
Abstract
Objective:
Nationwide reimbursement of intermittently scanned continuous glucose monitoring (isCGM) was introduced in Belgium (2016). This real-world observational study investigates the impact of isCGM over 24 months on adults with type 1 diabetes with impaired or normal awareness of hypoglycemia (IAH or NAH).
Methods:
We included 1905 people who started first-generation 14-day FreeStyle Libre (without alerts). Sixteen percent had IAH. Primary endpoint was evolution of quality of life (QOL); secondary endpoints were evolution of severe hypoglycemia, work absenteeism, glycated hemoglobin (HbA1c), and sensor-measured outcomes.
Results:
At baseline, people with IAH (n = 308) had significantly worse QOL than people with NAH (n = 1594). Only people with IAH improved on the hypoglycemia fear survey-worry subscale after 24 months (22.8 [95% confidence interval: 21.4–24.2] at baseline; 20.6 [19.0–22.1] at 24 months, P = 0.002). For both groups, Diabetes Treatment Satisfaction Scale improved over 24 months (IAH: +3.1 [2.1–4.1], P < 0.001; NAH: +2.3 [1.9–2.7], P < 0.001), whereas general QOL, diabetes distress, and HbA1c remained stable. People with IAH showed the strongest decline in work absenteeism and severe hypoglycemia (36.4% having an event 6 months before isCGM initiation; 16.0% having an event during last 6 months of follow-up, P < 0.001), with similar observations for hypoglycemia hospitalization and hypoglycemia coma. Over 24 months, people with IAH spent more time in hypoglycemia, but less time in hyperglycemia than people with NAH.
Conclusion:
These data show sustained improvement of severe hypoglycemia, work absenteeism, and hypoglycemia fear after isCGM reimbursement, mostly driven by people with IAH. Together with improved treatment satisfaction, irrespective of hypoglycemia awareness level, isCGM without alerts is a valuable tool under long-term real-world conditions.
Clinical Trial Registration number: NCT02898714.
Introduction
Close self-monitoring of blood glucose is essential for people with type 1 diabetes (T1D) to optimize insulin therapy and glycemic control, which is needed to prevent acute and chronic diabetes complications. To date, glucose sensor-based technologies are probably the most insightful technology to aid self-management of glycemic control.
Two different types of continuous glucose monitoring (CGM) systems can be discerned based on the level of user interaction to obtain glucose readings: intermittently scanned CGM (isCGM), which allows glucose values to be checked on demand by scanning the sensor-transmitter with a receiver or smartphone; and real-time CGM (rtCGM), which has a transmitter that automatically sends a new glucose reading to a receiver, smartphone, or smartwatch every 1–5 min. Unlike first-generation isCGM, next-generation isCGM and rtCGM can forewarn for (predicted) high and low blood glucose levels.
rtCGM and isCGM are increasingly being used and recommended in the management of T1D. 1 Belgium provides nationwide full reimbursement for isCGM since 2016, and for selected rtCGM devices since 2018 for people with T1D. At present, 81% of Belgian adults with T1D use CGM, with isCGM being the predominantly used device (68% of total population). 2
isCGM has been shown to improve glucose control, quality of life (QOL), and severe hypoglycemia, both in randomized controlled trials (RCTs) and in real-world studies. 3 –8 However, these reports are mostly of short duration (<12 months), thus making it less clear how much of the observed effects can be sustained for a longer period of time. Furthermore, real-world evidence of isCGM is often restricted to participants who fall within strict reimbursement criteria imposed by the payers. Long-term follow-up of unrestricted isCGM use has not been reported before, which hampers generalizability of study outcomes.
The use of isCGM in people with impaired awareness of hypoglycemia (IAH) is not well described. Only the study by Reddy et al 9 investigated the effect of rtCGM versus isCGM on people with IAH or recent severe hypoglycemia in an 8-week RCT. At study end, rtCGM proved to be more effective than isCGM in improving time in range (TIR; sensor-measured glucose 70–180 mg/dL [3.9–10.0 mmol/L]), time in hypoglycemia, and hypoglycemia fear. Nonetheless, people with IAH on isCGM showed improved within-group changes in time spent in hyperglycemia. However, there are no data looking at the long-term real-world impact of isCGM in people with IAH.
We previously reported the 12-month findings from the FUTURE study 3 in which we followed 1913 adults with T1D who started first-generation isCGM after full reimbursement became available in Belgium. These people showed an improvement in treatment satisfaction and lower incidence of severe hypoglycemia with stable glycated hemoglobin (HbA1c) and QOL. Our aim in the current analysis was to determine whether the observed benefits could be sustained up to 24 months, specifically looking at people with IAH and normal awareness of hypoglycemia (NAH).
