
Abstract

Introduction
The year 2020 was dramatically impacted by the COVID‐19 pandemic. Primary care, and individuals managed in primary care, were disproportionately impacted, with many clinicians redeployed to manage frontline COVID‐19 care, clinics closed or limited by lack of PPE, and individuals with diabetes either in lockdown or conducting their lives largely remotely, because of the risk of contracting COVID‐19.
Diabetes care quality, which had plateaued even before the COVID‐19 pandemic, has been challenged in ways that no one had envisioned pre‐COVID‐19. At the same time, the challenges of COVID‐19 have created significant opportunities for care innovation and intensified use of diabetes technology in primary care settings. Many centers in the United States—and the rest of the world—pivoted quickly to remote diabetes management in the face of limitations to in‐person care, and for that, diabetes technology demonstrated its true value.
Beyond devices, the year saw continued expansion in the role of the SGLT2 and GLP‐1 medication classes in the management of type 2 diabetes, increased validation continuous glucose monitoring (CGM) use in the management of all individuals on insulin, and increased visibility of time in range as a glycemic quality metric and target. While HbA1c‐based management continues to dominate the world of diabetes management in primary care, there has been increasing recognition of the value of alternate measures and goals, with a shift to management based on glycemic metrics when HbA1c was unavailable because of the pandemic, and a shift to diabetes management beyond glycemia, with the increasing recognition that the SGLT2 and GLP‐1 medication classes have significant potential to modify the progression of diabetes complications in the short‐ and long‐term.
For this review, we have divided articles into five key areas of innovation for articles e‐published or published between the dates of July 2020 and June 2021. Cited articles were chosen for innovation, impact, or reach regarding diabetes assessment and management. The publications reviewed addressed the following questions: (1) How are we doing?; (2) Drugs and their use in primary care; (3) Devices and technologies in primary care; (4) Clinician and patient training; and (5) Connected care and care model innovation.
Key Articles Reviewed for the Article
Fang M, Wang D, Coresh J, Selvin, E
Powell RE, Zaccardi F, Beebe C, Chen Z, Crawford A, Cuddeback J, Gabbay RA, Kissela L Litchman ML, Mehta R, Meneghini L, Pantalone KM, Rajpathak S, Scribner P, Skelley JW, Khunti K
Tsapas A, Avgerinos I, Karagianis T, Malandris K, Manolopoulos A, Andreadis P, Liakos A, Matthews DR, Bekiari E
Brown E, Heerspink HJL, Cuthbertson DJ, Wilding JPH
Martens TW, Beck RW, Bailey R, Ruedy KJ, Calhoun P, Peters AL, Pop‐Busui R, Philis‐Tsimikas A, Bao S, Umpierrez G, Davis G, Kruger D, Bhargava A, Young Y, McGill JB, Aleppo G, Nguyen QT, Orozco I, Biggs W, Lucas KJ, Polonsky WH, Buse JB, Price D, Bergenstal RM for the MOBILE Study Group
Karter AJ, Parker MM, Moffet HH, Gilliam LK, Dlott R
Bergenstal RM, Kerr MSD, Roberts GJ, Souto D, Nabutovsky Y, Hirsch IB
Carlson AL, Huyett LM, Jantz J, Chang A, Vienneau T, Ly TT
Rodbard D and Garg S
Wilmot EG, Lumb A, Hammond P, Murphy HR, Scott E, Gibb FW, Platts J, Choudhary P
Bode B, King A, Russell‐Jones D, Billings LK
Wysham CH, Kruger DF
Phillip M, Bergenstal RM, Close KL, Danne T, Garg SK, Heinemann L, Hirsch IB, Kovatchev BP, Laffel LM, Mohan V, Parkin CG, Battelino T
Dixon RF, Zisser H, Layne JE, Barleen NA, Miller DP, Moloney DP, Majithia AR, Gabbay RA, Riff J
Bui A, Kim J
HOW ARE WE DOING?
Trends in Diabetes Treatment and Control in U.S. Adults, 1999–2018
Fang M, Wang D, Coresh J, Selvin E
Welch Center for Prevention, Epidemiology, and Clinical Research and the Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD
Background
It is important to track current trends in the management of diabetes and associated comorbidities to determine areas of improvement and identify gaps in quality. These trends may identify areas in need of focus and disparities in care, ultimately informing public health priorities.
Methods
In this study, data was extracted on all participants of the National Health and Nutrition Examination Survey (NHANES) that were nonpregnant, aged 20 years or older with a diagnosis of any type of diabetes (n=6,653) during the time period of 1999 through 2018. The cross‐sectional analysis of glycemic, blood pressure, and lipid control was conducted in 3‐year intervals starting in 1999 to 2002 and ending in 2015 to 2018.
Results
Glycemic control defined as glycated HbA1c <7% steadily improved from 1999 to 2010, peaking at 57.4% (95% CI, 52.9 to 61.8) during the 2007–2010 period, and gradually declining to 50.5% (95% CI, 45.8 to 55.3) during the 2015–2018 period. The use of any glucose‐lowering agents increased by 8.6 percentage points from the 1999–2002 period to the 2007–2010 period and remained steady thereafter. The use of metformin, insulin, and newer agents (e.g., SGLT2 inhibitors, GLP‐1 receptor agonists) increased from 1999 to 2018 with a concomitant decline in the use of sulfonylureas and thiazolidinediones (e.g., pioglitazone). Blood pressure (BP) control (<140/90 mmHg) steadily improved from 1999 to 2014, peaking at 74.2% (95% CI, 70.7 to 77.4) then declining to 70.4% (95% CI, 66.7 to 73.8) during the 2015–2018 period. Lipid control (non-HDL cholesterol <130 mg/dL) improved dramatically during the early 2000s and plateaued with minimal improvement from 52.3%; (95% CI, 49.2 to 55.3) in 2007–2010 to 55.7% (95% CI, 50.8 to 60.5) in 2015–2018. This was consistent with increased statin use that plateaued after 2014. An “all or none” composite control measure defined as glycated HbA1c <7%, blood pressure <140/90 mmHg and non-HDLL cholesterol <130 mg/dL showed steady improvement from 1999 to 2010 with a steady decline starting in 2011, ending with only 22.2% achieving the composite measure (95% CI, 17.9 to 27.3) in 2015–2018. Participants who were younger adults (<44 years of age), Mexican Americans, at lower income, and without health insurance were less likely to receive monotherapy or combination therapy when glycemic, BP, and lipid targets were not achieved.
Conclusions
The current trends in diabetes treatment and control are very concerning, with clear evidence of worsening of glycemic and blood pressure control along with a plateau in lipid control.
Comment
This study clearly demonstrates that our healthcare system, including primary care clinicians, continues to struggle to achieve metabolic control in patients with diabetes. Several plausible reasons exist, including therapeutic inertia and the impact of studies such as the 2010 Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial, which resulted in an overall perception that less-intensive management of glycemia and blood pressure is acceptable. While it is encouraging to see a decline in use of sulfonylureas and thiazolidinediones and a rise in newer disease‐modifying medications such as SGLT2 inhibitors and GLP‐1 receptor agonists, their high cost may preclude widespread use. This study also demonstrated that disparities in diabetes care and treatment exist for those in high‐risk racial or ethnic groups and those patients with lower income or that are uninsured/underinsured. Attention must be paid to the social determinants of health to overcome these disparities in care. On a more positive note, the integration of new technology, such as continuous glucose monitoring and automated blood pressure monitoring in primary care, may have the potential to bend the current trend line in diabetes care and treatment in a more positive direction.
