
Abstract
Aim:
To assess relationships between continuous glucose monitoring (CGM) time in range (TIR), 70–180 mg/dL, time below range (TBR), <70 mg/dL, time above range (TAR), >180 mg/dL, and glucose coefficient of variation (CV) in relation to currently recommended clinical CGM targets for older people, which recommend reduced TIR and TBR targets relative to the general type 1 diabetes population.
Methods:
We conducted a post hoc analysis using the JDRF Australia Adult Hybrid Closed Loop trial database examining correlations in 120 adults with type 1 diabetes of 3 weeks masked CGM (Guardian Sensor 3; Medtronic) metrics (n = 61 on multiple daily injections, 59 on non-CGM augmented pumps) using manual insulin dosing at baseline and at 26-weeks, with 50% randomized to automated insulin dosing (AID).
Results:
Correlations between baseline TIR and TAR were strong (r = −0.966; P < 0.0001), weak for TBR (r = 0.363; P < 0.0001), and glucose CV (r = 0.037; P = 0.687) while moderate between CV and TBR (r = 0.726; P < 0.0001). Associations were similar for participants aged >60 years (n = 15) versus younger subjects. Correlations of changes in (Δ) TIR with ΔTAR over 26 weeks were strong (r = −0.945; P < 0.001) and correlations for ΔTBR were weak (r = 0.025; P = 0.802). ΔCV did not significantly correlate with ΔTAR (r = −0.064; P = 0.526) but did with ΔTBR (r = 0.770; P = <0.001).
Conclusions:
Changes in TIR are not associated with changes in TBR. Thus, we recommend that for older AID users whilst TBR targets should be prioritized to reduce hypoglycemia-related risk, TBR should be addressed independently of TIR. Clinical Trial Registratrion number: (ACTRN12617000520336).
Introduction
Older people make up a substantial proportion of those living with type 1 diabetes. In advantaged countries, such as Australia, they outnumber the young several fold. A census dated 30th Sept 2022 found that of 134,735 Australians living with type 1 diabetes, 35% (n = 46,505) were aged 60 years or older compared with 11% aged 20 years or less. 1 Although some older people with type 1 diabetes are very well and live, work, and travel independently, others are at high risk of severe hypoglycemia such as that related to impaired hypoglycemia awareness, impaired cognition, chronic diabetes complications, comorbidities, and frailty. 2
Consequently, hypoglycemia minimization has been a cornerstone of management strategies for older and high-risk people with type 1 diabetes and this has been reflected in management guidelines such as those in the highly cited landmark publication by Battelino et al. 3
Suggested modifications to targets relating to continuous glucose monitoring (CGM) metrics for older and high-risk people with diabetes include a reduction in CGM time below range (TBR) (70 mg/dL) from <4% to <1% and an associated reduction in time in range (TIR) (70–180 mg/dL) from >70% to >50%. 3 The implied premise justifying these modifications to the mainstream recommendations, aimed at addressing the specific needs of the elderly and those at high risk, is that there is an inverse association between TIR and TBR. Based upon these recommendations, it would be reasonable to expect that a proportional reduction of TIR by ∼30% will be associated with a proportional 75% reduction in TBR.
Advances in technology have enabled the development of automated insulin dosing (AID) systems that have helped significantly improve glycemia in people living with type 1 diabetes. 4 Recent publications have demonstrated the feasibility and efficacy of AID systems in people with type 1 diabetes aged ≥60 years 5,6 Glucose-related outcomes in these studies have been assessed in light of the aforementioned CGM targets, and although the TIR target was exceeded by considerable margins, the TBR target of <1% at <70 mg/dL was not achieved by either study. This raises the question as to whether an overemphasis on achieving TIR targets in these studies may have negatively impacted TBR reductions.