Methods
Study design and participants
This was a multicenter prospective observational cohort study to evaluate the real-life impact of isCGM (first version of the 14-day wear FreeStyle Libre flash glucose monitoring system [Abbott Diabetes Care, Witney, United Kingdom]) in adults with T1D who were recruited between July 2016 and July 2018 at University Hospitals Leuven, University Hospital Antwerp, and OLV Hospital Aalst in Belgium. The results from the full 24 months of the study are reported here, consisting of the first 12-month period from which the results have been published (together with details about device and diabetes management), 3 followed by an additional 12-month extension phase. The study was conducted from July 2016 to July 2020. Eight of the original 1913 participants were re-identified as having type 2 diabetes or excluded because of T1D diagnosis within 3 months of starting isCGM, which brings the total study population for analysis at 1905 adults with T1D (Supplementary Table S1).
The study complied with the Declaration of Helsinki and the International Conference on Harmonization/Good Clinical Practice Guidelines and was approved by the institutional review boards and independent ethics committees of the three participating centers. All participants provided informed consent before entering the study. The study is registered with ClinicalTrials.gov.
Outcomes
Primary endpoint was evolution over time of QOL between baseline and 24 months after start of isCGM. Secondary outcome measures were change in acute diabetes complications (hypoglycemia and/or ketoacidosis/hyperglycemia), work absenteeism, HbA1c, time in ranges, mean glucose concentration, and glycemic variability. Exploratory endpoints included change in weight, BMI, and prescribed insulin doses. Additional post hoc analyses evaluated how many people were able to achieve clinical and sensor-related consensus targets 10 and clinical composite endpoints. 11
Data collection
Details about data collection can be found here, 3 in short: Prespecified clinical data were collected from a period of 12 months before until 24 months after start of isCGM from electronic medical records. Upon isCGM initiation, people were identified as having IAH or NAH based on a review of the electronic medical records and entered in an Excel file using a dropdown list by the treating diabetes team.
Different questionnaires (Short Form 36 [SF-36], 12 Problem Areas in Diabetes—Short Form [PAID-SF], 13 Hypoglycemia Fear Survey [HFS]—worry, 14 Diabetes Treatment Satisfaction Questionnaire [DTSQ]—status and change, 15,16 questions about diabetes-related events) were presented to participants at baseline, 6, 12, and 24 months. Supplement 1 gives a more detailed explanation about the questionnaires. Patient-reported medical interventions, emergency room admissions, and hospitalizations for (symptoms of) acute diabetes complications (hypoglycemia/ketoacidosis/ketosis/hyperglycemia) were validated using hospital records. Hospitalizations for ketoacidosis at diagnosis of T1D were excluded.
Sensor glucose data were extracted for the whole day. For the analyses, following time points were used: 2 weeks (week 0 to 2), 6 months (month 5 to 6), 12 months (month 11 to 12), and 24 months (month 23 to 24).
Statistical analysis
All analyses were performed separately for people with IAH and NAH. The number of people in these subgroups is given in Supplementary Table S2.
We used a linear-mixed model to evaluate SF-36, PAID-SF, HFS-worry, DTSQ status, HbA1c, percentage of time spent in various glucose ranges, mean glucose concentration, standard deviation (SD), coefficient of variation (CV), weight, BMI, and insulin doses with a random effect of center to handle correlation between participants of the same center and an unstructured covariance matrix for four repeated measurements within the same participant. By using a linear-mixed model, cases with missing data still contributed to the analyses (Supplementary Table S3 for number of missing cases per outcome measure). This means that bias in the estimates owing to dropouts or missed appointments with the diabetes team can be reduced to a minimum.
Scores on the DTSQ change questionnaire were compared with zero with a one-sample t-test.
To facilitate interpretation, Cohen's d effect sizes were calculated for the QOL scores.
McNemar's test was used to evaluate changes in number of participants with hospitalizations, work absenteeism, needing help from third parties owing to hypoglycemia, and having hypoglycemic comas. Whereas with the Wilcoxon signed-rank test, differences in number of events and number of days of hospitalizations and work absenteeism, number of times help from third parties was needed, and number of hypoglycemic comas were assessed.