Strategies for Overcoming Therapeutic Inertia in Type 2 Diabetes: A Systematic Review and Meta‐Analysis
Powell RE1, Zaccardi F2, Beebe C3, Chen Z4, Crawford A1, Cuddeback J5, Gabbay RA4,6, Kissela L4 Litchman ML7, Mehta R8, Meneghini L9, Pantalone KM10, Rajpathak S11, Scribner P4, Skelley JW12, Khunti K2
1Mathematica, Princeton, NJ; 2Leicester Real World Evidence Unit, Leicester Diabetes Research Centre, University of Leicester, Leicester, UK; 3Quantumed Consulting, San Diego, CA; 4American Diabetes Association, Arlington, Virginia; 5AMGA (American Medical Group Association), Alexandria, Virginia; 6Harvard Medical School, Boston, MA; 7University of Utah College of Nursing, Salt Lake City, UT; 8Healthagen, a CVS Health Company, Scottsdale, AZ; 9UT Southwestern Medical Center, Parkland Health and Hospital System, Dallas, TX; 10Endocrinology and Metabolism Institute, Cleveland Clinic, Cleveland, OH; 11Merck & Co., Inc., Kenilworth, NJ; 12Samford University, Department of Pharmacy Practice, Birmingham, AL
Background
Therapeutic inertia is defined as the failure of healthcare providers to initiate, intensify, or de-escalate therapy when it is clearly appropriate based on current evidence‐based guidelines or protocols. While multifactorial in nature, therapeutic inertia is thought to stem from patient‐, provider‐, and health system–level factors that collectively lead to poor outcomes in patients with diabetes. The aim of this study was to move beyond categorizing the causes of therapeutic inertia and determine the effectiveness of different interventional strategies designed to overcome it.
Methods
Five large databases where electronically searched to identify randomized controlled trials or quasi‐experimental studies published between 2004 and 2019 that measured the impact of different healthcare interventional strategies on the level of glycemic management defined as change in glycated HbA1c. The interventions were categorized into four different groups, including (1) care management and patient education; (2) nurse or certified diabetes educator (CDE); (3) pharmacist‐based; or (4) physician‐based. The primary outcome was the mean difference in HbA1c change between the intervention and control groups.
Results
A total of 36 studies representing 22,243 participants with type 2 diabetes (T2D) meeting the strict inclusion criteria were included in the nonlinear random‐effects meta‐analysis. The majority (28 of 36) were randomized controlled trials and the remaining 8 were quasi‐experimental studies that used a matched comparison group as control. Seventy‐two percent of the interventions were conducted in the United States with the remainder in Europe, Australia, Canada, and South Africa. The table below summarizes the results.
The pharmacist‐based and nurse‐ or CDE‐based interventions had the most consistent reduction in HbA1c, and only one out of seven physician‐based interventions resulted in a lower HbA1c. Nonlinear random effect meta‐regression analysis demonstrated that reduction in HbA1c was greatest at 6 months (−0.38% [95% CI −0.56, −0.20]; −4.2 mmol/mol [95% CI −6.2, −2.2]), declining to −0.15% [95% CI −0.30, 0.01]; 1.6 mmol/mol [95% CI −3.3, 0.1] at 1 year. Interventions lasting greater than 1 year did not demonstrate an overall reduction in HbA1c. Regardless of the type of intervention, reduction in HbA1c was primarily found when patients had a baseline HbA1c >9% (75 mmol/mol).
Conclusions
The present study demonstrated that nonphysician‐based interventions using pharmacists, nurses, CDEs, or care managers are the most effective approaches to overcome therapeutic inertia and improve glucose management.
Comment
The quality of diabetes care continues to slowly decline, even with the availability of effective medications and technology to help patients manage their disease. Therapeutic inertia is clearly at the core of this decline. From a provider perspective, many factors can lead to therapeutic inertia, including shortage of time, lack of familiarity with new medications and evidence‐based guidelines, along with lack of awareness of the current level of diabetes care they provide that may lead to overconfidence. This article addressed how effective different interventions are at overcoming therapeutic inertia. The takeaway message is clear: to improve diabetes management, physicians must embrace a team approach where other nonphysician members of the team (nurses, CDEs, care managers, and pharmacists) are involved. These members of the diabetes team have the time, skills, and evidence‐based guidelines to provide the tools, resources, and education needed to allow patients to successfully self‐manage their diabetes. Successful diabetes management is a patient‐centered team sport.
DRUGS AND THEIR USE IN PRIMARY CARE
Comparative Effectiveness of Glucose‐Lowering Drugs for Type 2 Diabetes: A Systematic Review and Network Meta‐Analysis
Tsapas A1,2, Avgerinos I3, Karagianis T3, Malandris K3, Manolopoulos A3, Andreadis P3,4, Liakos A3, Matthews DR5, Bekiari E1
1Clinical Research and Evidence‐Based Medicine Unit and Diabetes Center, Aristotle University of Thessaloniki, Thessaloniki, Greece; 2Harris Manchester College, University of Oxford, Oxford, UK; 3Clinical Research and Evidence‐Based Medicine Unit, Aristotle University of Thessaloniki, Thessaloniki, Greece; 4North West Anglia NHS Foundation Trust, Peterborough City Hospital, Peterborough, UK; 5Harris Manchester College, University of Oxford, and Oxford Center for Diabetes, Endocrinology, and Metabolism, Oxford, UK
Background
The number of therapeutic options for the management of type 2 diabetes (T2D) has grown significantly in the last decade. In recent years, there is increasing evidence that some antihyperglycemic agents can have benefits beyond glycemic management, namely with regard to vascular and renal outcomes. Thus the decision regarding which medication(s) to add for patients needing additional glycemic lowering beyond diet, lifestyle, and most commonly metformin, has shifted the focus to the presence of atherosclerotic disease, heart failure, and chronic kidney disease (or their risk factors). However, direct comparison data between the currently available antihyperglycemic agents in T2D are sparse. This comparative effectiveness and network meta‐analysis seeks to overcome some limitations of previous meta‐analyses and includes data from randomized, controlled trials of anti‐diabetic drugs on important clinical outcomes to help clinicians make more informed decisions as they discuss treatment options with patients.
Methods
The authors selected English‐language randomized trials (of at least 24 weeks intervention) specifically evaluating the effects of these therapies on mortality, glycemic, and vascular outcomes. The study group used pairs of reviewers to assess for and mitigate bias. Therapeutic agents included metformin, sulfonylureas, pioglitazone, DPP‐4 inhibitors, GLP‐1 receptor agonists, SGLT2 inhibitors, alpha‐glucosidase inhibitors, meglitinides, pre‐mixed insulins, basal insulins, and basal‐bolus insulin regimens. All medications were evaluated by class, with the exception of GLP‐1 receptor agonists and SGLT2 inhibitors, for which intra‐class assessments were made. The authors used change from baseline in HbA1c and all‐cause mortality as the primary outcomes for the network meta‐analysis. Secondary outcomes included severe hypoglycemia, cardiovascular death, stroke, myocardial infarction, hospitalization for heart failure, diabetic retinopathy, and amputation.
Results
The electronic database searches yielded 453 eligible trials (which included 320,474 patients) assessing 21 different diabetes treatments from 9 drug classes. Less than a quarter of the studies involved drug‐naïve patients, whereas over half of them included interventions as add‐on to metformin‐based therapy (i.e., metformin only or metformin plus other agents). In patients at low cardiovascular risk, neither drug‐naïve nor those on metformin‐based background treatment had any clinically meaningful difference in mortality or vascular outcomes. In those at increased cardiovascular risk on metformin‐based background treatment, oral semaglutide, empagliflozin, liraglutide, extended‐release exenatide, and dapagliflozin showed reduced all‐cause mortality, with oral semaglutide, empagliflozin, and liraglutide also showing reduced cardiovascular death. SGLT2 inhibitors reduced heart failure hospitalization and end‐stage renal disease. Adverse outcomes demonstrated increased retinopathy with subcutaneous semaglutide and increased amputation with canagliflozin. Of note, most studies (n=360) were funded by the pharmaceutical industry, and characterization of cardiovascular risk differed between studies.
Conclusions
Metformin use as the first‐line treatment of drug‐naïve patients at low cardiovascular risk remains evidence-based. For those on metformin at low cardiovascular risk, these data do not inform the next optimal therapeutic choice, whereas for those at increased cardiovascular risk already on a metformin‐based regimen, GLP-1 receptor agonists and SGLT2 inhibitors are optimal add‐on therapies based on cardiovascular risk profiles, therapeutic priorities, and patient personal preferences.
