximations of the relative sensitivities of response variables. Comparisons between two and three groups were analyzed with independent samples t-test and one-way analysis of variance (ANOVA), respectively. The glycemic data of historical controls were used as illustrative background data, and statistically compared with the data of the study subjects only at the start of study (at 0 week). Correlations between measures of glycemic control were analyzed with Spearman's rank correlation. All P-values were two-sided and the level of statistical significance is set at P ˂ 0.05.
Results
Thirty-five participants were enrolled and completed the study protocol. Of them, 18 (51%) were boys and the mean age of the participants was 4.3 years (Table 1). At baseline, historical control has otherwise similar glycemic parameters than children with type 1 diabetes who initiated AHCL, but TBR was significantly higher (4.6% [3.2] vs. 3.0 [1.9] %, P = 0.016, respectively).
Treatment with the AHCL system resulted in a rapid improvement in major glycemic parameters. Between 0 and 12 weeks, HbA1c (SMD = −0.46, t = −2.7), mean SG value (SMD = −0.77, t = −4.6), and time above range (TAR) (SMD = −0.90, t = −5.4) decreased and TIR (SMD = 0.89, t = 5.3) increased significantly (Fig. 2). At the same time, SG SD decreased significantly (SMD = −0.70, t = −4.1, P = 0.0002). There was no difference in SG CV (SMD = 0.17, t = 0.99, P = 0.33) and TBR between baseline