
Abstract
Studies that investigate use of diabetes technologies such as blood glucose monitoring (BGM) and continuous glucose monitoring (CGM) often report contradictory findings regarding efficacy and clinical utility. Whereas some studies of a given technology have shown no benefit, others have reported significant benefits. These incongruities derive from how the technology is viewed. Is it viewed as a tool, or is it an intervention? In this article, we discuss earlier studies that illustrate the contrast between use of BGM as a tool versus use as an intervention, compare and contrast the roles of BGM and CGM as tools and/or interventions in diabetes management, and suggest that CGM can function effectively as both.
Introduction
From early years of blood glucose meters, there has been tremendous progress in home glucose monitoring system technology, especially with the recent development of continuous glucose monitoring (CGM). However, the role of subsequent diabetes technologies such as CGM has been ambiguous at best. Are diabetes technologies tools or interventions, or both? For the purposes of this discussion, we define tool as a device, medication, or measure that can be used to accomplish a specific task. An intervention comprises an action or approach initiated to treat a disease, prevent harm, or improve overall health.
Although efforts to differentiate tools from interventions may seem trivial, failure to understand this distinction can lead to erroneous conclusions in influential research. In this article, we review earlier studies that illustrate the contrast between use of blood glucose monitoring (BGM) as a tool versus use as an intervention, compare and contrast the roles of BGM and CGM as tools and/or interventions in diabetes management, and propose that CGM has the ability to function effectively as both.
Earlier BGM Studies
DiGem trial
Tools have often been used or misused as interventions. A tool in the absence of an action or approach is not an intervention. One such example is the DiGem Trial where the use of a tool BGM was considered an intervention. 1 This led to a conclusion that negatively impacted the future use of BGM in managing type 2 diabetes (T2D). The objective of the study was to determine whether BGM (alone or in conjunction with instruction in self-care behaviors) is more effective than usual care (no BGM) in improving glycemic control in non-insulin treated patients with T2D.
Patients in the BGM groups were instructed to perform three blood glucose tests per day, one after fasting, and the other two before meals or 2 h after meals, 2 days per week. They were followed primarily by nurses who managed patient care based on BGM data who could not make any medication changes—all medication changes were made by a general practitioner based on quarterly HbA1c changes. 2 At study end, investigators observed no significant difference in HbA1c between the usual care and the BGM groups. Based on these findings and subsequent cost analyses, 3 the U.K. National Health Service continues to deny coverage for BGM in T2D patients treated with noninsulin therapies unless a physician states a legitimate reason for a specific patient. 4
Although results from the DiGem trial are often cited as definitive proof that BGM is not useful in noninsulin treated T2D, 5,6 a key limitation not discussed in the report was the study design, which raised questions about the validity of the conclusions. 7,8 First, the prescribed testing regimen provided little or no information about the occurrence or magnitude of daily glycemic excursions if patients only tested before meals.
Thus, the attending nurses were severely limited in their ability to counsel patients and make changes in their lifestyle behaviors (i.e., no action or approach). More importantly, physicians were only notified when BGM data indicated that glucose levels were consistently >270 mg/dL. Thus, it is conceivable that no therapeutic changes were made even in the presence of level 2 hyperglycemia (>250 mg/dL), which is well above established glucose targets. Based on these limitations, reliance on HbA1c levels for all therapy decisions likely negated any potential advantages gained through BGM.
STeP study
The STeP study (Structured Testing Program) evaluated the usefulness of BGM as an integral component of a comprehensive intervention that included obtaining and documenting glucose data in a structured format, patient–clinician collaboration in interpreting the data, and shared decision making in adjusting therapy (medication, lifestyle, or both). 9 In the study, all patients were provided a blood glucose meter and test strips at the baseline visit. Patients randomized to the structured testing group (STG) used a paper tool to record and plot a 7-point BGM profile (fasting, preprandial/2-h postprandial at each meal, bedtime) on 3 consecutive days before each quarterly visit. An example of a completed form is shown in Figure 1.

ACCU-CHEK® 360° View blood glucose analysis tool.
STG physicians and staff received training on interpreting the BGM data provided and were provided with an algorithm that listed various pharmacological/lifestyle treatment strategies that could be utilized in response to the specific glycemic patterns they identified. Patients received training in filling out the form, interpreting their data, and making lifestyle changes in response to problematic glycemic patterns. They were asked to document meal sizes and energy level and to comment on their BGM experiences on the tool.