Comment
Given the lack of robust head‐to‐head prospective studies, this comparative analysis and network meta‐analysis help fill in some of the knowledge gaps most important to the clinician treating patients with T2D, with the majority of these clinicians practicing in primary care. The 2021 American Diabetes Association Standards of Care (in addition to other published guidelines) advocate for using the presence of atherosclerotic cardiovascular disease, heart failure, and chronic kidney disease as the driving factor for pharmacologic treatments after metformin. This current study supports this, with some additional interesting findings. As seen in the preliminary results of the GRADE study (presented at the American Diabetes Association Scientific Sessions, June 28, 2021), which was a randomized, prospective comparative analysis study in T2D, GLP‐1 receptor agonists and basal insulin showed the most robust HbA1c lowering. Also observed in this study, similar to GRADE, was a higher risk of severe hypoglycemia with sulfonylurea but not with basal insulin. Thus to the primary care clinician who is prioritizing avoidance of hypoglycemia, sulfonylurea may be less favorable than basal insulin.
SGLT2 Inhibitors and GLP‐1 Receptor Agonists: Established and Emerging Indications
Brown E1,2, Heerspink HJL3, Cuthbertson DJ1,2, Wilding JPH1,2
1Department of Metabolic and Cardiovascular Medicine, Institute of Life Course and Medical Sciences, University of Liverpool, Liverpool, UK; 2Liverpool University Hospitals NHS Foundation Trust, Longmoor Lane, Liverpool, UK; 3Department of Clinical Pharmacy and Pharmacology, University of Groningen, University Medical Centre Groningen, Groningen, Netherlands
Background
The sodium glucose cotransporter 2 (SGLT2) inhibitor and glucagon‐like peptide‐1 (GLP‐1) receptor agonist classes of medications have been approved for the management of type 2 diabetes for many years. More recent cardiovascular outcome trials (CVOTs) and trials conducted in specific populations (e.g., patients with chronic kidney disease) have demonstrated that these classes of medications have additional cardio‐ and renal‐protective effects beyond lowering glucose.
Methods
This comprehensive review article contained citations limited to human subjects identified through searches of PubMed up to May 2021 using terms “glucagon‐like peptide‐1 (GLP‐1) receptor agonist” and “sodium glucose cotransporter 2 (SGLT2) inhibitor.” In addition, the generic drug names of all “gliflozins” and “glutides” were searched in PubMed using the same date range. All evidence‐based guidelines for the management of type 2 diabetes and cardiovascular disease published by the American Diabetes Association (ADA), European Association for the Study of Diabetes (ESAD), and European Society of Cardiology (ESC) were reviewed for potentially relevant articles. The authors also supplemented this with peer‐reviewed articles cited in retrieved articles and review articles to make the articles included as comprehensive as possible.
Results
The impact of the SGLT2 inhibitors on three‐point major adverse cardiovascular events (MACE) (non‐fatal MI, non‐fatal stroke, CV death) is variable, with an overall trend for modest reduction. Where this class shows a clear benefit is with reduction in hospitalization for heart failure (HHF) with a consistent relative risk reduction of 30% to 35% for all the gliflozins. The review also demonstrated a clear class effect on reducing the progression of renal disease (e.g., slower decline in eGFR and less ESKD) regardless of the composite renal outcome measure studied. Analysis of the gliflozins demonstrated a class effect on genital yeast infection affecting up to 10% of women. Importantly, there was no increased risk of bacterial urinary tract infections. Reports of necrotizing fasciitis of the perineum (Fournier's gangrene) have been reported in pharmacovigilance data, but analysis of adverse events in large cardiovascular outcome trials (CVOTs) did not show an increased risk. Euglycemic diabetic ketoacidosis (DKA) has been reported and is associated with off‐label use in type 1 diabetes, insulin use, intercurrent infection, and surgery.
Review of the GLP‐1 receptor agonists demonstates this class is very effective at lowering HbA1c along with significant weight loss in the range of 5%–10%. A meta‐analysis of all the GLP‐1 receptor agonists demonstrated that this class reduces three‐point MACE and all‐cause mortality by 12% (HR 0.88; 95% CI 0.82–0.94 for MACE and 95% CI, 0.83–0.95 for all‐cause mortality) (1). While not as impressive as that seen in the SGLT2 inhibitors, the meta‐analysis showed HHF was also reduced by 9% (HR 0.91, 95% CI 0.83–0.99). Analysis of secondary renal end points from the GLP‐1 receptor agonist cardiovascular outcomes trials with most of the benefit coming for the reduction in new onset or progression of albuminuria, and not from slowing the decline in eGFR. The most common adverse events are gastrointestinal in nature, particularly nausea, which was reported in the range of 25%–65% of patients treated with GLP‐1 receptor agonist. The risk of acute pancreatitis or pancreatic cancer does not appear to be higher than placebo or other diabetes medications. Reassuringly, the GLP‐1 receptor agonists do not appear to increase the risk of medullary thyroid carcinomas.
Conclusions
SGLT2 inhibitors and GLP‐1 receptor agonists are considered second‐line, or even arguably first‐line, glucose‐lowering therapies in patients with atherosclerotic cardiovascular disease, heart failure, and chronic kidney disease. They should be added to metformin regardless of the current level of glycemic control.
Comment
The SGLT2 inhibitors and GLP‐1 receptor agonists are disease‐modifying medications that do so much more to protect patients with type 2 diabetes beyond lowering HbA1c. All major diabetes and cardiovascular professional organizations have embraced the overwhelming research to recommend these medications for patients that have a history, or are at high risk, of atherosclerotic cardiovascular disease, heart failure, or chronic kidney disease. While the preponderance of the data on SGLT2 inhibitors and HHF have focused on patients with a reduced ejection fraction of <40% (HFrEF), the recently, published EMPEROR‐Preserved study of patients with class II–IV HF and ejection fraction of greater than 40% showed benefit versus placebo (2). Unfortunately, primary care has not kept up with the evidence‐based guidelines and these import classes are still underused.
DEVICES AND TECHNOLOGIES IN PRIMARY CARE
Effect of Continuous Glucose Monitoring on Glycemic Control in Patients with Type 2 Diabetes Treated with Basal Insulin: A Randomized Clinical Trial
Martens TW1, Beck RW2, Bailey R2, Ruedy KJ2, Calhoun P2, Peters AL3, Pop‐Busui R4, Philis‐Tsimikas A5, Bao S6, Umpierrez G7, Davis G7, Kruger D8, Bhargava A9, Young Y10, McGill JB11, Aleppo G12, Nguyen QT13, Orozco I14, Biggs W15, Lucas KJ16, Polonsky WH17, Buse JB10, Price D18, Bergenstal RM19 for the MOBILE Study Group
1International Diabetes Center, Park Nicollet Internal Medicine, Minneapolis, MN; 2Jaeb Center for Health Research, Tampa, FL; 3Keck School of Medicine of the University of Southern California, Los Angeles, CA; 4University of Michigan, Ann Arbor, MI; 5Scripps Whittier Diabetes Institute, San Diego, CA; 6Vanderbilt University Medical Center, Nashville, TN; 7Emory University School of Medicine, Atlanta, GA; 8Henry Ford Health System, Detroit, MI; 9Iowa Diabetes Research, West Des Moines, IA; 10University of North Carolina School of Medicine, Chapel Hill, NC; 11Washington University School of Medicine, St Louis, MO; 12Feinberg School of Medicine, Northwestern University, Chicago, IL; 13Las Vegas Endocrinology, Henderson, NV; 14Carteret Medical Group, Morehead City, NC; 15Amarillo Medical Specialists, Amarillo, TX; 16Diabetes & Endocrinology Consultants PC, Morehead City, NC; 17Behavioral Diabetes Institute, San Diego, CA; 18Dexcom Inc, San Diego, CA; 19International Diabetes Center, HealthPartners Institute, Minneapolis, MN
This manuscript is also discussed in article on Continuous and Intermittent Glucose Monitoring in 2021, page XX
Background
Continuous glucose monitoring (CGM) use has been shown to be helpful in the management of adults with type 1 diabetes (T1D), and with type 2 diabetes (T2D) on intensive insulin regimens, but use by individuals with T2D on basal insulin but not prandial insulin has not been well studied.