and 12 weeks (SMD = 0.11, t = 0.7, P = 0.51). The changes in glycemic parameters did not differ between children aged 2–4 years and those aged 5–6 years (Supplementary Appendix SA1). Glycemic parameters at all time points are shown in Supplementary Figure S1.
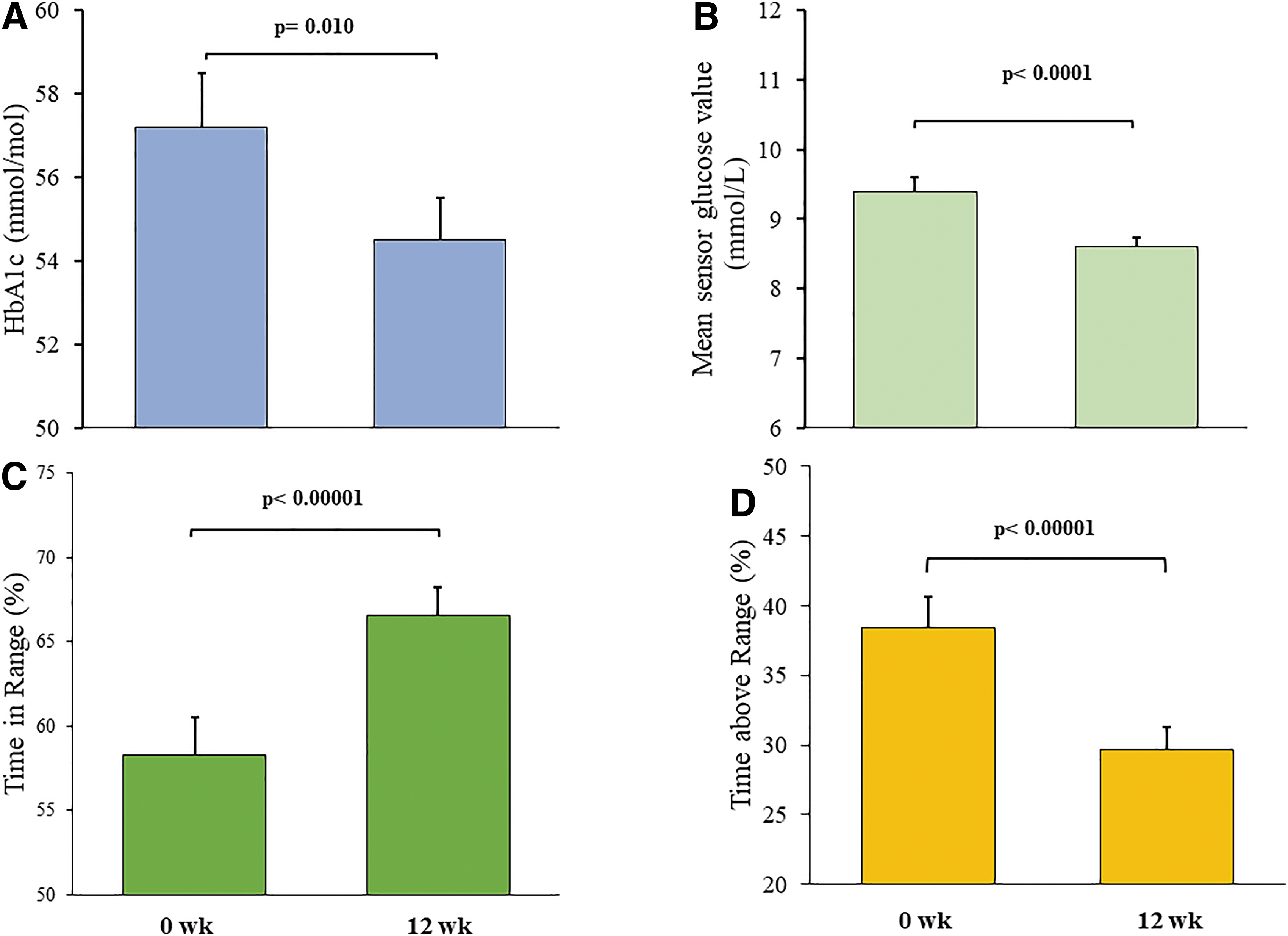
HbA1c
The changes in HbA1c, TIR, TAR, TBR, and SG did not depend on previous treatment modality (F = 0.06–1.6, P = 0.22–0.95) or correlate with age, time from diagnosis, TDD, or insulin dose per weight (P = 0.22–0.80). During the AHCL treatment, GRI values decreased significantly (SMD = 0.93, t = 5.5, P < 0.00001) (Fig. 3). At the 12-week visit, the children with type 1 diabetes remained well in SmartGuard (98.6% [1.9]), and the active insulin time was lower than at the start of the study (3.4 h [0.3] vs. 2.2 h [0.2], P < 0.0001) (Table 2). Glycemic parameters in children with type 1 diabetes who had received training remotely (n = 28) did not differ from those were trained at the outpatient clinic (n = 7) (Supplementary Appendix SA1). No events of DKA or serious hypoglycemia occurred during the study period.
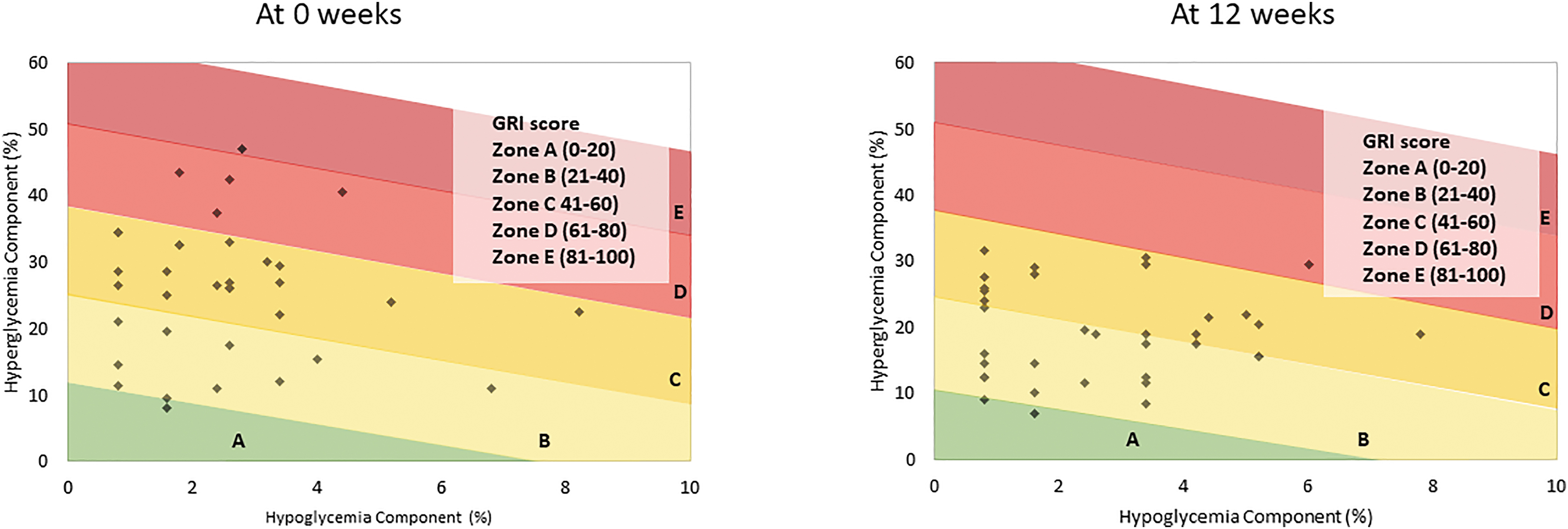
GRI at baseline (0 week) and after 12 weeks of AHCL treatment in 35 children with type 1 diabetes. The reduction in GRI between the time points was statistically significant (P < 0.00001). AHCL, advanced hybrid closed loop; GRI, glycemia risk index. Color graphics are available online.