A logistic regression model with generalized estimating equations was used to evaluate the evolution of proportion of participants who reached target HbA1c (<7%; <53 mmol/mol), sensor-related consensus targets, and composite endpoint targets. 10,11
Differences between people with IAH and NAH at different time points were compared with the Mann–Whitney U-test, analysis of covariance with correction for age or diabetes duration, or with the chi-square test.
A Bonferroni–Holm correction was considered for results from all 18 scales referring to the primary outcomes (8 subscales of SF-36, 2 summary scales of SF-36, PAID-SF, HFS-worry, 3 subscales of DTSQ status, and 3 subscales of DTSQ change). No adjustment was made for multiple testing of secondary endpoints.
Statistical analyses were performed with SPSS software for Windows (IBM SPSS Statistics version 28; Armonk, NY). Data are given as mean with SD or least-squares mean with 95% confidence interval (CI), unless otherwise stated.
Results
Person characteristics and isCGM use
Baseline characteristics of the 1905 participants, grouped by level of hypoglycemia awareness are given in Table 1. In both groups, >50% were men and used multiple daily injections. People with IAH were on average older, had a longer duration of T1D, and had a lower mean baseline HbA1c.
Baseline Characteristics
Data are given as mean (SD) or n (%).
As identified from the electronic medical records.
P-value for the difference between groups.
Defined as graduated from university or college.
Numbers represent period of 12 months before start.
Hospitalizations for ketoacidosis at diagnosis of type 1 diabetes were excluded.
Other diagnoses besides confirmed ketoacidosis can include ketosis without acidosis and sustained hyperglycemia.
Numbers represent period of 6 months before start.
DTSQ, Diabetes Treatment Satisfaction Questionnaire; HbA1c, glycated hemoglobin; HFS, Hypoglycemia Fear Survey; IAH, impaired awareness of hypoglycemia; NAH, normal awareness of hypoglycemia; PAID-SF, Problem Areas in Diabetes-Short Form; SD, standard deviation; SF-36, Short Form 36.
Regarding QOL, people with IAH had worse scores on the SF-36, PAID-SF, HFS-worry, and DTSQ status treatment satisfaction survey in comparison with people with NAH (Tables 1 and 2). After correction for age/diabetes duration, baseline scores still indicated worse QOL for people with IAH as compared with people with NAH for the following QOL scores: SF-36 Role Physical (P = 0.006 after correction for age/P = 0.011 after correction for diabetes duration), SF-36 Social Functioning (P = 0.001/P = 0.004), SF-36 Physical Component Summary (P = 0.018/P = 0.040), PAID-SF (P = 0.001/P = 0.003), HFS-worry (P < 0.001/P < 0.001), and DTSQ status treatment satisfaction (P < 0.001/P < 0.001). A higher perceived frequency of hypoglycemia was reported by people with IAH on the DTSQ status questionnaire (Table 1), which remained valid after correction for age and diabetes duration.
Quality of Life Scores Before and After Initiation of Intermittently Scanned Continuous Glucose Monitoring for People with Impaired and People with Normal Awareness of Hypoglycemia
Data are given as least-squares mean (95% CI).
P-value for the change versus baseline, except for DTSQ change where P-value is for the change versus zero.
Significant after Bonferroni–Holm correction.
CI, confidence interval; NA, not applicable.
A significantly higher proportion of people with IAH had at least one severe hypoglycemia event as well as at least half a day of absence from work in the period before start of isCGM (Table 1).
People with IAH scanned the isCGM sensor more; however, differences were small (average scan frequency across 24 months: 9.9 ± 5.0 times/day for IAH vs. 9.4 ± 5.9 times/day for NAH; P = 0.004).
Of 1905 people who started isCGM, 96% (n = 1825/1905), 91% (n = 1735/1905), and 82% (n = 1568/1905) had >6, 12, and 24 months of follow-up, respectively (Supplementary Fig. S1). In total, 337 people (18%) ended the study prematurely. There were three reasons to stop: stopped using isCGM (n = 237/337, 70% of people who stopped), lost to follow-up (n = 77/337, 23% of people who stopped), or deceased during the study period (n = 23/337, 7% of people who stopped). Both participants with IAH and NAH stopped using isCGM mainly because of switch to rtCGM (n = 17/30, 57% of people with IAH who stopped vs. n = 71/207, 34% of people with NAH who stopped) and skin reactions (n = 5/30, 17% of people with IAH who stopped vs. n = 42/207, 20% of people with NAH who stopped).