Methods
This randomized controlled trial was conducted at 15 centers in the United States and studied adults with T2D on long‐acting or intermediate-acting insulin, but not prandial insulin, with or without other glucose‐lowering medications, with diabetes being managed in primary care. Participants were randomized in a 2:1 allocation to either use of CGM or traditional fingerstick blood glucose monitoring (BGM), in the management of their diabetes, and were followed over 8 months. Primary outcome measure was differential changing in HbA1c; key secondary outcome measures were differential change in CGM‐measured time in glucose range of 70–180 mg/dL, and time with glucose level >250 mg/dL, as well as mean glucose level at 8 months.
Results
A total of 175 randomized participants had a mean age of 57 (SD 9 years), were 50% female, 53% racial or ethnic minorities, and had a mean baseline HbA1c level of 9.1% (SD 0.9%). Of these 175 individuals, 165 (94%) completed the trial. In the CGM group, mean HbA1c decreased from 9.1% at baseline to 8.0% at 8 months, while in the BGM group, the decrease was 9.0% at baseline to 8.4% at 8 months (adjusted difference, −0.4% [95% CI, −0.8% to −0.1%]; P=.02). Additionally, the CGM group had improvement in time in target glucose range of 70–180 mg/dL of 59%, versus 43% in the BGM group (adjusted difference, 15% [95% CI, 8% to 23%]; P<0.001), improved hyperglycemia, with 11% of time versus 27% with a glucose of greater than 250 mg/dL (adjusted difference, −16% [95% CI, −21% to −11%]; P<0.001), and a lower mean glucose of 179 mg/dL versus 206 mg/dL (adjusted difference, −26 mg/dL [95% CI, −41 to −12]; P<0.001). Severe hypoglycemic events were rare, occurring in 1% of the CGM group and 2% of the BGM group.
Conclusions
In adults with suboptimally controlled T2D treated with basal insulin but not prandial insulin, CGM, as compared to BGM, resulted in significantly lower HbA1c levels at 8 months.
Comment
The use of CGM in the management of insulin‐dependent diabetes is well supported for individuals with T1D; it is the current standard of care. In T2D, use of real‐time CGM has previously been shown to be of benefit for individuals using multiple daily dose insulin in the Diamond Study (3), and this has translated into real‐world benefit as shown by Karter and colleagues in data published simultaneously with the publication of the MOBILE study data in JAMA (4). For individuals using multiple daily dose insulin, this data has translated into availability of CGM for management of their diabetes for many, including those covered by Medicare in the United States, and by many commercial carriers in the United States and by National Healthcare systems outside the United States. The data presented in the MOBILE study extends the benefit of CGM to individuals using less-intensive insulin regimens not involving prandial insulin, and also showed significant benefit across a very diverse population of patients. It is hoped that this data will translate into increased support in guidelines for this broader group of individuals with insulin‐managed diabetes, and increased availability of CGM for all individuals managing their diabetes with insulin, regardless of regimen, demographics, or medical coverage.
Association of Real‐Time Continuous Glucose Monitoring with Glycemic Control and Acute Metabolic Events Among Patients with Insulin‐Treated Diabetes
Karter AJ1, Parker MM1, Moffet HH1, Gilliam LK2, Dlott R3
1Division of Research, Kaiser Permanente, Oakland, CA; 2Kaiser Northern California Diabetes Program, Endocrinology and Internal Medicine, Kaiser Permanente, South San Francisco Medical Center, South San Francisco, CA; 3Population Care, Regional PROMPT, Regional Clinical, Thyroid Subgroup, TPMG Regional Laboratory Services, Division of Endocrinology ‐ Diablo Service Area, Martinez, CA
Background
Continuous glucose monitoring (CGM) use is currently recommended for individuals with type 1 diabetes (T1D) based on multiple lines of observational and research‐based evidence. Observational evidence for CGM use in individuals with type 2 diabetes (T2D) on insulin is less robust.
Methods
This is an exploratory retrospective cohort study of individuals receiving care in the Kaiser system of Northern California, managing either T1D or T2D with insulin, comparing glycemic outcomes for those initiating real‐time CGM, compared to non‐initiation of real‐time CGM, between 2014 and 2019. Comparator groups were being treated with insulin, were self‐monitoring glucose levels, and did not have prior CGM use. Ten end points were measured during the 12 months preceding and the 12 months after initiation. End points included HbA1c; hypoglycemia or hyperglycemia requiring emergency room (ER) or hospital visit; HbA1c levels <7%, <8%, and >9%; ER or hospital encounters for any reason; and number of outpatient and telephone visits.
Results
A total of 3,806 patients initiating CGM (mean age, 42.4 years [SD, 19.9 years]; 51% female; 91% T1D, 9% T2D) were compared to 37,947 patients not initiating CGM (mean age, 63.4 years [SD, 13.4 years]; 49% female; 6% T1D, 94% T2D). Initiators of CGM had lower baseline HbA1c, but higher baseline rates of hypoglycemia and hyperglycemia. Use of real‐time CGM was associated with significantly lower HbA1c (differential −0.40%; 95% CI, −0.48% to −0.32%; P<0.001) after initiation, as well as lower rates of ER visit or hospitalization for hypoglycemia (differential −2.7%; 95% CI, −4.4% to −1.1%; P=.001), compared to non‐users of CGM. There were also statistically significant differences in the proportion of patients with HbA1c <7% (differential 9.6%; 95% CI, 7.1% to 12.2%; P<0.001), <8% (differential 13.1%; 95% CI, 10.2% to 16.1%; P<0.001), and >9% (differential −7.1%; 95% CI, −9.5% to −4.6%; P<0.001) after initiation CGM. CGM use was not associated with statistically significant difference in rates of hyperglycemia, ER visits, or hospitalization for any reason.
Conclusions
This retrospective cohort study of insulin‐treated individuals with T1D or T2D selected by clinicians for real‐time CGM use, compared to non‐initiators, had significantly more HbA1c improvement and significantly less ER visits and hospitalizations for hypoglycemia. The observational nature of this study may have increased susceptibility to selection bias in the results.
Comment
While use of CGM in the management of T1D is well established in many studies, use of CGM in the management of T2D is less well established, and less well supported by real‐world data. Use in individuals with T2D on multiple daily dose insulin is supported by the Diamond Study (3), and use in individuals on basal insulin regimens is supported by the MOBILE Study (published in the same issue of JAMA as this article) (5), but observational evidence for the use of CGM in individuals managing T2D on insulin has previously been limited. This large retrospective cohort study extends the findings previously established in the randomized controlled trials cited above, to real‐world populations, and adds critical real‐world context in supporting the use of CGM across all populations managing diabetes on insulin. An important subnote to this study is the finding that populations more heavily impacted by social determinants of health were less likely to be prescribed CGM. There is a pressing need for further research to help identify and minimize the barriers to use of diabetes technology in disadvantaged populations, which often suffer the double burden of increased prevalence of diabetes and its complications, yet decreased access to the tools needed to optimally manage diabetes.
Flash CGM Is Associated with Reduced Diabetes Events and Hospitalizations in Insulin‐Treated Type 2 Diabetes
Bergenstal RM1, Kerr MSD2, Roberts GJ2, Souto D3, Nabutovsky Y2, Hirsch IB4
1International Diabetes Center, Park Nicollet and HealthPartners, Minneapolis, MN; 2Abbott, Sylmar, CA; 3Abbott Diabetes Care, Alameda, CA; 4University of Washington School of Medicine, Seattle, WA
Background
While we have data on the benefits of CGM on glycemic management, we have little data on the role of CGM in reducing the risk of acute complications leading to emergency services or hospitalizations. Large databases of medical claims may provide key data to understand the possible role of CGM in these areas.
Methods
A retrospective real‐world study was conducted analyzing the IBM MarketScan Commercial and Medicare Supplemental databases to understand if the use of CGM (in this case, flash CGM) could impact acute medical events and hospitalizations for individuals with T2D. The medical records of individuals (N=2,463) who were on rapid acting insulin and presumed basal insulin were tracked, using ICD‐10 codes, for 6 months before and for 6 months after they acquired a CGM system and acute medical events and hospitalizations were recorded.