We aimed to test this hypothesis by a post hoc assessment of the relationships between glucose metrics, focusing on TIR and TBR, in adults with type 1 diabetes, including in age-based subgroups (>55 and ≤55 years and >60 and ≤60 years) in a cohort of 120 adults with type 1 diabetes who were enrolled in a 26-week AID study.
Research Design and Methods
The study received approval by the Human Research ethics Committee at St Vincent's Hospital Melbourne (HREC 088/16). We conducted a post hoc analysis of masked CGM data from our previously published randomized hybrid closed loop study (ACTRN12617000520336) in 120 Australian adults with type 1 diabetes of whom 64 (53%) were female. Details of the full protocol and main outcomes have been published. 7,8 Participants' ages ranged from 25 to 70 years with 23 (19%) being aged >55 years and 15 (12.5%) were aged >60 years and a mean (SD) diabetes duration of 24 (12) years. Mean (SD) baseline HbA1c levels were 57 (10) mmol/mol or 7.4 (0.9) %.
At baseline, insulin doses were determined manually, with 61 (51%) participants using multiple daily injections (MDIs) and 59 (49%) using insulin pumps without glucose sensor augmentation. Participants were randomized in equal proportions to AID (Medtronic 670G) and usual care for 26 weeks and 110 participants (92%) completed the study.
For this analysis, 3 weeks masked CGM (Guardian Sensor 3; Medtronic) data collected for the study at baseline, pre-randomization, and at study end were used. For those participants randomized to the AID arm, CGM data were collected using the same masked CGM system used to collect pre-randomization and control arm data. The masked CGM was worn in addition to the AID system's real-time CGM. This ensured that data collected was comparable regardless of study stage or randomization status. This sensor configuration has reported performance parameters of MARD (SD) of 9.6 (9.0)% and mean (SD) functional sensor life of 146 (39) h.
CGM metrics and the minimum acceptable data set were defined in accordance with agreed standards mandating at least 10 days of complete data, that is 70% of data from 14 days. 3 Severe hypoglycemia was defined as that requiring third party assistance. 9 The Low Blood Glucose Index (LBGI) was calculated as previously described. 10 Data were analyzed using Stata Software (StataCorp LLC, College Station, TX) and Pearson's correlation coefficients were generated comparing standardized CGM metrics at concurrent time points. Statistical significance was taken at P < 0.05.
Results
Analysis of baseline masked CGM data showed a strong correlation between TIR and time above range (TAR) (>180 mg/dL), whereas correlations between TIR and TBR and time below clinically low range (<54 mg/dL) were weak (Fig. 1a and Supplementary Figure S1a–c). The pattern and strength of these correlations were broadly preserved at 26 weeks independent of study arm (Supplementary Fig. S2). In addition, baseline TIR correlated well with 180–250 mg/dL (r = −0.686; P = <0.001) and >250 mg/dL (r = −0.907; P = <0.001) and less well with 54–70 mg/dL (r = 0.494; P = <0.001) CGM ranges.

Conversely, the associations between glucose coefficient of variation (CV) and TIR and TAR were weak, whereas stronger associations were observed with TBR and with time below clinically low range (Fig. 1b and Supplementary Figure S1d–f). In contrast with TIR, analysis of the 26-week data suggests that AID has a modest impact on correlations between CV with TAR and TBR (Supplementary Fig. S3). In addition, baseline CV correlated moderately with 54–70 mg/dL (r = 0.644; P = <0.001) and less well with 180–250 mg/dL (r = −0.516; P = <0.001) and >250 mg/dL (r = 0.039, P = 0.672) CGM ranges.
Changes in TIR between baseline and 26-weeks remained strongly correlated with changes over the same period in TAR, but not with changes in TBR and time in clinically low range (Fig. 2). Conversely, changes in CV over the 26-week trial did not correlate with TAR but did correlate with TBR and time in clinically low range (Fig. 3).

