
Abstract
Background and Aims:
Older people with type 2 diabetes (T2DM) on insulin are at increased risk of hypoglycemia and associated morbidity. Management of T2DM in older people must optimize glycemic control, while minimizing risks for hypoglycemia and diabetic ketoacidosis (DKA). In France, the FreeStyle Libre® (FSL) system has been reimbursed since June 2017 for T2DM on intensive insulin therapy. We assessed the impact of starting FSL on hospitalizations for acute diabetes events (ADEs) in people ≥65 years old, with T2DM on intensive insulin therapy.
Materials and Methods:
A retrospective study on the French Système National des Données de Santé (SNDS) claims database was conducted on people ≥65 years old with T2DM, treated with multiple daily injections (MDI) or insulin pump and starting FSL between August 1, 2017, to December 31, 2018. The analysis covered claims data for 12 months before, and up to 24 months after FSL initiation. Hospitalizations for severe hypoglycemia (SH), DKA, comas, and hyperglycemia were identified using ICD-10 codes.
Results:
We identified 38,312 people with T2DM ≥65 years old on intensive insulin therapy initiating FSL during the selection period. Hospitalizations for ADEs were observed in 1.6% of subjects in the 12 months before FSL initiation, compared to 1.05% after 12 months and 0.96% after 24 months, a −34% and −40% reduction, driven by fewer DKA admissions after 12 months and by fewer SH admissions at 24 months.
Conclusions:
These results indicate that FSL can reduce hospitalization for ADEs in this vulnerable older population of adults 65 years of age and older with T2DM on intensive insulin therapy, in whom optimal glycemic control must be achieved, while minimizing risk of hypoglycemia and other ADEs.
Introduction
Flash glucose monitoring using the FreeStyle Libre (FSL) system is associated with significant improvements in glycemic control and outcomes for people living with type 2 diabetes (T2DM), as documented in randomized clinical trials (RCTs) and real-world studies. Although the REPLACE RCT did not show reductions in HbA1c, it did reveal reductions in time below range (TBR) 70 mg/dL 1,2 for users of FSL compared to the control arm using self-monitored blood glucose (SMBG) only.
A separate RCT 3 and two retrospective observational studies 4,5 demonstrated reductions in long-term HbA1c were associated with using FSL in people with T2DM on intensive insulin therapy. Starting FSL is also associated with a reduction in hospital admissions for acute diabetes events (ADEs), such as diabetic ketoacidosis (DKA) or severe hypoglycemia (SH), in people with T2DM. 6 For people with T2DM, the observed reductions in HbA1c and ADEs requiring hospital admissions are sustained for at least 2 years after starting FSL. 7,8
The prevalence of T2DM among the elderly population is significant, with an estimated 25% of people 60 years of age or older being diagnosed with T2DM in the United States, 9 which is almost double the equivalent prevalence in France. 10,11 However, relatively few studies on the use of FSL or real-time continuous glucose monitoring (rtCGM) specifically in the elderly population of people with T2DM are available. One study on people with either T1DM or T2DM, ≥65 years of age, on intensive insulin therapy, found that CGM use was associated with a 0.5% decrease in mean HbA1c, as well as a 68% fall in self-reported episodes of SH. 12
Reductions in moderate-to-SH were also reported for 210 people with diabetes on insulin therapy, ≥65 years of age using CGM, including a small number with T2DM, 13 compared to nonusers, and this was associated with reduced diabetes distress. A subgroup analysis of the DIAMOND study showed that, in adults ≥60 years old with T2DM on intensive insulin therapy, use of rtCGM was associated with improved HbA1c and reduced glycemic variability 14 and that the response of people ≥60 years old with T2DM was not different compared to younger adults ≤44 years old. Bao et al. reported that people with T2DM ≥65 years old on basal insulin therapy were able to improve time in range and reduce hypoglycemia after starting rtCGM, at least as significantly as younger adults. 15
Initiation of basal-insulin therapy in T2DM is associated with a three-fold increase in the relative risk of SH 16 and this increases with the intensification of insulin therapy. 17 It is also evident that the risk of severe or fatal hypoglycemia increases considerably in elderly individuals with diabetes, who are treated with insulinotropic medications, 18 –20 and the risk of falls and fractures among elderly people with T2DM treated with insulin is increased compared to those on oral-only medication. 21,22 Hypoglycemia in elderly people with T2DM is also associated with increased incidence of cardiovascular events, dementia, and death. 22 The association of CGM with reduced fear of hypoglycemia provides a clear rationale for enabling wider access to FSL systems for people with T2DM of all ages, including older people. 23,24
The RELIEF study (Real-world Evidence of FreeStyle Libre: analysis of the Système National des Données de Santé (SNDS) database in France) 6 was conducted using the French national health claims database, the SNDS, 25 which covers the entire French population (∼66 million people) and includes extensive information on all healthcare resource use at an individual level, including outpatient visits, dispensed medication, procedures, chronic conditions, as well as hospital admission diagnoses and procedures, and date of death. The goals of the RELIEF study were to understand the impact of using FSL on ADEs in standard practice in France, following its approval for reimbursement by the National Sickness Fund in June 2017.