Results
Acute medical events decreased by 61%, from 0.180 to 0.072 events/patient-year (hazard ratio [HR] 0.39 [0.30, 0.51]; P<0.001)
Conclusions
The use of flash CGM was associated with a lowering of acute medical events and hospitalizations among individuals with T2D on presumed basal/bolus therapy. In addition to improving glucose management, these data support the use of CGM in T2D patients on insulin therapy as a means to reduce adverse clinical outcomes and possibly reduce costs.
Comment
The early emphasis on showing the value of CGM has been on generating data to show CGM can guide therapy decisions and lifestyle choices to improve time in range and minimize hypoglycemia, which in turn is usually associated with an improved HbA1c. As CGM is used more widely in primary care and CGM data are integrated into the electronic health record (EHR), we will be in a better position to confirm and extend the findings of this observational analysis of a large claims data base. Insurers and employers are eager to see a reduction in acute and costly diabetes complications to continue to broaden their coverage of CGM and to invest in CGM‐based disease‐management programs.
Improved Glycemic Control in 3,592 Adults with Type 2 Diabetes Mellitus Initiating a Tubeless Insulin Management System
Carlson AL1, Huyett LM2, Jantz J2, Chang A2, Vienneau T2, Ly TT2
1International Diabetes Center, Minneapolis, MN; 2Insulet Corporation, Acton, MA
This manuscript is also discussed in article on Insulin Delivery Hardware: Pumps and Pens, page XX
Background
Many patients with type 2 diabetes (T2D) benefit from treatment with insulin‐based regimens, including multiple daily injections. There have been several advancements in insulin delivery technology in recent years, with several continuous subcutaneous insulin infusion systems available. These insulin pump systems have clearly demonstrated improvements in the care of patients with type 1 diabetes (T1D); however, the benefit of such systems has not been as well described in those with T2D. The tubeless patch pump system, Omnipod (Insulet, Acton, MA) is one such insulin delivery system, which uses a tubeless “patch” pump that can be fully programmed to deliver basal and bolus insulin. This study sought to investigate the potential use for such a system in a real‐world study in adults with T2D.
Methods
This retrospective, observational study used data collected from existing datasets regularly collected by the manufacturer of a large cohort in the United States from January 2014 to May 2020. The manufacturer's staff collecting the data included diabetes educators and registered dieticians/nurses who work with both patients and clinicians to support patients on this system. The primary outcome was a change in HbA1c from baseline (prior to starting on the Omnipod system) to 90 days (or as close to 90 days as possible) after the initiation of the device. Secondary outcomes included the change in total daily dose of insulin (TDD) and self‐reported frequency of hypoglycemia.
Results
Of the available 7,359 adults in the database, only 3,592 had both baseline and follow‐up HbA1c data and thus were included in the analysis. The baseline HbA1c was 9.2%±2.0% with patient‐reported TDD of 103±70 units and 1.2±2.0 hypoglycemia episodes per week. The majority of patients were previously on multiple daily injections of insulin (74%) compared to those on other insulin pumps (15%). At follow‐up, the HbA1c decreased significantly (P<0.0001) to 7.9%±1.3%, for a net change of −1.3%. The TDD at follow‐up decreased to 71±41 units for a net decrease of 33 units per day. Similar to HbA1c, those previously on multiple daily injections saw the largest decrease in TDD (−35 units). With regard to hypoglycemia, the self‐reported number of hypoglycemia episodes (<70 mg/dL) per week decreased significantly from 1.2±2.0 to 0.7±1.1 episodes per week (n=2,922; P<0.0001).
Conclusions
After 90 days on the Omnipod system, this cohort of adults with T2D showed a significant decrease in HbA1c, TDD, and hypoglycemia. This improvement in HbA1c was achieved with more than a 30% decrease in TDD, noting that TDD is often a limiting factor in using insulin pump therapy for those with T2D. Given the potential for more severe diabetes‐related complications with higher HbA1c levels, the observation that the number of patients achieving an HbA1c <7% more than doubled with starting this pump system, and the finding that those with the highest baseline HbA1c saw the largest decrease in HbA1c, imply this type of insulin pump system could be beneficial for those with T2D at higher HbA1c levels to start. The reported reduction in hypoglycemia events is also a reassuring finding for those starting on this pump system. The study is limited by its retrospective design and also by some of the data being self‐reported by patients.
Comment
This study has many findings that should be of interest to primary care clinicians, namely that moving someone from multiple daily injections to an insulin pump system can result in reduced HbA1c (particularly those starting with a higher HbA1c at baseline), while lowering TDD and hypoglycemia. Some of the common barriers to using basal/bolus insulin therapy in primary care are cost concerns (T2D can often require higher TDD, which can be cost‐prohibitive, especially in the United States), and real or perceived fear of hypoglycemia can lead to clinical inertia in insulin titration. This retrospective study did not assess the frequency and amount of insulin titration (i.e., no additional interventions were made during the study period), but to see these results without a clearly specified insulin titration schema suggests that a more established titration program with frequent adjustments could see even bigger improvements in diabetes outcomes. This was a relatively short study, so it remains uncertain if further observation would show durability of the findings. However, in the era of value‐based care, the observation of a −1.3% decrease in HbA1c and the mean follow‐up HbA1c being < 8% is promising for this technology in T2D. It also underscores the need to develop systems to support primary care clinicians in the implementation of pump therapy and protocols for frequent titration of insulin pump technology to improve outcomes.
Standardizing Reporting of Glucose and Insulin Data for Patients on Multiple Daily Injections Using Connected Insulin Pens and Continuous Glucose Monitoring
Rodbard D1 and Garg S2
1Biomedical Informatics Consultants LLC, Clinical Biostatistics Department, Potomac, MD; 2Barbara Davis Center for Diabetes, Departments of Medicine and Pediatrics, University of Colorado Anschutz Medical Campus, Aurora, CO
Background
The number of insulin‐requiring patients with diabetes is increasing worldwide. A small number of those people, mostly with type 1 diabetes, use insulin pumps with sophisticated features for insulin delivery and recording of insulin delivery metrics. For the increasing population using multiple daily injections of insulin (MDI), features currently available to individuals using insulin pumps, such as automated recording of insulin doses or “memory” of such dosing, have not been available until recently, with the development of insulin “smart pens.” These pens connect to an application to collect, store, analyze, and display insulin dosing data in combination with glucose data, allowing improved management guidance for both healthcare providers and patients. Recently there have been calls to standardize reports produced by automated insulin delivery systems, and the authors here call for an urgent need to likewise standardize the connected insulin pen metrics and reports using a one‐page summary or “dashboard.” In this report they present one such prototype for displaying these data.
Methods
The authors used a review of the literature and their own experience with multiple systems to create their connected pen report. Using glucose and insulin data displays from blood glucose meters, continuous glucose monitors, insulin pumps, automated insulin delivery systems, and insulin pens, they used this review and experience to develop and propose a one‐page prototype report for connected insulin pens.
Results
The authors propose five metrics to be included in a one‐page report: (1) glucose metrics (such as time in ranges); (2) insulin metrics (including type of insulin and doses, as well as timing of doses); (3) an enhanced ambulatory glucose profile (AGP); (4) user experience such as alarms, and lifestyle factors if data are available, such as meals, exercise, sleep, etc.; (5) clinical insights and interpretation.
Conclusions
This report presents a prototype standardized approach using a one‐page dashboard report to summarize and display connected insulin pen data for patients on MDI therapy.
Comment
The historical variability of diabetes data display between individual devices is shifting toward standardization of data display across all devices, platforms, and manufacturers, though up to now this has been primarily for insulin pumps and continuous glucose monitors. This methodology has been invaluable for both clinicians and patients as they seek to have a systematic approach to the management of patients in the increasingly complex landscape of diabetes management. In this paper we see this approach applied to those on MDI therapy, for whom such standardization is currently lacking. While the authors acknowledge that some adjustments to this prototype will likely be desired by individual or subsets of users, the fundamental glucose and insulin metrics included here are consistent with other standardized reports and should be intuitive to those familiar with other diabetes technologies. Importantly, connected smart pens for the first time allow easy access to glucose data directly displayed next to the amount and timing of insulin data for those using MDI, something that was previously only available for insulin pump users. With more patients expected to be using MDI in the future, this advantage in providing much more comprehensive data will hopefully facilitate more informed, personalized, and frequent insulin dose adjustments to help patients meet and maintain their glucose targets.