Patients randomized to the active control group (ACG) were instructed to use their glucose meter after their physicians' recommendations but received no additional training, or instruction. At 12 months, a significantly greater HbA1c reduction in adherent STG patients was observed compared with adherent ACG patients (−1.3 vs. −0.8, P < 0.003). Use of the tool led to earlier, more frequent, and more effective treatment change compared with the control group.
Key differences between the studies
In contrast to the DiGem trial in which the BGM data were underutilized, and all medication changes were based on HbA1c, the STeP study utilized a tool that presented the glucose data in a graphical format. Although HbA1c testing was useful in assessing average glucose levels between study visits, the glucose profiles generated through structured testing appeared to be more relevant to therapeutic decision making by facilitating rapid identification of problematic glycemic patterns and prompting timely therapy changes. For patients, use of the tool helped them better understand the “cause and effect” of their medications and prompted them to respond to problematic glycemia with appropriate behavior changes when needed.
Whereas the DiGem trial simply looked at the impact of increasing BGM frequency but with no specified preprandial/postprandial testing and few (if any) medication changes based on the data, the STeP study clearly demonstrated the value of BGM when incorporated into a comprehensive regimen that utilized structured glucose data in combination with patient–clinician collaboration and shared decision making. This approach improved clinical outcomes by engaging both patients and their clinicians.
To summarize, based on the studies already discussed, when BGM is unstructured, it is simply a tool for measuring glucose and accomplishes very little. However, BGM, as a tool, facilitates an intervention when the data are structured, presented graphically, prompts patients to modify lifestyle and medication adherence behaviors, and discusses in collaborative patient–clinician interactions to make treatment decisions. Interestingly, a recent study by Bergenstal et al. found no differences in HbA1c or percentage of time in range (%TIR) between structured BGM and CGM in T2D patients. 10 The only difference was less hypoglycemia in the CGM group.
Limitations of BGM
Although structured BGM has proven its value, unstructured and/or infrequent BGM has significant limitations that are inherent to the technology. For example, BGM only provides a single “point-in-time” measurement with no indication of the direction or velocity of changing glucose levels. Users must test frequently to obtain these data, which seldom occur unless the initial measurement indicates an acute hypoglycemic or hyperglycemic event. Without frequent testing, users cannot see the “cause and effect” of their medications and lifestyle behaviors, which can impact adherence to their prescribed regimens. 11 More importantly, they may fail to detect potentially life-threatening situations such as hypoglycemia as shown in Figure 2.

Infrequent BGM can fail to detect extreme glucose excursions. BGM, blood glucose monitoring.
When BGM was first introduced, clinicians had to leaf through logbooks that often contained erroneous, illegible, and/or incomplete glucose data, and patients often forget to bring their glucose records to clinic visits. 12 –14 Although today's “memory” meters have mostly addressed the ability to obtain accurate data and display it in easy-to-interpret formats through download software, the information is not actionable unless patients are testing frequently. In addition, many primary care practices are not set up for downloading meters.
Another limitation of BGM is the additional burden it places on patients, leading to poor adherence to recommended testing frequency. An earlier survey of 16,061 T1D patients who participate in the T1D Exchange registry found that 34% performed BGM three times daily. 15 Another survey reported nonadherence to recommended BGM frequency for T1D patients to be as high as 60%. 16
In a Swedish survey-based cross-sectional study of 314 T1D adults, Moström et al. found that only 43.9% of respondents performed BGM ≥4 times per day, despite glucose meters and testing supplies being available at no cost. 17 The most common reasons for infrequent testing reported by respondents were “not remembering” (53%), “lack of time” (51%), “self-consciousness” (21%), and “pain/discomfort” (14%).
Puckrein et al. recently reported findings from a 12-month retrospective analysis that assessed glucose monitoring adherence in Medicare beneficiaries who were treated with intensive insulin regimens. 18 Investigators found that 38.14% of beneficiaries were nonadherent to their prescribed glucose monitoring and 35.42% had no record of obtaining glucose monitoring supplies. In an earlier study, Siddiqui et al. found that 61.9% of 33 T2D adults who were treated with antihyperglycemic oral medications reported that they did not use BGM in their daily regimen. 19
CGM: The Next Generation of Structured Testing
How CGM functions as both tool and intervention
Unlike BGM, CGM does not require users to interrupt their daily activities to obtain and view their glucose data. Functioning as tools, the most current CGM systems provide immediate feedback to users by automatically transmitting a constant stream of data to a handheld reader or smartphone that displays the current glucose value, the recent glucose trend, and the direction and rate of changing glucose through trend arrows (Fig. 3). When the sensor detects immediate or impending glycemic events, audible alerts are triggered automatically, warning users to address or avoid these events.