Correlations comparing

Correlations comparing
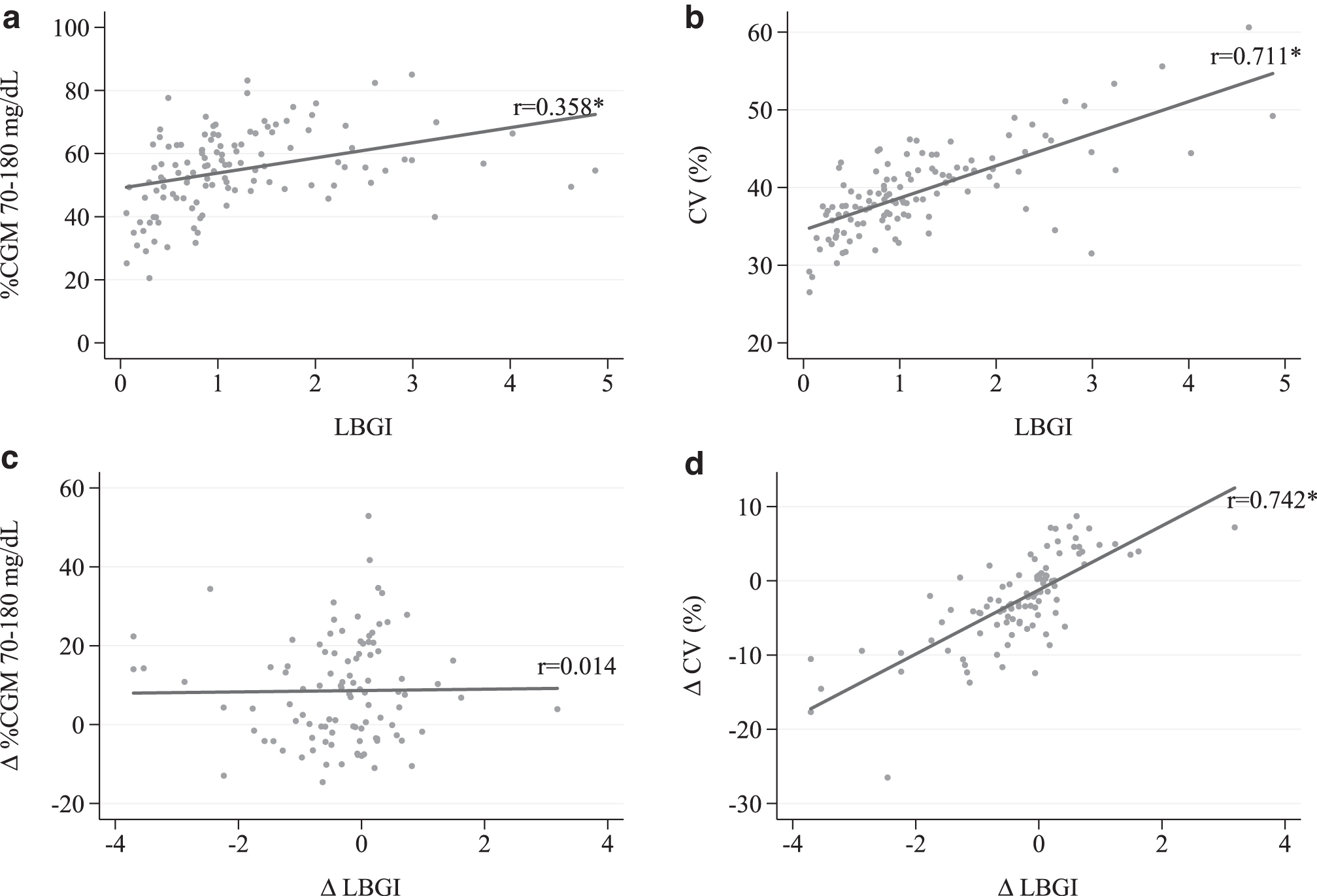
LBGI correlated moderately with CV but poorly with TIR in the analysis of baseline data and changes over 26-weeks in LBGI correlated moderately with changes in CV but not in TIR (Fig. 4).