CLINICIAN AND PATIENT TRAINING
Time in Range: A Best Practice Guide for UK Diabetes Healthcare Professionals in the Context of the COVID‐19 Global Pandemic
Wilmot EG1,2, Lumb A3,12, Hammond P4, Murphy HR5,6, Scott E7, Gibb FW8,9, Platts J10, Choudhary P11,13
1Diabetes Department, Royal Derby Hospital, University Hospitals of Derby and Burton NHS Foundation Trust, Derby, UK; 2Faculty of Medicine and Health Sciences, University of Nottingham, Nottingham, UK; 3Oxford Centre for Diabetes, Endocrinology and Metabolism, University of Oxford, Oxford, UK; 4Diabetes Resource Centre, Harrogate District Hospital, Harrogate and District NHS Foundation Trust, Harrogate, UK; 5Norwich Medical School, University of East Anglia, Norwich, UK; 6Women's Health Academic Centre, Division of Women's and Children's Health, King's College London, London, UK; 7Leeds Institute for Cardiovascular and Metabolic Medicine, University of Leeds, Leeds, UK; 8Edinburgh Centre for Endocrinology & Diabetes, Royal Infirmary of Edinburgh, Little France Crescent, Edinburgh, UK; 9Centre for Cardiovascular Science, University of Edinburgh, Edinburgh, UK; 10Diabetes Centre, University Hospital Llandough, Cardiff and Vale University Health Board, Penarth,UK; 11Department of Diabetes, School of Life Course Sciences, King's College London, London, UK; 12NIHR Oxford Biomedical Research Centre, Oxford, UK; 13Leicester Diabetes Centre, University of Leicester, Leicester, UK
Background
Continuous glucose monitoring (CGM) technology has improved glycemic management and quality of life for people with diabetes, and recent changes in access to continuous glucose monitoring systems in the UK medical system have allowed more people to benefit from CGM technology. Limitations to in‐person healthcare imposed by the COVID‐19 pandemic have created an opportunity to optimize remote management using CGM‐based time in range glycemic measures.
Methods
The authors review the use of time-in-range- (TIR) based management in routine clinical care, as an actionable and direct target for glycemic improvement. They review the evidence for its use, including the link between TIR and risk of developing diabetes complications, and the correlation with HbA1c, which currently is the established gold standard for population‐based diabetes care quality assessment. They review TIR‐based glycemic targets, based on the 2019 International Consensus on Time in Range, and discuss practical insights into barriers and facilitators to implementation in real‐world medical practices. Finally, they review emerging evidence of the benefits and potential of remote management in the setting of the COVID‐19 pandemic.
Results
This is an overview of TIR management goals for individuals with T1D, T2D, and T1D in pregnancy, and can serve as a reference “best practice guide” for the use of CGM‐based metrics in managing diabetes in diverse settings, including primary care settings.
Conclusions
Optimization of glycemic management using TIR metrics based on international consensus recommendations allows a practical and actionable alternative to face‐to‐face and HbA1c‐based management that has broad applicability during the global COVID‐19 pandemic and beyond.
Comment
The aim of the authors is to provide a “best practice” guide to the use of TIR and CGM metrics in the management of individuals with diabetes during the COVID‐19 pandemic. This review goes well beyond that objective, however, in providing a comprehensive and understandable overview of the use of CGM metrics to optimize glycemic management in diverse settings; it is an excellent overview of the use of TIR to optimize diabetes management both for remote care and face‐to‐face care. Beyond the COVID‐19 pandemic, TIR‐based management has potential to improve the precision of diabetes care and decrease the clinical inertia, and may be a key component in helping primary care move beyond stalled progress in improving glycemic metrics in everyday medical practice, especially for individuals on insulin. This article should be required reading for primary care clinicians well beyond the UK medical system.
Leveraging Advances in Diabetes Technologies in Primary Care: A Narrative Review
Bode B1, King A2, Russell‐Jones D3, Billings LK4
1Atlanta Diabetes Associates; Atlanta, GA; 2HealthTexas at Stone Oak, San Antonio, TX; 3Royal Surrey County Hospital, Guildford, UK; 4NorthShore University HealthSystem/University of Chicago Pritzker School of Medicine, Skokie, IL
Background
Primary care providers play a key role in the care of individuals with T2D. Advances in diabetes technology can help in personalizing care and addressing individual needs.
Methods
This article reviews available diabetes technologies with applicability to primary care management of diabetes, dividing them into two general categories, devices for glycemic monitoring and insulin delivery systems. Glucose monitoring systems, including self‐monitoring blood glucose devices (SMBG), which measure by fingerstick blood sample, and continuous glucose monitoring devices, which monitor interstitial glucose and provide real‐time data, including the pros and cons of both technologies, are discussed. Glycemic metrics based on CGM data are also reviewed. Insulin delivery devices beyond traditional syringe‐based therapy are discussed at length. These include insulin pens, which are currently widely available, and connected pens that assist in calculating and delivering doses, which are becoming increasingly available, as well as a variety of insulin pumps. Finally, software and applications to monitor and manage glycemic data are discussed.
Results
Continuous glucose monitoring technology allows review of glycemic metrics including time in range, and studies show that real‐time CGM can improve glucose management for individuals with T1D, and T2D on multiple daily dose insulin, more than SMBG. Insulin pens have improved the convenience of insulin delivery over traditional injections for individuals using insulin to manage their diabetes, and connected pens can help in calculating dosing and capturing data on dosing to facilitate optimization of mealtime insulin use. Insulin pumps allow greater precision in insulin dosing, at the cost of increasing complexity and increased expense.
Conclusions
Diabetes technology can help patients improve glycemic management and decrease disease burden. Advances in technology have made promising diabetes technologies more widely available for use in primary care, and in individuals managing T2D. A guiding principal in the use of diabetes technology is that technology should be individualized based on patient parameters and needs, desires, and device availability.
Comment
Diabetes technology beyond fingerstick blood glucose monitors and insulin pens is relatively new to many primary care clinicians, yet has potential to improve glycemic management and decrease burden for many with diabetes managed in primary care, including the much larger population of individuals with T2D who are predominantly managed in primary care settings. This article is an overview of currently available CGM technology, as well as connected pens and insulin pumps, outlining advantages and disadvantages of available devices. It is an excellent reference for primary care clinicians as they consider diabetes technology options and work with patients to choose technology that balances cost and burden versus benefit, allowing individualization of technology choice in managing diabetes in primary care. Key components of maximizing the benefit of emerging diabetes technologies include both making primary care aware of the technologies and creating the systems to optimize the use of the technologies in primary care, and this article can serve as important first step in increasing awareness of diabetes technologies among primary care clinicians.
Practical Considerations for Initiating and Utilizing Flash Continuous Glucose Monitoring in Clinical Practice
Wysham CH1, Kruger DF2
1Rockwood Clinic/MultiCare Health System, University of Washington, Spokane, WA; 2Division of Endocrinology, Diabetes and Bone & Mineral, Henry Ford Health System, Detroit, MI
Background
Use of continuous glucose monitoring (CGM) in patients with type 1 and type 2 diabetes has been shown to improve overall glucose management, especially in those managed intensively with multiple daily injections of insulin or insulin pump. There are currently three types of CGM systems on the market including real‐time CGM, flash CGM (also called intermittently scanned CGM), and professional CGM. This article reviews practical approaches and strategies to integrate the most recent intermittently scanned flash CGM system called FreeStyle Libre 2 (FSL2) into clinical practice.
Methods
The authors reviewed current research and evidence‐based guidelines to make recommendations on the patient selection, education/training, interpretation, coding, and documentation related to FSL2 use. A case study application was used to reinforce key concepts and strategies for successful integration of this new technology into practice.
Results
Patients that would benefit from the FSL2 system include the following:
1. Patients treated with intensive insulin regimens.
2. Patients with type 2 diabetes not on intensive insulin regimens as an alternative to self‐monitored blood glucose.
3. Newly diagnosed patients with type 2 diabetes for educational purposes.
4. Patients at increased risk for hypoglycemia.
5. Pregnant patients with any type of diabetes (note, CGM use is not currently approved for use during pregnancy in the United States, but is approved in the UK and other select countries).