Quality of life
For SF-36 subscore scales, people with IAH remained stable in contrast to people with NAH who showed slight reductions after 24 months (Table 2). However, within-group differences were not clinically significant after 24 months (Supplementary Table S4). In addition, only people with IAH showed a significant improvement on the HFS-worry scale after 24 months (IAH: 22.8 points [95% CI: 21.4–24.2] at baseline vs. 20.6 points [95% CI: 19.0–22.1] at 24 months, P = 0.002; NAH: 17.2 points [95% CI: 16.7–17.8] at baseline vs. 17.2 points [95% CI: 16.5–17.8] at 24 months, P = 0.799; Table 2).
The DTSQ status satisfaction scale improved from baseline to 6 months and remained high throughout the whole 24 months for both groups (P < 0.001 vs. baseline for both groups; Table 2).
The mean perceived frequency of hypoglycemia of the DTSQ status scale was higher for the IAH group at baseline (3.5 points [95% CI: 3.3–3.7] for IAH vs. 2.9 points [95% CI: 2.7–3.1] for NAH, P < 0.001) and did not change significantly, whereas the score for people with NAH increased up to 24 months (3.3 points [95% CI: 3.1–3.5], P < 0.001), indicating a rise in perceived hypoglycemia (Table 2).
Based on treatment effect sizes, the use of isCGM had a medium to large effect (Cohen's d > 0.5) on treatment satisfaction and only a small effect (Cohen's d < 0.2) on the other QOL scores in both groups (Supplementary Table S5).
Acute diabetes complications and work absenteeism
More people with IAH had hypoglycemia-related acute complications than people with NAH before start of isCGM and the former group showed the largest reduction of these events over 24 months (Fig. 1). A decline in hypoglycemia-related hospitalizations was seen only in people with IAH. Nevertheless, both people with IAH and NAH showed a decrease in help needed from third parties because of hypoglycemia and hypoglycemic comas. The same trend was observed for diabetes-related work absenteeism (Supplementary Table S6).

Hypoglycemia-related acute complications for people with IAH and people with NAH before and after isCGM initiation. Data points represent percentage of people with
Sensor-measured glucose outcomes