Current CGM systems automatically calculate and display recent glucose trends (A) and trend arrows (B) indicating the direction and velocity of changing glucose. CGM, continuous glucose monitoring.
Functioning as an intervention, CGM organizes, summarizes, and analyzes a large stream of glucose data and provides clinicians with accurate, complete, and actionable information in formats that can be interpreted quickly and easily. With CGM, users can link their devices to a smartphone app that automatically transfers the data to their clinician for review using download software. However, physicians will still need to establish workflow protocols to manage data downloading. Although all CGM companies offer their own software, many include a page that features a modified version of the Ambulatory Glucose Profile (AGP), which was developed by the International Diabetes Center (Minneapolis, MN). 20
The AGP report is an internationally recognized standard for displaying and interpreting CGM data in a format that allows clinicians and patients to quickly identify patterns and trends in daily glucose control. 21 –24 Utilizing the clinical targets for assessment of CGM data established in 2020, 24 the report displays data in numerical and graphical formats. The AGP report from the LibreView software (Abbott Diabetes Care, Alameda, CA) is an example of the data provided in the AGP (Fig. 4).
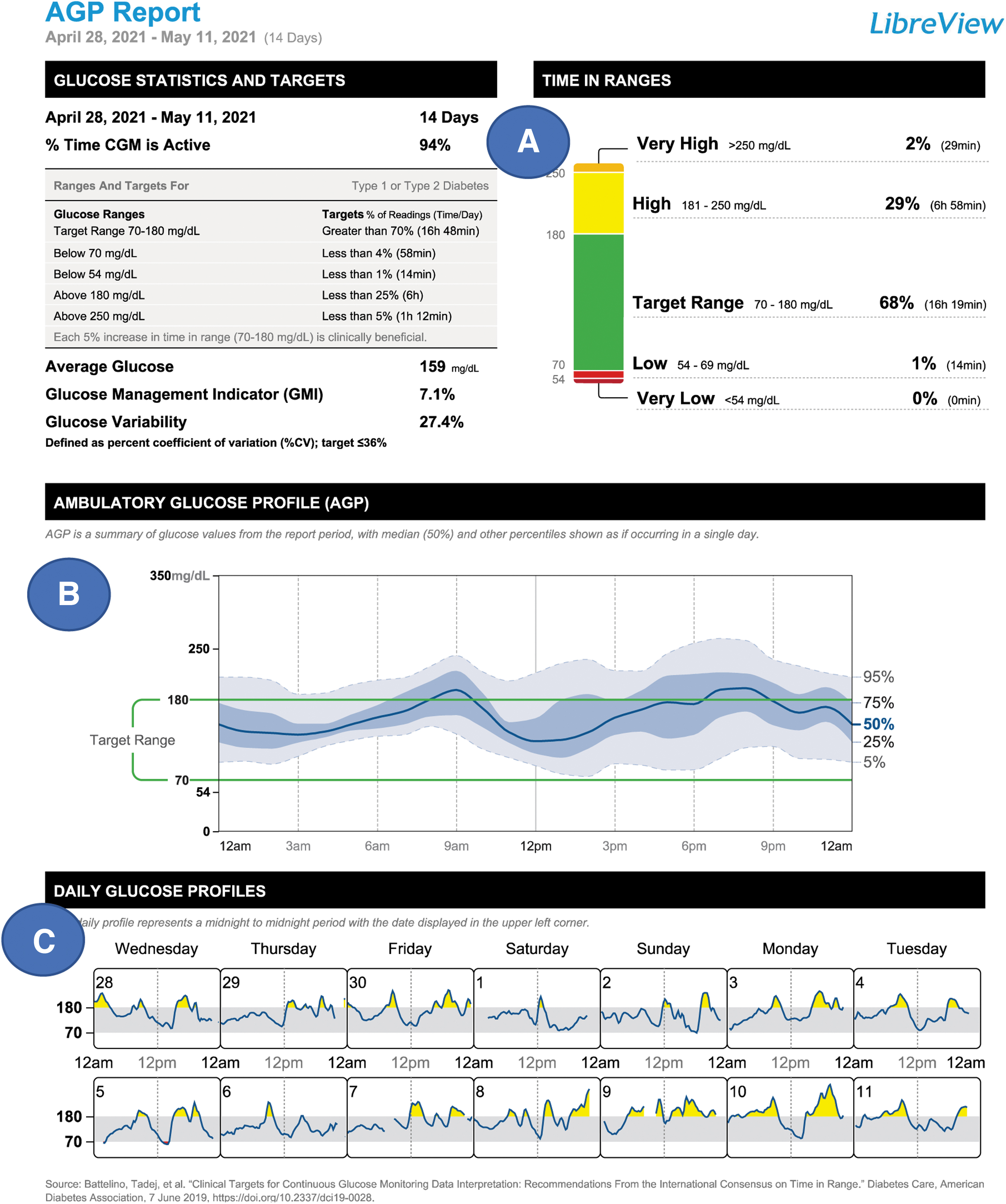
LibreView AGP Report. AGP, Ambulatory Glucose Profile.