6. Patients with financial constraints that limit real‐time CGM systems, yet desire improved glycemic management.
Patient education is critical when starting FSL2 and should include guidance on proper sensor placement, optimal scanning “flash” frequency, use of trend arrows and alerts, guidance on interpreting glucose data, how to respond to hypo‐ and hyperglycemia, and when fingerstick testing is required for times when symptoms do not match the sensor glucose reading (6). Patients should also be instructed how to set up their Freestyle LibreView account so that they can upload their glucose data and review reports such as the FSL2 Summary Report that has been adapted from the Ambulatory Glucose Profile (AGP) Report (7). The LibreView account will also allow the patient to share their CGM data with their diabetes care team.
The interpretation of CGM data is based on an international consensus statement to bring uniformity to CGM‐based data metrics and targets (8). Ten metrics were identified that should be reported, with the most important being mean glucose, glucose management indicator (GMI), glycemic variability, time in range (TIR), time below range (TBR), and time above range (TAR). A four‐step process was provided to guide the interpretation of the Freestyle LibreView Summary Report.
Coding and documentation are critical for appropriate reimbursement for the CGM‐based care and education provided. Current CPT codes for CGM billing include 95249 for patient‐owned sensor placement, hook up, calibration, training, and report generation. CPT code 95250 is used for clinic‐owned professional CGM. CPT code 95251 is used for CGM interpretation. All codes must be based on minimum of 72 h of glucose data. CPT code 95251 applies to patient‐ and clinic‐owned CGM devices.
Conclusions
Successful integration of CGM into clinical practice requires planning and clinic workflows that clearly delineate the roles and responsibilities of each clinic staff member in providing education on the use of the technology, data downloading and management, and purposeful interpretation the glucose data.
Comment
This article provides practical strategies and guidance for the successful integration of CGM technology into clinical practice that can be applied not only to FSL2 but to other CGM systems (e.g., Dexcom and Medtronic) as well. It describes a very practical four‐step approach for the interpretation of AGP reports. However, primary care clinicians may need additional decision support to guide therapy recommendations. Advancements in machine learning and artificial intelligence, or other methods of guidance, will need to be harnessed to provide decision support for primary care, especially in the area of insulin initiation and titration. In addition, seamless integration of discreet CGM metric data and glucose summary reports like the AGP into the electronic health record (EHR) will be critical for expansion of CGM technology into primary care and will be necessary for it to become an effective way to track diabetes quality and population health.
CONNECTED CARE AND CARE MODEL INNOVATION
The Digital/Virtual Diabetes Clinic: The Future Is Now—Recommendations from an International Panel on Diabetes Digital Technologies Introduction
Phillip M1,2, Bergenstal RM3, Close KL4, Danne T5, Garg SK6, Heinemann L7, Hirsch IB8, Kovatchev BP9, Laffel LM10, Mohan V11, Parkin CG12, Battelino T13
1The Jesse Z and Sara Lea Shafer Institute for Endocrinology and Diabetes, National Center for Childhood Diabetes, Schneider Children's Medical Center of Israel, Petah Tikva, Israel; 2Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel; 3International Diabetes Center at Park Nicollet, Health Partners, Minneapolis, MN; 4Close Concerns and diaTribe, San Francisco, CA; 5Diabetes Centre for Children and Adolescents, AUF DER BULT, Kinder‐und Jugendkrankenhaus, Hannover, Germany; 6University of Colorado Denver and Barbara Davis Center for Diabetes, Aurora, CO; 7Science Consulting in Diabetes, Neuss, Germany; 8Division of Metabolism, Endocrinology, & Nutrition, Department of Medicine, University of Washington School of Medicine, Seattle, WA; 9Center for Diabetes Technology, University of Virginia, Charlottesville, VA; 10Pediatric, Adolescent and Young Adult Section and Section on Clinical, Behavioral and Outcomes Research, Joslin Diabetes Center, Harvard Medical School, Boston, MA; 11Dr. Mohan's Diabetes Specialties Centre & Madras Diabetes Research Foundation, Chennai, India; 12CGParkin Communications, Inc., Henderson, NV; 13Department of Pediatric Endocrinology, Diabetes and Metabolism, University Medical Centre‐University Children's Hospital, and Faculty of Medicine, University of Ljubljana, Ljubljana, Slovenia
Background
Medical care has been slow to adopt the digital and cloud‐based revolution that is so prevalent in other businesses. The electronic health record has certainly become a core feature of clinical practice, but integrating digital technology like CGM and developing virtual care models for disease states like diabetes was slow to progress in early 2020. Yet a broad group of diabetes experts convened a consensus conference to summarize the current literature and project what would be needed and valuable in the future regarding digital or virtual diabetes care.
Methods
In February of 2020 an international panel of healthcare providers (HCP), researchers, patient advocates, and industry representatives was convened to review the status of digital diabetes technologies, characterize deficits in current technologies, and identify issues for consideration.
Results
An expert panel laid out the challenges and potential solutions for incorporating telehealth or digital diabetes technologies into the future of diabetes care. The panel concluded that many of the components needed for an effective virtual or digital diabetes clinic were in the early stages of development, but continued work on refining each component and then integrating them into a connected care system was needed.
Conclusions
The Advanced Technologies & Treatments for Diabetes (ATTD) Consensus Panel put forward a roadmap (figure below) for many elements that needed to be integrated into a virtual or digital diabetes care clinic. Over the course of completing this manuscript, with the COVID‐19 pandemic in full force, many of the elements of virtual care suggested and predicted by the consensus panel were implemented in rapid succession to meet the needs for remote or virtual monitoring and care for people with diabetes.

Change in acute diabetes events and all-cause hospitalizations at 0, 45, 90, 135, and 180 days after CGM initiation (figure used with permission).

Conceptualized clinical data flow in Digital/Virtual Diabetes Clinic model (figure used with permission).
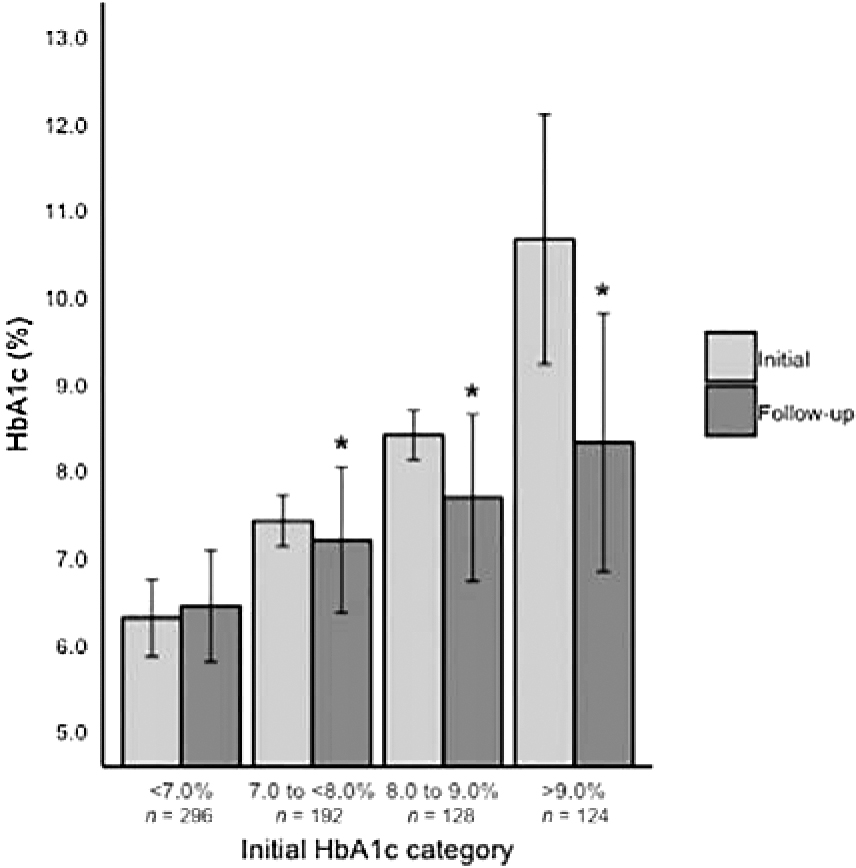
Change in HbA1c from initial measurement to follow-up stratified by initial HbA1c range (figure used with permission).