Glycemic and Insulin Pump Data at the Start of the Study and at 12 Weeks in 2- to 6-Year-Old Children with Type 1 Diabetes Who Were Treated with the MiniMed 780G™ System
Mean (SD). P- and t-values obtained from paired samples t-test.
Next, we evaluated how more aggressive insulin pump setting impacted on glycemic control. At 12 weeks, children with type 1 diabetes with lower target level (5.5 or 6.1 mmol/L) and active insulin time <2.5 h (n = 12) had lower TBR (2.2% [1.6]) compared with children with type 1 diabetes with higher target level (6.7 mmol/L) or active insulin time >2.5 h (3.8% [2.2], P = 0.030) (n = 23). Similarly, higher target level and longer active insulin time correlated positively with TBR (r = 0.35, P = 0.041, r = 0.43, P = 0.009, respectively).
No significant differences in other glycemic markers or TDD were found between the groups. At the same time, children with type 1 diabetes with target level <6.1 mmol/L had similar TDD than those with target level set to 6.7 mmol/L (12.9 IU [3.8] vs. 12.9 IU [4.1], P = 0.99, respectively). Similarly, TDD in children with type 1 diabetes with active insulin time <2.5 h did not differ from those with active insulin time >2.5 h (13.1 IU [4.3] vs. 12.5 IU [2.7], P = 0.66, respectively).
The parental distress questionnaire score decreased from 37.5 (18.3) to 28.6 (14.3) during the 12 weeks of treatment (SMD = 0.52, t = −3.1, P = 0.006). At the start of the study, the PAID-PR score did not correlate with markers of glycemic control, TDD, age, or time from diagnosis (P = 0.22–0.91). Similarly, at 12 weeks, no significant correlations were found between the PAID-PR score and glycemic markers or TDD (P = 0.15–0.80).
Discussion
In this prospective trial, 12-week use of the MiniMed 780G™ system was associated with improvements in glycemic control in 2- to 6-year-old children with type 1 diabetes without increasing the time spent in hypoglycemia. In addition, the use of MiniMed 780G™ appears to be safe in these children since no events of serious hypoglycemia or ketoacidosis were observed during the study. At the same time, the perceived diabetes distress of caregivers was significantly reduced.
Monitoring HbA1c is a traditional way to assess glycemic control and risk of diabetic complications. 29 A good HbA1c in the first 3–15 months after diagnosis is suggested to have an important role in preventing the development of macroalbuminuria and retinopathy in early adulthood. 30 Unfortunately, HbA1c does not measure short-term glycemic variability. 31 In recent years, the impact of TIR (i.e., a marker of short-term glycemic fluctuations) on the risk of micro- and macrovascular complications as well as peripheral neuropathy and cardiac autonomic neuropathy has been reported. 32
To prevent these ominous complications, it is important to achieve satisfying TIR together with acceptable HbA1c already in early childhood. In previous HCL studies in children under the age of 7 years, TIR has increased ∼8%–13% regardless of the baseline TIR. 16 –21 The results of this study confirm the findings of larger multicenter studies, suggesting that HCL systems improve glycemic outcomes also in young children with type 1 diabetes. However, this is the first study to assess this AHCL, Minimed 780G™, treatment in young children.
We found no change in TBR before and after treatment with the MiniMed 780G™ system. This is probably due to efficient pretrial treatment; most of the subjects were on either the PLGS pump or the HCL system and the TBR was already within the acceptable range. Only 3 of our 35-subject population were on MDI treatment modality before study start due to fact that in our hospital majority of small children are put on pump therapy already when diabetes is diagnosed. In a recent study of Ware and coworkers, HbA1c was lower (49 mmol/mol/6.6%) than in our population, but at the same time their TBR was higher (4.9%). 16
Balancing between stringent glycemic control and risk of hypoglycemia is challenging. In our study, GRI reflecting the overall quality of glycemia with a single number declined significantly during the AHCL treatment, thus further supporting the beneficial effect on glycemic control. 33 The improvements in GRI resulted from the decrease in the hyperglycemic component, which is in line with the significant decrease in TAR during treatment.