The statistics section (Fig. 4A) presents each patient's percentage of CGM usage, average glucose, glycemic variability (reported as the percentage of coefficient of variation [%CV]), and the glucose management indicator, which is an estimate of HbA1c from mean glucose over the sensor wear period. The percentage goals for %TIR, %TBR, and %TAR are also provided, with a graphic depiction and statistics for the patient are presented on the right. The AGP (Fig. 4B) combines daily profiles to create a 1-day (24-h Modal Day) graphic.
The dark blue line indicates the median glucose level at all day parts. The light blue and gray areas depict the degree of glycemic variability. The profile enables clinicians and patients to quickly identify the time(s) of day when glucose is most problematic. The daily glucose profiles (Fig. 4C) allow for further analysis of each day covered in the data set.
Use of the AGP report and other software reports creates valuable opportunities for patients and clinicians to collaborate, in-clinic or remotely using telehealth technology, prompts more timely and targeted therapy and individualized care, and it helps patients better understand the effects of medications and lifestyle behaviors on their glycemic control. When combined into an overall approach to diabetes management, the demonstrated result is improved clinical outcomes and quality of life.
Efficacy of CGM in all diabetes populations
Over the past several years, numerous clinical trials and real-world observational studies have demonstrated the safety and efficacy of CGM use in individuals treated with intensive insulin therapy. 25 –34 More recently, an increasing number of studies have demonstrated similar glycemic benefits among individuals treated with basal insulin only and noninsulin therapies. 35 –44
Martens et al. studied 175 T2D adults treated with basal insulin with/without noninsulin medications assessing the use of CGM versus BGM on glycemic outcomes for 8 months. 40 Mean HbA1c decreased 1.1% from baseline with CGM used compared with a 0.5% reduction in the BGM group (P = 0.02), with significant increases in the percentage of time spent in glucose range (%TIR) and decreases in time below range (%TBR) and above range (%TAR). Moreover, the HbA1c improvements were observed across the age range of 33–79 years. Wright et al. recently reported significant HbA1c reductions (from 10.1% to 8.6%, P < 0.001) in a large retrospective database analysis of 1034 adults with nonintensively treated T2D adults. 39
Significant glycemic improvements have also been reported in similar U.S. and Canadian retrospective studies. 41,42 In a 6-month prospective interventional single-arm study of CGM use in 38 T2D adults (58% treated with noninsulin medications), the mean HbA1c level decreased from 10.1% at baseline to 7.3% at study end (P < 0.001), with significant increases in %TIR (P < 0.001) and significant reductions in body weight (P = 0.002). 43 Regardless of these findings, CGM coverage for individuals treated with less intensive therapies currently remains extremely limited (among commercial insurers and nonexistent for Medicaid beneficiaries).