Comment
There could not have been a timelier article addressing the potential future of diabetes care than the prescient ATTD Consensus on the need for a virtual or digital diabetes care model. The central roles of diabetes monitoring devices, Smartphone technology, EHR integration, standardized digital data reporting, and patient/clinician communication (shared decision making) were all highlighted as in need of further development and somehow being seamlessly connected. The pandemic moved major components of the virtual clinic model forward with warp speed, in particular diabetes visits performed via telehealth. While we now realize there are major refinements and additional innovations needed in each component on the virtual care roadmap, we know there is no turning back on this being a major part of diabetes surveillance, support, and management in the future.
A Virtual Type 2 Diabetes Clinic Using Continuous Glucose Monitoring and Endocrinology Visits
Dixon RF1, Zisser H2, Layne JE1, Barleen NA1, Miller DP2, Moloney DP1, Majithia AR3, Gabbay RA4, Riff J1
1Onduo LLC, Newton, MA; 2Verily Life Sciences, South San Francisco, CA; 3School of Medicine, University of California San Diego, La Jolla, CA; 4Joslin Diabetes Center, Harvard Medical School, Boston, MA
Background
Data is accumulating on the ability of CGM to improve glucose management in individuals with T1D and T2D in observational or randomized clinical trials. But studies evaluating new models of clinical care centered around cloud‐based CGM technology as part of a connected care ecosystem are needed.
Methods
The Onduo Virtual Diabetes Clinic (VDC) was established around a telehealth virtual care model for adults with T2D and included connected devices (BGM, CGM, weight scales), remote lifestyle coaching, and a mobile app for added clinical support. There were video consults with an endocrinologist and use of real‐time CGM for those deemed in need of this technology.
Results
Early data on 740 participants showed a significant improvement in HbA1c at 6 months. HbA1c decreased by 2.3%±1.9%, 0.7%±1.0%, and 0.2%±0.8% across baseline categories of >9.0%, 8.0% to 9.0% and 7.0% to <8.0%, respectively (all P<0.001).
Conclusions
A virtual diabetes clinic model for the management and support of individuals with T2D showed improvement in HbA1c (particularly in those with high baseline HbA1c values) and deserves further study and refinement.
Comment
As clinical trials show benefit from the use of CGM, work now needs to proceed on ways to implement effective and efficient use of CGM and other connected care devices to manage adults with T2D. This early evaluation of one such virtual diabetes clinic are very promising because those with the highest HbA1c values improved the most while using these coaching and CGM support tools. More data are needed to see if these gains are sustainable and cost‐effective. In addition, we look forward to detailed learning on which coaching tools were most effective and how to best communicate using CGM data and reports in a virtual connected care environment.
Continuous Glucose Monitoring for Underserved and Minority Patients with Type 2 Diabetes in an Interprofessional Internal Medicine Clinic
Bui A1, Kim J1,2
1University of North Carolina Eshelman School of Pharmacy, Chapel Hill, NC; 2Moses Cone Internal Medicine Clinic, Cone Health, Greensboro, NC
Background
Use of continuous glucose monitoring (CGM) in patients with diabetes has been shown to improve overall glucose management by lowering glycosylated HbA1c and reducing the risk for hypoglycemia. This study explored if CGM used in an internal medicine clinic providing care for an underserved and primarily minority patient population with type 2 diabetes would result in improved glucose management. The interprofessional team consisted of pharmacists, dieticians, and physicians working in close collaboration.
Methods
A retrospective quasi‐experimental study was conducted between August 2018 and August 2019 at an internal medicine residency clinic using an interprofessional team to manage patients with diabetes. Inclusion criteria included patients with type 2 diabetes age 18 years and older with an indication for CGM based on clinical judgment of the interprofessional team. Indication for CGM included hypoglycemia, hyperglycemia, and/or glycemic variability. Study participants must have participated in the clinic's CGM service and have at least 10 consecutive days of CGM data available for analysis. Exclusion criteria included patients who were pregnant or those who missed one or more CGM service clinic appointments. The CGM service included three appointments spaced 1 week apart. The CGM sensor was placed at the first appointment and the patient returned at weeks 2 and 3 for CGM data download, analysis, interpretation, and therapy recommendations made by the pharmacist and/or dieticians in collaboration with the patient's attending or resident physician.
Results
Fifty‐five patients met the inclusion criteria and were included in the analysis. They had mean age of 61+11.2 years, 44% were male, and 78% were African American. CGM‐derived average blood glucose decreased significantly nearly 18 mg/dL from 208.4 mg/dL at week 1 to 190.7 mg/dL at week 2 (P=0.0281). Time in range (70–180 mg/dL) increased from 45.2 to 51.4% (P=0.0038), time above range (>180 mg/dL) decreased from 49.8 to 44.3% (P=0.0168), and time below range (<70 mg/dL) showed a non‐significant increase from 3.0% to 5.0%. The most common interventions were increasing medication dose and education regarding lifestyle or medications that each occurred in 24% of patients at week 1 and in 28% and 36% of patients at weeks 2 and 3, respectively. Medication dose was decreased or stopped in 30.3% of patients at week 1 and in 13.8% of patients at week 2. The majority of 66 interventions made at week 1 were made by the attending or resident physician (56%), followed by the pharmacy team (33%) and 11% by the dietician team. The breakdown of interventions by team member was similar at week 2.
Conclusions
The present study demonstrated that an interprofessional CGM service consisting of pharmacists, dieticians, and physicians working collaboratively is associated with increased time in range, lower time above range, and without significant increase in time below range. CGM provided personalized glucose data allowing medication and lifestyle interventions within a 2‐week period.
Comment
This small study has important implications for primary care, especially those who provide care in underserved communities where the social determinants of health play such an important role in preventing optimal chronic disease management. The study demonstrated the power of the interprofessional team, especially the value of engaging the pharmacist and dietician to work closely with the attending physician to make therapeutic and lifestyle interventions. One interesting finding is how 1 week of CGM data leads to intensification of therapy (increased dose or added medication) as well as de‐escalation of therapy, presumably to prevent hypoglycemia. Even with a rather short intervention period of 2 weeks, it shows that clinically significant improvement in glucose management can be achieved. It also provides a model to successfully implement CGM technology and support underserved communities by providing support for the initiation of CGM as well as rapid follow‐up to make therapeutic and lifestyle changes. The short duration of the study precluded the determination of the impact of having patients use CGM for a longer period of time, but it is not unreasonable to expect even greater improvement of glucose management with extended follow‐up.
Footnotes
Author Disclosure Statement
Dr. Gregg Simonson serves on the scientific advisory board for Merck and has received educational grants from Sanofi and Abbott. Dr. Simonson's employer, nonprofit HealthPartners Institute, contracts for his services and he receives no personal income for these services.
Dr. Thomas W. Martens has received research support, has acted as a consultant, or has been on the scientific advisory board for Abbott Diabetes Care, Dexcom, Lilly, Novo Nordisk, Medtronic, Insulet and Medscape. Dr. Martens's employer, nonprofit HealthPartners Institute, contracts for his services, and he receives no personal income for these services.
Anders L. Carlson is a medical director at DocSquad, part of Bright Health Group's integrated care delivery organization. Through the International Diabetes Center at HealthPartners, he receives research and/or consulting support from Medtronic, Insulet, Dexcom, Sanofi, Eli Lilly, Abbott, UnitedHealth, Mannkind, and Novo Nordisk. No personal income from any of these services goes to Dr. Carlson.
Dr. Richard M. Bergenstal has received research support, has acted as a consultant, or has been on the scientific advisory board for Abbott Diabetes Care, Ascensia, Bigfoot Biomedical, CeQur, DexCom, Eli Lilly, Hygieia, Insulet, Medtronic, Novo Nordisk, Onduo, Sanofi, and United Healthcare. Dr. Bergenstal's employer, nonprofit HealthPartners Institute, contracts for his services and he receives no personal income for these services.