People with IAH spent more time (in %) in hypoglycemia than people with NAH in the first 2 weeks of isCGM use (<70 mg/dL [3.9 mmol/L]: 10.8% [95% CI: 9.2–12.4] for IAH vs. 8.6% [95% CI: 7.3–10.0] for NAH, P < 0.001; <54 mg/dL [3.0 mmol/L]: 5.1% [95% CI: 3.8–6.5] for IAH vs. 3.6% [95% CI: 2.8–4.4] for NAH, P < 0.001). Over 24 months, both groups were able to reduce time spent in hypoglycemia, which resulted in a significant between-group difference at 24 months (<70 mg/dL [3.9 mmol/L]: Δ2.6%, P < 0.001; <54 mg/dL [3.0 mmol/L]: Δ1.6%, P < 0.001; Fig. 2A, B and Supplementary Table S7).
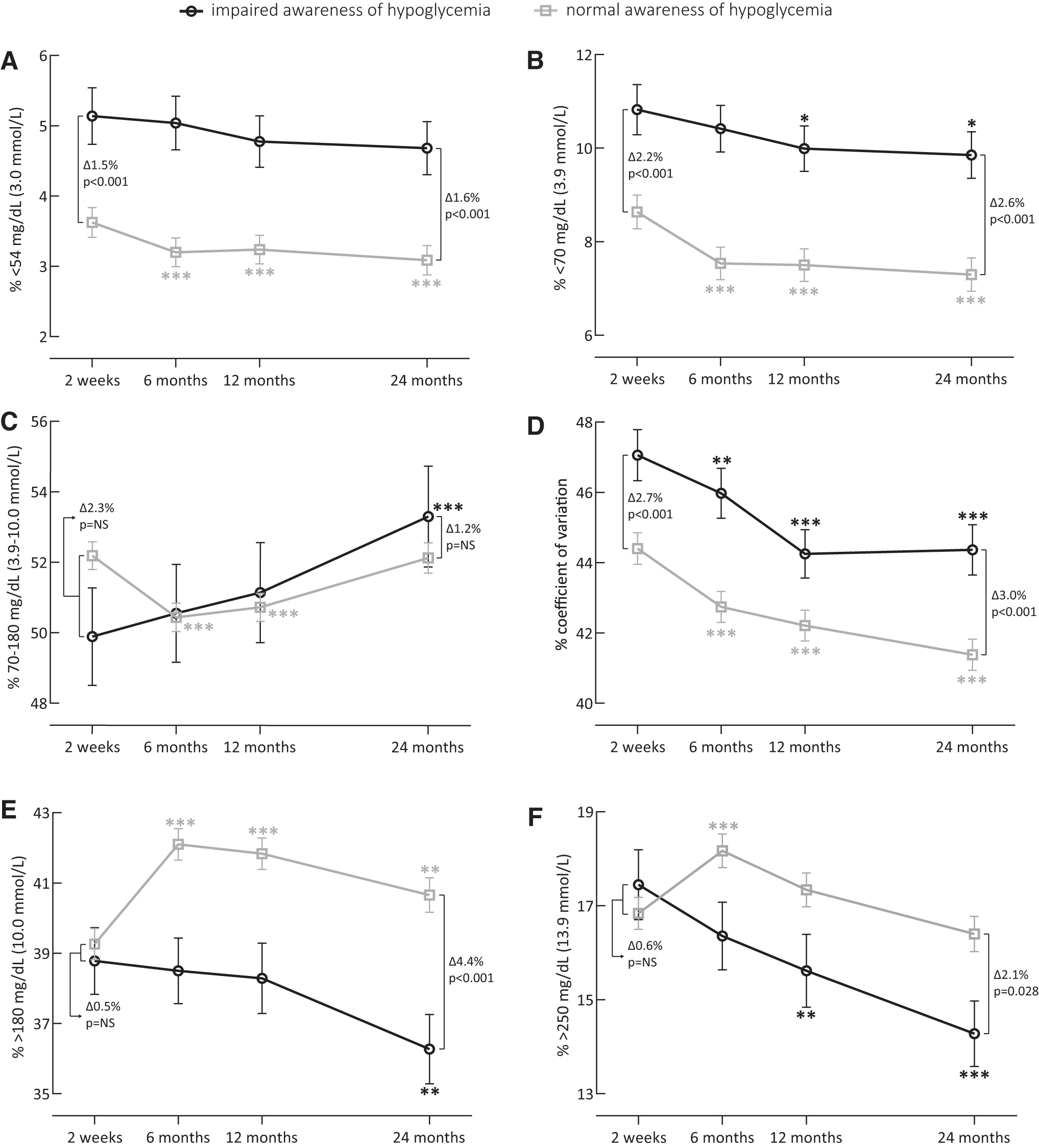
Sensor-measured glucose outcomes for people with IAH and people with NAH during isCGM use. Data points represent least-squares mean (standard error) of
After 24 months, only people with IAH showed an improvement in TIR (Fig. 2C, and Supplementary Table S7) and time in both levels of hyperglycemia as compared with the first 2 weeks of isCGM use, so that people with IAH spent less time in hyperglycemia than people with NAH at 24 months (>180 mg/dL [10.0 mmol/L]: Δ4.4%, P < 0.001; >250 mg/dL [13.9 mmol/L]: Δ2.1%, P = 0.028; Fig. 2E, F and Supplementary Table S7). Both groups showed a decrease in glycemic variability as measured by CV (Fig. 2D and Supplementary Table S7) while using isCGM (P < 0.001 vs. baseline for both groups).
Based on the analysis of the glucose consensus targets (Supplementary Table S8), both groups benefited from isCGM with increased proportions of people achieving the predefined targets of <25% above 180 mg/dL (10.0 mmol/L) (IAH: 21.5% of people at 2 weeks vs. 25.2% of people at 24 months, P = 0.804 for the 24-month evolution; NAH: 18.0% of people at 2 weeks vs. 18.9% of people at 24 months, P = 0.024 for the 24-month evolution) and <5% above 250 mg/dL (13.9 mmol/L) (IAH: 13.3% of people at 2 weeks vs. 25.4% of people at 24 months, P = 0.001 for the 24-month evolution; NAH: 15.8% of people at 2 weeks vs. 19.6% of people at 24 months, P < 0.001 for the 24-month evolution) throughout 24 months of follow-up.
For the other consensus targets, the proportion of people with IAH who could achieve these targets did not change statistically significantly over 24 months. More people in the NAH group were able to achieve the targets of CV ≤36% and <4% below 70 mg/dL (3.9 mmol/L) after 24 months (P < 0.001 for both outcomes); however, less people with NAH could meet the targets of HbA1c <7% (53 mmol/mol) (19.5% of people at baseline vs. 17.1% of people at 24 months, P < 0.001) and the consensus targets in combination with HbA1c <7% (53 mmol/mol).