Correlations comparing
Correlations at baseline were preserved in those aged >55 years (n = 23) and >60 years (n = 15) (Fig. 5).

Correlation map for
There were 17 episodes of severe hypoglycemia in 12 participants over the 26-weeks trial. There were no significant differences in age, TIR, TBR, time in clinically low range, and CV at 26-weeks when comparing individuals who experienced at least one episode of severe hypoglycemia with those who did not (Supplementary Tables S1 and S2).
Discussion
Hypoglycemia minimization remains a cornerstone in the management of people with type 1 diabetes, particularly for those who are elderly or who are frail and at high risk. In recognition of the increased clinical risks associated with hypoglycemia in this cohort, Battelino et al strengthened the TBR target of <4% at 70 mg/dL recommended for the general type 1 diabetes population to <1% for older people and those at high risk. 3 This modification of the TBR target as a strategy would be expected to effectively address the risk of hypoglycemia in this vulnerable group.
In this context, it is notable that, as described in publications by McAuley et al 5 and Boughton et al, 6 the majority of AID-managed adults with type 1 diabetes aged 60 years and over failed to meet the recommended CGM TBR target. It is not our intent to question the appropriateness of the TBR target for older people but rather to challenge any assumptions that TIR is of limited importance in this group and needs to be sacrificed to achieve the TBR target.
In addition to the modification to the TBR targets already described, the published guidelines also place less emphasis on maintaining TIR glucose levels for older and high-risk people, with the TIR target reduced from 70% to 50%, implying that there is a trade-off between TIR and TBR. 3 In contrast to their observations relating to TBR, the TIR outcomes with AID use described by McAuley et al 5 and Boughton et al 6 substantially exceeded the TIR targets for older people, which raises the possibility that a reduction in TBR may be achieved by sacrificing TIR. Our data, in keeping with previous observations, indicate a strong relationship between TIR and TAR. 11,12
However, our observations also indicate that the relationship of TIR with TBR is tenuous. Our longitudinal assessment over 26 weeks revealed that changes in TIR correlated strongly with changes in TAR but poorly with TBR. A change in TIR accounted for 89% of the variability of change in >180 mg/dL range but <0.1% of the variability of change in <70 mg/dL range and 0.4% of the variability of change in <54 mg/dL range. Based upon an analysis of our cohort, a sacrifice of 20% TIR would on an average increase TAR by ∼18% with a negligible (<0.1%) impact on TBR and time below clinically low range.
The dissociation between TIR and TBR is particularly relevant with the advent of AID systems. Trials evaluating this new technology have consistently achieved increases in TIR, usually with reductions in TBR or at least without compromising TBR. 4 –6 Our data suggest that the main outcome of interventions resulting in a reduction in TIR would be more hyperglycemia, with minimal impact, if any, upon hypoglycemia, indicating that TIR targets should be addressed independently of TBR considerations. We recognize that in addition to TBR, other specific measures of hypoglycemia risk exist, such as LBGI, which characterize differences in the glycemic variability of individuals with type 1 diabetes. 10,13,14
These indices may offer alternative metrics to TBR as targets the means by which to assess efficacy of interventions aimed at lowering hypoglycemia risk. However, for the cohort studied herein, the associations and changes in LBGI followed the same pattern as did TBR, with the latter having an advantage in that it is easily calculated and as a concept is readily understood in comparison with LBGI. Other metrics such as glycemic risk index (GRI) may offer a more holistic approach to assessing glucose control with a global estimate of risk. 15 By their nature, assessments such as GRI combine the components of high and low glucose risk. However, the focus of this study lies in investigating the relationship between TIR and TBR in the context of the modified CGM targets for older people with diabetes.