The RELIEF study has shown that FSL use is associated with a significant reduction in hospitalization for ADEs in France in the 12 months following starting FSL, including for DKA and SH, both for people with T1DM or T2DM. 6 Among people with T2DM, there was a 39.4% fall in ADEs, driven by a 52.1% reduction in hospitalization for DKA, even in T2DM treated with basal insulin only. 26 These reductions among FSL users with T2DM were maintained at 2 years, with a 48% fall in admissions for ADEs and with a 47% reduction in hospitalizations for DKA. 8
Although definitions may differ, we have adopted those provided by the European Union 27 and reflected in accepted international standards of medical care in diabetes, 28 which define older adults as 65 years of age or more. The aim of this extended analysis of the RELIEF outcomes is to evaluate the impact of using FSL for people ≥65 years old with T2DM on intensive insulin therapy in France, including defined subgroups 65–69, 70–79, and ≥80 years of age. We report on the observed impact for this group of people with T2DM on hospitalization for ADEs in the 24-month period after access to the FSL system, as well as the persistence of older people with T2DM with FSL technology and on changes in the usage of SMBG test strips after starting FSL.
Materials and Methods
Patient selection
The RELIEF longitudinal retrospective cohort study was carried out using data extracted from the national French claims database (SNDS) between January 1, 2015, and December 31, 2019. Patient selection, as well as inclusion and exclusion criteria based diabetes status and FSL usage have been extensively described in previous studies. 6,8
The study reported here identified individuals 65 years of age or older with T2DM at the index date, who were treated with multiple daily injections (MDI) with insulin or continuous subcutaneous insulin infusion (CSII) pumps, with or without oral antihyperglycemic drugs or injectable GLP-1 receptor agonists, who initiated the FSL system during the period between August 1, 2017, and December 31, 2018 (Supplementary Fig. S1).
These criteria mean that the FSL prescription at the index date will be the first-generation sensor, without optional alerts, and which requires the user to scan the sensor with the FSL reader or LibreLink smartphone app to view glucose data and trends. People with T2DM were divided into two cohorts: those who started FSL in 2017 and who had up to 24 months of follow-up to December 31, 2019, and those who had at least 12 months of follow-up after starting FSL. All subjects were considered new users of the FSL system, based on criteria previously described. 6,8 We then analyzed data from these patients over the 12 months before initiation of the FSL system and up to 24 months following initiation (for the 2017 cohort).
Treatment characteristics of people with T2DM before and after initiation of the FSL system
The predicted treatment regimen(s) at FSL initiation and during the 12–24 months afterward were evaluated based on medication reimbursement data in the SNDS in the period August 1, 2017, to December 31, 2019.
Acute diabetes events
Events were identified during the period August 1, 2016 to December 31, 2019 to cover the 12 months before the earliest FSL index date and up to 24 months after the FSL index date. Hospitalizations for DKA were recorded using ICD-10 code E11.1 (T2DM with DKA) as the main or related diagnosis. Hospitalizations for SH were recorded using ICD-10 codes, E16.0 (drug-induced hypoglycemia without coma), E16.1 (other hypoglycemia), E16.2 (hypoglycemia, unspecified), and T38.3 (poisoning by adverse effects of insulin and oral hypoglycemic [antidiabetic] drugs). Hospitalizations for diabetes-related comas were identified with ICD-10 codes E11.0 (T2DM with coma) and E14.0 (Diabetes Unspecified with coma) and hyperglycemia-related stays using ICD-10 code R739 (hyperglycemia, unspecified).
Persistence with the FSL system
Persistence with use of the FSL system was defined between first delivery of a FSL sensor and discontinuation of the FSL system. Discontinuation was assumed when no sensors were delivered to the patient over a consecutive 6-month period. The date of discontinuation was calculated by noting the last recorded date of sensor delivery and then adding on the associated 28-day sensor-wear period for two sensors (i.e., if two sensors were delivered in the last recorded claim, the date of discontinuation was the date of the last claim plus 1 month to take into account that two sensors will last 28 days).