This resulted in a significant difference between people with IAH and NAH for the following targets after 24 months: HbA1c (P < 0.001; in favor of people with IAH), targets of hypoglycemia (<4% below 70 mg/dL [3.9 mmol/L], P < 0.001; <1% below 54 mg/dL [3.0 mmol/L], P < 0.001; in favor of people with NAH), and target of time above range (<25% above 180 mg/dL [10.0 mmol/L], P = 0.046; in favor of people with IAH). There were no between-group differences for the other consensus targets at 24 months (Supplementary Table S8).
Metabolic control and daily insulin dose
People with IAH as well as people with NAH had a stable HbA1c profile during 24-month isCGM use (Supplementary Fig. S2). Both at baseline (7.9% [62 mmol/mol] vs. 7.7% [61 mmol/mol], P = 0.002) and after 24 months (7.8% [62 mmol/mol] vs. 7.7% [61 mmol/mol], P = 0.007), a significant difference in HbA1c was observed between the two groups, where people with IAH had the lowest HbA1c levels.
A slight numeric increase in body weight from baseline to 24 months was found in both groups (75.2 kg [95% CI: 73.6–76.8] to 75.6 kg [95% CI: 74.0–77.2], P = 0.197 for IAH; 76.4 kg [95% CI: 72.5–80.2] to 77.2 kg [95% CI: 73.8–80.7], P < 0.001 for NAH), without statistically significant between-group differences. The same was observed for BMI (data not shown).
The total (basal+mealtime) prescribed daily insulin dose throughout the 24-month follow-up period slightly decreased for both groups (IAH: baseline, 0.62 U/kg [47.5 U/day] and 24 months, 0.59 U/kg [45.1 U/day]; NAH: baseline, 0.64 U/kg [49.5 U/day] and 24 months, 0.62 U/kg [48.5 U/day]). A higher decrease in basal insulin dose (−1.4 U/day [95% CI: −2.1 to −0.6]) was observed for people with IAH as compared with mealtime insulin dose (−1.0 U/day [95% CI: −2.2 to 0.1]), whereas the opposite could be observed for people with NAH (−0.2 U/day [95% CI: −0.6 to 0.2] for basal dose; −0.6 U/day [95% CI: −0.8 to −0.1] for mealtime dose) (Supplementary Table S9). The ratio of the daily basal insulin dose to the total daily insulin dose remained stable and was comparable between groups (0.45 for IAH and 0.46 for NAH).
Discussion
Results from the 24-month observational FUTURE study provide more insight into the real-life effects of isCGM in a large and heterogeneous population of people living with T1D. To our knowledge, this is one of the largest and longest prospective real-world cohort studies to assess patient-reported outcome measures, clinical and sensor data after nationwide fully reimbursed introduction of isCGM. We showed that isCGM use by adults with T1D treated in three specialized centers was associated with 24 months of sustained improvements in treatment satisfaction, less work absenteeism, and less acute hypoglycemic events, mainly in people with IAH.
We are the first to show the long-term real-world impact of isCGM in people with IAH. Two other real-world studies, one from the United Kingdom 17 and one from Scotland, 18 only report the proportion of people with IAH before and after isCGM initiation, but other endpoints are not disclosed for people with IAH and NAH separately. The randomized controlled iHART trial 9 assessed the difference between isCGM and rtCGM in people with T1D with IAH or recent severe hypoglycemia. After 8 weeks of treatment, people in the isCGM group had a significant decline in time spent above 270 mg/dL (15 mmol/L) and an increase of TIR, which is consistent with our findings. A possible reason for the lack of studies in people with IAH using isCGM could be that in many countries these people are eligible for rtCGM reimbursement, which is the preferred method to avoid hypoglycemia. 19 Indeed, in our previous real-world study about rtCGM reimbursement, 20 proportion-wise, more people with IAH were included than in the current FUTURE study.