We, therefore, caution against strategies based upon the assumption that to achieve TBR targets, a reduction in TIR is required. Conversely, considerations influencing the TIR targeted in the older person may include those aimed at minimizing the complexity and intrusiveness of insulin regimens and burdensome dietary restrictions that need to be balanced against the knowledge that even acute and subacute elevations in glucose may come at a cost (infections, electrolyte imbalance, dehydration, sarcopenia, falls, cognition, and incontinence) as well as their well-recognized impact upon the development and progression of chronic diabetes complications. 16
We also suggest that TBR targets aimed at ensuring patient safety should be addressed independently with strategies specifically aimed at reducing hypoglycemia. These may entail those aimed at reducing glucose variability and could include interventions facilitating optimal timing and dose of insulin bolus administration for meals or high glucose corrections and to reduce exercise-related glucose extremes. In contrast with TIR, in our trial, changes in CV over 26 weeks accounted for 59% and 41% of the variation in CGM time <70 and <54 mg/dL, respectively, and <0.5% of the variability in TIR (70–180 mg/dL).
The correlation of CV with hypoglycemia CGM metrics is well known and, therefore, an expected finding. Rodbard has previously noted that %TBR is strongly dependent on the glucose CV, with minimal risk of hypoglycemia when the glucose CV is <20%. 13 Although there were insufficient data for us to confidently determine a definitive CV cutoff for a TBR of <1%, our data do suggest that this target could be realistically achieved with CVs substantially higher than 20%. However, we emphasize that TBR at present is the most appropriate clinical metric as a target for minimizing hypoglycemia risk with reductions in glycemic variability reflected by glucose CV as a means by which to achieve this end.
Our observations and conclusions are in keeping with those by Montaser et al 14 who recently described two blocks of CGM metrics, the first related to mean glucose and hyperglycemia and the second to glycemic variability and hypoglycemia, each of which had high internal correlations, but insignificant between-group correlations with the former relating to efficacy and the latter to safety. TIR clustered with hyperglycemia and mean glucose, whereas TBR was associated with hypoglycemia. Our own analyses contextualize these observations within a clinical framework.
The strengths of this study include the quality of the trial data set utilized for the analysis, providing both cross-sectional and longitudinal data points in a moderate-sized cohort followed for 6-months in a consistent standardized format. That participants were not regular CGM users pretrial and half of the participants were using MDI pretrial before being randomized to AID or standard care is a study strength. International standards were employed to determine and ensure the quality of the masked CGM traces. 3 Access to the baseline CGM data could not have influenced behavior.
Data from older and younger adults with type 1 diabetes were available, enabling direct comparisons. Limitations include the potential for selection bias, as with any trial, that all sites were in a single country (Australia), the moderate study size, and small number of participants aged >60 years.
Also, the original study inclusion criteria did not specifically include (nor exclude) older adults, but those who were prepared to consider a hybrid closed loop system. Furthermore, there was a clinically meaningful, but not statistically significant difference in time spent < 70mg/dL for trial participants who did vs. did not experience a severe hypoglycemic event. However, the number of events was small with insufficient statistical power for the comparison in question and studies with larger numbers are required.
Overall, our observations are congruent with data reported from other advantaged countries. 11 –14 In addition, our analyses did not suggest that the pattern in relationships between CGM metrics varied with increasing age. Finally, interrogation of larger global databases, including “real-world” “free-living” people with type 1 diabetes, is needed to confirm our observations and to provide a definitive evaluation of glucose CV cutoffs corresponding to TBR targets and the impact of AID upon these CGM metrics.
In conclusion, as those living with type 1 diabetes age, health care professionals will increasingly be faced with the challenges associated with glycemic control in older high-risk people living with this currently incurable disorder. With the recent advent of AID, increasingly, we are observing outcomes in the general type 1 diabetes population where significant TIR increments can be achieved without compromising TBR, and this also applies to older people living with type 1 diabetes. 4 –6 We suggest that hypoglycemia avoidance and TIR targets should not be linked when considering therapeutic interventions, and in particular the former should be addressed in its own right and prioritized in those who are older and at high risk.