SMBG test strip usage among FSL system users
The impact of FSL on usual blood glucose monitoring was estimated through SMBG test-strip acquisition as documented by pharmacy claims. Because test-performance rates are not available, we have assumed that the data on test-strip claims correlate with test-strip usage, that is, 100 test strips dispensed = 100 tests assumed. For the purposes of analysis, daily SMBG test-strip usage was estimated using this methodology.
Statistical analysis
All analyses were purely descriptive and conducted on the population starting FSL after the index date in 2017, except for the persistence of FSL system, which was estimated through a Kaplan–Meier survival curve from all initiation occurring after the index date in 2017 and the end of 2019 (Supplementary Fig. S1). As this study was conducted on a single, exhaustive nationwide database, no statistical testing was undertaken for observed differences over time. No missing data were considered. All statistical analyses were conducted using SAS® V9.4 software (SAS Institute, North Carolina, USA).
Results
Patient treatment characteristics
Characteristics of the T2DM population of FSL system users, 65 years of age or older, are described in Table 1. There were 38,312 subjects with T2DM on intensive insulin therapy at the point of initiating FSL. Around 49.8% of these were on insulin therapy only, and 50.2% were also being treated with at least one noninsulin antihyperglycemic drug (AHA). The majority of these (78.6%) were taking metformin and 29.9% were prescribed a GLP-1 receptor agonist (Table 1).
Treatment Characteristics of Patients with Type 2 Diabetes, 65 Years of age or Older, Starting FreeStyle Libre System from August 1, 2017, to December 31, 2018
Data for patients initiating FSL in 2018 did not extend to 24 months.
CSII, continuous subcutaneous insulin infusion; DPP4, dipeptidyl-peptidase; FSL, FreeStyle Libre; GLP, glucagon-like peptide; MDI, multiple daily injections with insulin; T2DM, type 2 diabetes.
After 6–12 months following first use of FSL, a small proportion of patients had stopped intensive insulin therapy and had transitioned to basal insulin-only regimen (±AHA; 3.2%) or AHA treatment only (0.8%) or had stopped any diabetes pharmacologic treatment (4.6%) (Fig. 1). After 12–18 months of FSL use, the number of patients on insulin pump therapy had increased to 15.8% (Fig. 1), with a reduced number on MDI (±AHA; 73.5%) and a further increase in patients who had stopped their diabetes drug treatment (6.8%). In the period from 18 to 24 months, the number of patients on an insulin pump regimen was constant at 15.5% (Fig. 1), but there was an increase in the number of patients using FSL, who had stopped pharmacologic treatment (10.7%).

Treatment characteristics of patients starting the FSL system from August 1, 2017, to December 31, 2018. Pie charts illustrate the treatment regimens at initiation (T0), and at 6–12, 12–18, and 18–24 months after starting the FSL system. All subjects were people 65 years of age or older with T2DM, who were on an intensive insulin regimen (±antihyperglycemic drugs) at the point of starting the FSL system. AHA, antihyperglycemic agents; FSL, FreeStyle Libre; MDI, multiple daily injections with insulin; T2DM, type 2 diabetes.
Rates of hospitalization for ADEs after starting the FSL system
The total rate of ADEs for people ≥65 years of age with T2DM on intensive insulin therapy was 1.60% in the 12 months before starting FSL (Fig. 2). The rates of DKA and SH were 0.61% and 0.74%, respectively. During the 12 months after starting FSL, the total number of ADEs was reduced by 34%, driven by a 54% fall in DKA admissions, with a 15% reduction in hospitalizations for SH (Fig. 2). Diabetes-related comas were reduced by 35% from 0.20% to 0.13% after starting FSL and the small number of hospitalizations for hyperglycemia was reduced by 56%.