People with IAH had worse QOL at baseline, even after correction for age and diabetes duration, especially for diabetes distress and worries owing to hypoglycemia. Low glucose levels are often associated with stressful effects on mood and emotions, which on the long term may provoke subsequent development of an anxiety state or depression. 21 Furthermore, the level of hypoglycemia awareness strengthens this negative impact, 22 which could explain the poorer scores on the PAID-SF and HFS-worry compared with people with NAH who had less episodes of (severe) hypoglycemia. In addition, research has identified a link between the severity of hypoglycemia and a detrimental effect on all eight SF-36 dimensions. 23 Conversely, we should take into account that the impact of hypoglycemia on QOL might also be explained by the prior psychological wellbeing of the individual. 22 In any case, our data illustrate that the multifaceted effects of hypoglycemia on daily life are considerable and can also have important clinical implications for diabetes management attainment. 24
To ascertain the effect of a new treatment on QOL, mainly validated questionnaires are used. We observed statistically significant changes in SF-36 subscales (for NAH), HFS-worry (for IAH), and DTSQ status and change (for IAH and NAH) after 24 months of isCGM use. However, statistical significance does not translate automatically into clinical relevance and is often overlooked when interpreting such outcomes. 25 For SF-36 in diabetes, a 1-point score change in norm-based scores could already be linked to a change of the risk on clear and intuitive outcomes, such as mortality, hospitalization, inability to work, and loss of work. 26 Yet, no such associations were studied for the other QOL scores, making interpretations less straightforward. Therefore, we calculated study-specific distribution-based minimum important differences based on the effect size of the score change 27 and evaluated them by Cohen's d. Consequently, the statistically significant declines in SF-36 scales for NAH cannot be considered of clinical importance. The 2-point improvement in hypoglycemia fear for IAH can be seen as a relatively small change, and the higher treatment satisfaction lies in the range of medium to large importance for both groups. In addition, comparing QOL across studies and therapies in T1D remains a challenge as a lot of heterogeneity is present in incorporated surveys. Thus, as patient-reported outcomes are gaining importance in T1D research and clinical practice, a list of recommended QOL measures should ideally be devised as is already the case for CGM metrics. 11
An important observed advantage of introducing isCGM is a significant reduction of severe hypoglycemia and hypoglycemic comas, particularly for people with IAH even without the integration of alarms. On the same lines, less hospitalizations for hypoglycemia could be observed for people with IAH, related to the observation that frequency in the year before isCGM use was three times higher than for people with NAH. No studies about isCGM to date report the frequency of these acute events for IAH and NAH separately, making comparisons with other populations difficult. The Swedish and French registry studies by Nathanson et al 28 and Roussel et al, 29 respectively, confirmed a fall in severe hypoglycemia when using isCGM versus finger stick measurements. Despite that the observed frequencies at baseline in the FUTURE study are 4–6 times lower than what was observed for people with IAH in the rtCGM RESCUE study, 20 avoidance of any of these events remains crucial owing to the important risks of recurrent and severe hypoglycemia 30 and the major impact on work productivity of people with T1D. 23
During the first 2 weeks of starting isCGM, it was already clear that people with IAH spent more time in hypoglycemia, with levels similarly as described by others. 31 Subsequent long-term isCGM use did result in a small decrease in time spent in hypoglycemia but mainly in a decrease in time spent in hyperglycemia with a consequent increase in TIR, which is different than the observed effects in people with NAH. This illustrates an imbalance between hypoglycemia concern and risk of severe hypoglycemia. The study by Anderbro et al 32 noted that 32% of those at high risk of severe hypoglycemia expressed low concern about hypoglycemia, which is in line with another study within the T1D Exchange Registry showing that those with IAH were more likely to prioritize avoidance of hyperglycemia. 33 In a cluster analysis of the HFS questionnaire, 34 only a little more than one-third of people with IAH expressed fear of hyperglycemia. Taken together, these cognitive attitudes represent a barrier to engage in common therapies to avoid hypoglycemia. 35 –37 In contrast, health care professionals often focus on avoidance of hypoglycemia, which might explain the observed decrease of prescribed insulin doses compared with before isCGM use.
The FUTURE population did not show a benefit on HbA1c levels, which is in contrast to the ABCD nationwide audit in the United Kingdom that included 10,370 isCGM users who showed a reduction in HbA1c from 8.3% (67.5 mmol/mol) at baseline to 7.8% (62.3 mmol/mol) after a mean of 7.5 months of follow-up. 17 However, this reduction could mainly be attributed to people with baseline HbA1c levels >8.5% (69.5 mmol/mol), which was also observed in other large cohorts. 28,38 –40 Moreover, in studies where baseline HbA1c levels were comparable with the FUTURE population, similar effects of isCGM on follow-up HbA1c could be observed. 28,40 None of these large real-world observations report on temporal sensor-measured outcome measures, which would be interesting to compare across different settings and reimbursement criteria for isCGM.