Footnotes
Acknowledgments
Authors thank participants and trial site staff for their participation, NHMRC Clinical Trial Centre (NHMRC CTC) Staff for trial co-ordinations, and NHMRC CTC biostatistician Adrienne Kirby for assistance with data management.
Authors' Contributions
D.N.O., O.C., and R.A.V. conceived the analysis. S.V. performed the analysis. D.N.O., A.J.J., S.V., R.A.V., and O.C. wrote the article. The Australian JDRF Closed-Loop Research Group designed and conducted the original trial.
Statement of Guarantor
D.N.O. is the guarantor of this study and, as such, had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Author Disclosure Statement
D.N.O. has served on advisory boards for Abbott Laboratories, Medtronic, Merck Sharp & Dohme, Novo Nordisk, Roche, and Sanofi; received research support from Medtronic, Novo Nordisk, Roche, Eli Lilly and Company, and Sanofi; and received travel support from Novo Nordisk and Merck Sharp & Dohme. O.C. serves as the medical affairs director—Medtronic Diabetes EMEA. S.V. has no conflicts to declare. R.A.V. serves as chief medical officer, Global Medical and Clinical Affairs Medtronic-Diabetes. A.J.J. has received research support from Medtronic, Sanofi, Abbott Laboratories, and Mylan; and has served on advisory boards for Medtronic, Sanofi, Abbott Diabetes Care, and Insulet.
Funding Information
The original trial was funded by JDRF Australian Type 1 Diabetes Clinical Research Network (3-SRA-2016-351-M-B), a special initiative of the Australian Research Council, and the National Health and Medical Research Council of Australia (APP1099379). In-kind support was provided by Medtronic (HCL systems, masked CGM devices, and technical expertise with device issues) and Roche Diabetes Care (blood glucose meters for participants using MDI).
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Table S1
Supplementary Table S2
Appendix
The Australian JDRF Closed-Loop Research Group members have had input into the study and are named as follows:
Adult Clinical Sites: David N. O'Neal (CI), Sybil A McAuley, Melissa H. Lee, Barbora Paldus, Catriona M. Sims, Richard J. MacIsaac, Glenn M. Ward (St Vincent's Hospital Melbourne); Peter G. Colman (Royal Melbourne Hospital); Neale D. Cohen (Baker Heart and Diabetes Institute); Leon A. Bach, Kavita Kumareswaran (The Alfred); Stephen N. Stranks, Morton G. Burt (Flinders Medical Centre); D. Jane Holmes-Walker (Westmead Hospital); Roland W. McCallum (Royal Hobart Hospital); Joey Kaye (Sir Charles Gairdner Hospital).
Psychological and Cognitive Group: Jane Speight, Christel Hendrieckx, Jennifer Halliday, Sienna Russell-Green (Australian Centre for Behavioural Research in Diabetes: Diabetes Victoria and Deakin University); Steven Trawley (Cairnmillar Institute).
Data and Biobanking Coordination: Alicia J. Jenkins, Andrzej Januszewski, Anthony C. Keech (University of Sydney).
Statistical Analyses: Sara Vogrin, Vijaya Sundararajan (University of Melbourne); Hanafi Mohammed Husin (Australian Centre for Behavioural Research in Diabetes: Diabetes Victoria and Deakin University).
Health Economics: Philip M. Clarke (University of Melbourne).
Paediatric Study Group: Timothy W. Jones, Elizabeth A. Davis, Martin I. de Bock, Mary B. Abraham (Perth Children's Hospital and Telethon Kids Institute); Geoff R Ambler (The Children's Hospital at Westmead); Fergus J. Cameron (Royal Children's Hospital Melbourne); Jan M. Fairchild (Women's and Children's Hospital, Adelaide); Bruce R. King (John Hunter Children's Hospital).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.