An increasing body of evidence associates both hyperglycemia and hypoglycemia with adverse findings in brain MRI in fragile young children. 11,34,35 Another less well-known complication of hypoglycemia is dental caries. The prevalence of caries in children with diabetes is very high, up to 67%, and this risk may be reduced not only with good glycemic control but also by avoiding constant snacking to treat or prevent hypoglycemia. 36 AHCL pump therapy maintains high TIR and low CV, and thus may prevent the child from engaging in constant snacking.
Initial pump settings in our study at start of automation were very cautious (active insulin time 3.5 h and SmartGuard™ target level 6.7 mmol/L) to prevent hypoglycemia in our very fragile cohort of children with type 1 diabetes. During the 12-week study period we, however, noticed that shortening the active insulin time to 2.5 h, or even to 2 h, did not increase hypoglycemias but instead had an impact on effect of autocorrection feature, helping our subjects to reach more TIR.
Surprisingly, those with tighter SmartGuard™ target levels also had lower TBR than children with type 1 diabetes with SmartGuard™ target level 6.7 mmol/L, and longer active insulin time correlated positively with TBR. However, the use of tighter SmartGuard™ target levels did not correlate with TDD. This result is in line with recently published real-life study in older children and adults and suggest that also very young children may benefit more aggressive SmartGuard™ target levels and shorter active insulin time to reach glycemic goals without increasing TBR. 22
In families with very young children with type 1 diabetes, the emotional burden caused by the disease, the fear of hypoglycemia and future complications, and the constant surveillance of the child due to difficulties in trusting other adults to take care of their child's diabetes led to increased anxiety and distress of caregivers. 37 Technological advances in diabetes care have been suggested to reduce parental distress.
In a recent randomized controlled study with CamAPS FX HCL-system, caregivers of 30 children were interviewed and all of them reported less diabetes-related work, better sleep, less distress, and more normal life of child with type 1 diabetes. 38 In a short 3-week study, the parents of small children also reported a reduced burden of diabetes management, less time spent managing diabetes, and improved quality of sleep during HCL treatment. 39 Similar results were found in our study, although the follow-up period in both studies were relatively short.
The COVID-19 pandemic forced us to start the MiniMed 780G™ system mainly remotely. However, there was no change in glycemic parameters or safety between children with type 1 diabetes trained remotely and those trained at the outpatient clinic, confirming that virtual pump training may also be used in young children, as seen before in older age groups. 40 Many of the subjects suffered from several viral infections (respiratory infections and gastroenteritis) during the study, which made diabetes care challenging for parents.
Despite this, we found significant improvements in both glycemic endpoints and parental diabetes distress. A strength of the study was that the study population represents a real-world clinical setting. At our clinic, there are no 2- to 6-year-old children with type 1 diabetes with HbA1c >85 mmol/L. Also, every child in this age group is using CGM, and thus the glucose monitoring technology was familiar to the families participating in the study. All participants completed the 12-week study period.
A major limitation of the study was the lack of a prospective control group. However, to provide an overview of typical glycemic control at our clinic in this age group, we generated a historical control group matched to the study population. Co-incidentally HbA1c, mean glucose, and TIR were better (although nonsignificantly) in our historical cohort compared with our study population. Moreover, both the study subjects and historical controls were selected from the patient register in alphabetical order to avoid assessment bias. The use of such a high-quality control group is acceptable for replacement of a control arm in a nonconfirmatory study setting where the study conditions closely mimic those of the controls. 41
In conclusion, the AHCL system MiniMed 780G™ improved glycemic control safely in a 12-week study period in toddlers and preschoolers, simultaneously diminishing parental diabetes distress, offering hope for the treatment of type 1 diabetes in this vulnerable population.
Footnotes
Acknowledgments
The authors thank R.N. Rea Jussila and R.N. Elina Peltonen for gathering the data. The authors thank Medtronic, Inc. for supplying the equipment and technical support.
Authors' Contributions
A.-K.T., M.-A.P., and T.J.V. wrote the article and researched data. T.J.V. made statistical analyses. E.T.H., M.H.H., M.E.H., J.N.J., S.M.K., H.M.L., S.M.L., A.K.W., M.T.H., and P.J.M. researched data and reviewed/edited the article.
Author Disclosure Statement
A.K.T. received lecture and consultation honoraria from Medtronic Diabetes Finland and EMEA and is a member of the Medtronic advisory board in Finland. M.-A.P. received a lecture honorarium from Medtronic Diabetes Finland.
Funding Information
This study was funded by unrestricted grants from the Medtronic External Research Program. Grant number ERP-2020-12544.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Appendix SA1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.