An important limitation of our study is the lack of blinded baseline isCGM data, limiting the evaluation of sensor-measured outcomes before versus after isCGM initiation and possibly underestimating the real impact on time in ranges. Furthermore, we used the electronic medical files to identify people as having IAH, which reflects the classification made by the treating health care professional. By using validated questionnaires like those of Gold et al 41 or Clarke et al, 42 we possibly could have identified an additional population with differing levels of hypoglycemia unawareness, as previous research estimated that 20% of people with T1D have IAH, 43 which is somewhat higher than that identified in the FUTURE population. Nevertheless, the used methodology returned a valid distinction between IAH and NAH as apparent from baseline differences, which are in line with previous research. 9,35,44 Finally, the device under review was the 14-day wear of the first version of the FreeStyle Libre without optional alarms. In the meantime, a second version with optional alarms has replaced the former version in many countries. This is however the case for almost all studies with diabetes technology because many devices under investigation are already replaced by next-generation devices by the time the study is finished, certainly in long-term studies. Nevertheless, this should not withhold research groups to investigate the impact of technology and to avoid lack of evidence-based use of these diabetes devices.
In summary, data after 24 months of isCGM use in a population of adults living with T1D show a sustained improvement of severe hypoglycemia, hypoglycemia coma, hospitalizations for hypoglycemia, and work absenteeism, mostly driven by people with IAH. Together with improved satisfaction with diabetes therapy irrespective of level of hypoglycemia awareness, isCGM even without alerts proves to be a valuable tool in the treatment of people with T1D.
Footnotes
Acknowledgments
The deepest gratitude goes to the participants of this study, who graciously gave their time for collection of data. The authors thank the data nurses, the local investigators, and the students for administering the questionnaires, completing the case reporting files, and collecting data. The authors also thank Steffen Fieuws for providing advice about the statistical analyses.
Authors' Contributions
S.C. designed the study, gathered and analyzed the data, performed statistical analyses, wrote the article, and made figures and tables. P.G. and C.M. designed the study, gathered and discussed the data, and wrote the article. C.D.B., N.B., L.V.H., and F.N. gathered and discussed the data and edited the article. S.C. and P.G. are guarantors of this work and, as such, had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Author Disclosure Statement
KU Leuven has received research support for S.C. from Roche Diabetes Care, Novo Nordisk, and Sanofi. C.D.B. reports consulting fees and honoraria for speaking for Abbott, AstraZeneca, Boehringer-Ingelheim, A. Menarini Diagnostics, Eli Lilly, Medtronic, Novo Nordisk, and Roche. L.V.H. received consulting fees and honoraria for speaking from Abbott, AstraZeneca, Boehringer-Ingelheim, Eli Lilly, Medtronic, Merck Sharp and Dohme, Novo Nordisk, Sanofi-Aventis, and Roche. F.N. reports consulting fees and honoraria for speaking from Abbott, AstraZeneca, Boehringer-Ingelheim, Eli Lilly, Johnson and Johnson, Medtronic, Merck Sharp and Dohme, Novo Nordisk, Roche, and Sanofi-Aventis. C.M. serves or has served on the advisory panel for Novo Nordisk, Sanofi, Merck Sharp and Dohme Ltd., Eli Lilly and Company, Novartis, AstraZeneca, Boehringer Ingelheim, Roche, Medtronic, ActoBio Therapeutics, Pfizer, Imcyse, Insulet, Zealand Pharma, Avotres, Mannkind, Sandoz, and Vertex. Financial compensation for these activities has been received by KU Leuven; KU Leuven has received research support for C.M. from Medtronic, Imcyse, Novo Nordisk, Sanofi and ActoBio Therapeutics; CM serves or has served on the speakers bureau for Novo Nordisk, Sanofi, Eli Lilly and Company, Boehringer Ingelheim, Astra Zeneca and Novartis. Financial compensation for these activities has been received by KU Leuven. P.G. serves or has served on the advisory panel for Novo Nordisk, Sanofi-Aventis, Boehringer-Ingelheim, Janssen Pharmaceuticals, Roche, Medtronic, Abbott and Bayer. Financial compensation for these activities has been received by KU Leuven. P.G. serves or has served on the speakers bureau for Merck Sharp and Dohme, Boehringer-Ingelheim, Bayer, Medtronic, Insulet, Novo Nordisk, Abbott, Roche, VitalAire and Dexcom. Financial compensation for these activities has been received by KU Leuven. KU Leuven received for P.G. nonfinancial support for travel from Sanofi-Aventis, A. Menarini Diagnostics, Novo Nordisk, Medtronic, and Roche. N.B. has nothing to disclose.
Funding Information
No funding was available; in particular, this study was conducted without support of Abbott Diabetes Care (Witney, United Kingdom).
Supplementary Material
Supplement 1
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Table S8
Supplementary Table S9
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.