Constructivism/Social Constructivism: A Theoretical Basis
Although it is easy to accept the view of CGM as a tool, the concept of CGM as an intervention is more difficult to grasp without an understanding of two relevant and related learning theories, constructivism and social constructivism, which were originally formulated in the study of child development and learning, 45,46 but have since been applied in the education of health care professionals. 47,48 As described by Piaget, constructivism posits that individuals construct new knowledge through interactions between their prior knowledge and experiences and that new knowledge and experiences they gain from interactions with others. 45
In other words, rather than passively receiving knowledge from others (e.g., written, didactic), real knowledge is constructed based on past knowledge and experiences. Piaget further proposed that there is a circular relationship between a stimulus that causes a cognitive or behavioral response, and how that response affects the way the next stimulus is perceived. Vygotsky expanded this concept as the basis for social constructivism, which emphasizes the role of collaboration with others in the learning process. 46
Assuming the validity of these theories, it is reasonable to consider that the act of placing a CGM device in a patient's hands becomes an intervention because it provides data through continuous feedback (stimulus) that prompts a response (cognitive or behavioral)—even without prior training in interpreting and acting upon CGM data—and likely affects how the patient responds to his/her next view of the data. For example, in a recent study of 35 adults with newly diagnosed T2D, Polonsky et al. observed significant changes in glycemic control and reported behaviors after the first few weeks of unblinded CGM use compared with 2 weeks of blinded CGM use at baseline. 44
Other than instruction on how to place their sensors and set up their devices, participants received no training in data interpretation before unblinded CGM use. In essence, wearing a sensor prompted participants to modify their behaviors to improve their glycemic control. Over the 8-week intervention period, participants attended five weekly virtual group sessions in which they shared their experience using CGM and asked questions but were encouraged to conduct weekly “personal experiments” to answer their questions themselves. At study end, investigators observed a significant increase in %TIR with a corresponding decrease in %TAR (both P = 0.01) and an overall rise in well-being (P = 0.04). Participants also reported improvements in healthy eating (P < 0.001).
Although the mentioned study illustrates how CGM functions as both a tool and an intervention, it is important to note that the efficacy of the intervention is affected by four key determinants (Table 1). The presence of one or more negative conditions will likely result in patient frustration, leading to discontinuation of CGM use and poor outcomes until the condition is addressed and resolved.
Determinants of Continuous Glucose Monitoring Intervention Efficacy
Summary
Trying to determine whether CGM is a tool, an intervention, or both may seem trivial. However, when narrowly viewed and assessed as a simple tool, there is a strong probability that the true utility of CGM or other diabetes technologies may be missed. As demonstrated in the DiGem trial, 1 failure to utilize BGM data in a clinically meaningful way showed no significant benefit. Results from the DiGem trial and similarly designed studies provided strong support for the NHS in denying BGM coverage for noninsulin-treated T2D patients.
Although the STeP study showed significant benefits in improving glycemic outcomes and prompting more timely and frequent therapy adjustments in noninsulin-treated patients, 9 many public and private insurers continue to view BGM as tool for adjusting insulin, not as an intervention that prompts both patients and clinicians to make adjustments in medications and lifestyle behaviors. As such, coverage is often limited to one test strip per day.
Unfortunately, despite a growing body of evidence demonstrating the benefits of CGM in T2D patients treated with nonintensive therapies, 35 –44 coverage for noninsulin-treated T2D is restricted or denied. Although reductions in severe hypoglycemia is a key benefit of CGM in intensively treated diabetes, coverage restrictions on individuals who are not treated with intensive insulin regimens ignore the science, which has clearly shown that chronic hyperglycemia leads to the development of myriad macrovascular and microvascular complications, leading premature mortality and significant health care costs regardless of type of diabetes or treatment regimen.
There is also evidence that excessive glycemic variability is strongly associated with the development of retinopathy and albuminuria in adults with T2D. 49
CGM is clearly a tool when viewed as a method for measuring glucose. However, as discussed here, it is also an intervention in the broadest sense because it organizes glucose data into actionable information that prompts actions that avoid harm and improve health. However, the benefits of CGM as an intervention are demonstrated when patients have the requisite knowledge to interpret their information, the motivation to take necessary action based on their data, the confidence in themselves to take the appropriate action, and support from their health care team.
Footnotes
Authors' Contribution
E.E.W. and S.S. wrote the article. All authors reviewed the article before submission and take full responsibility for the accuracy of its content.
Acknowledgements
The author wishes to thank Christopher G. Parkin, MS, CGParkin Communications, Inc., for editorial support and assistance in developing this manuscript.
Author Disclosure Statement
E.E.W. has received consulting fees from Abbott, Astra Zeneca, Bayer, Boehringer Ingelheim, Eli Lilly, Mannkind, Merck, Sanofi US, and Voluntis and has acted as a speaker for Abbott, Bayer, Boehringer Ingelheim, and Eli Lilly. S.S. reports no financial conflicts.
Funding Information
Funding for the development of this article was provided by Abbott Diabetes Care.