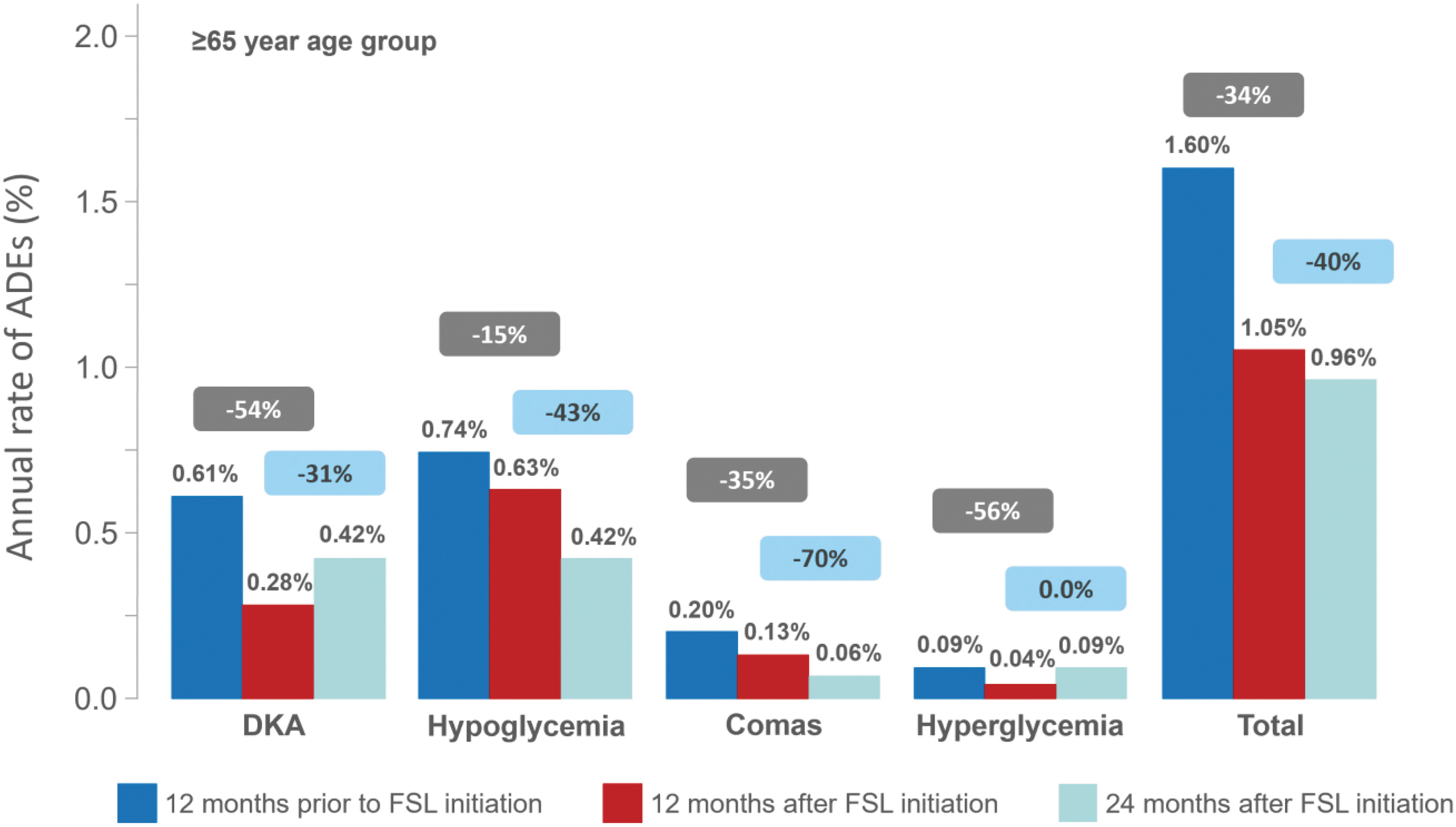
Percentage of people 65 years of age or older with T2DM on intensive insulin therapy with hospital admission for ADEs 12 months before and 24 months after initiation of the FSL system. Data show % of people 65 years of age and older with T2DM, who initiated the FSL system while on intensive insulin therapy and at least one hospital admission for an ADE in the 12 months before FSL initiation and in the 12 and 24 months after initiation (cohort 2017; n = 14,147). Change from 12 months before and 12 months after FSL initiation is shown in gray boxes. Change from 12 months before and 24 months after FSL initiation is shown in blue boxes. ADE, acute diabetes event; DKA, diabetic ketoacidosis.
Notably, the reduction in DKA admissions was maintained up to 24 months. The analysis of the 2017 cohort showed that the fall in SH requiring hospitalization was even more pronounced over the second year of FSL use (−43%; Fig. 2). The number of admissions for diabetes-related comas also showed a further decline over the same period.
When we analyzed the separate age-ranges across the population ≥65 years old (Fig. 3), we found that the pattern of reduction in admissions for SH was generally similar across the age groups. Hospitalization for SH was reduced by 45% among the 65–69-year age group over the first year of FSL use and by 67% over 2 years following the first use of FSL. For subjects 70–79 and ≥80 years of age, there were significant reductions in SH over the second year following FSL initiation (−30% and −46%, respectively), rather than over the first year. For subjects younger than 80 years, reductions in DKA were most pronounced over the first year (Fig. 3). Overall, the frequency of hospital admission for ADEs was highest (1.98%) in the 12 months before starting FSL among subjects ≥80 years old, particularly for SH (0.99%) and diabetes-related comas (0.37%).
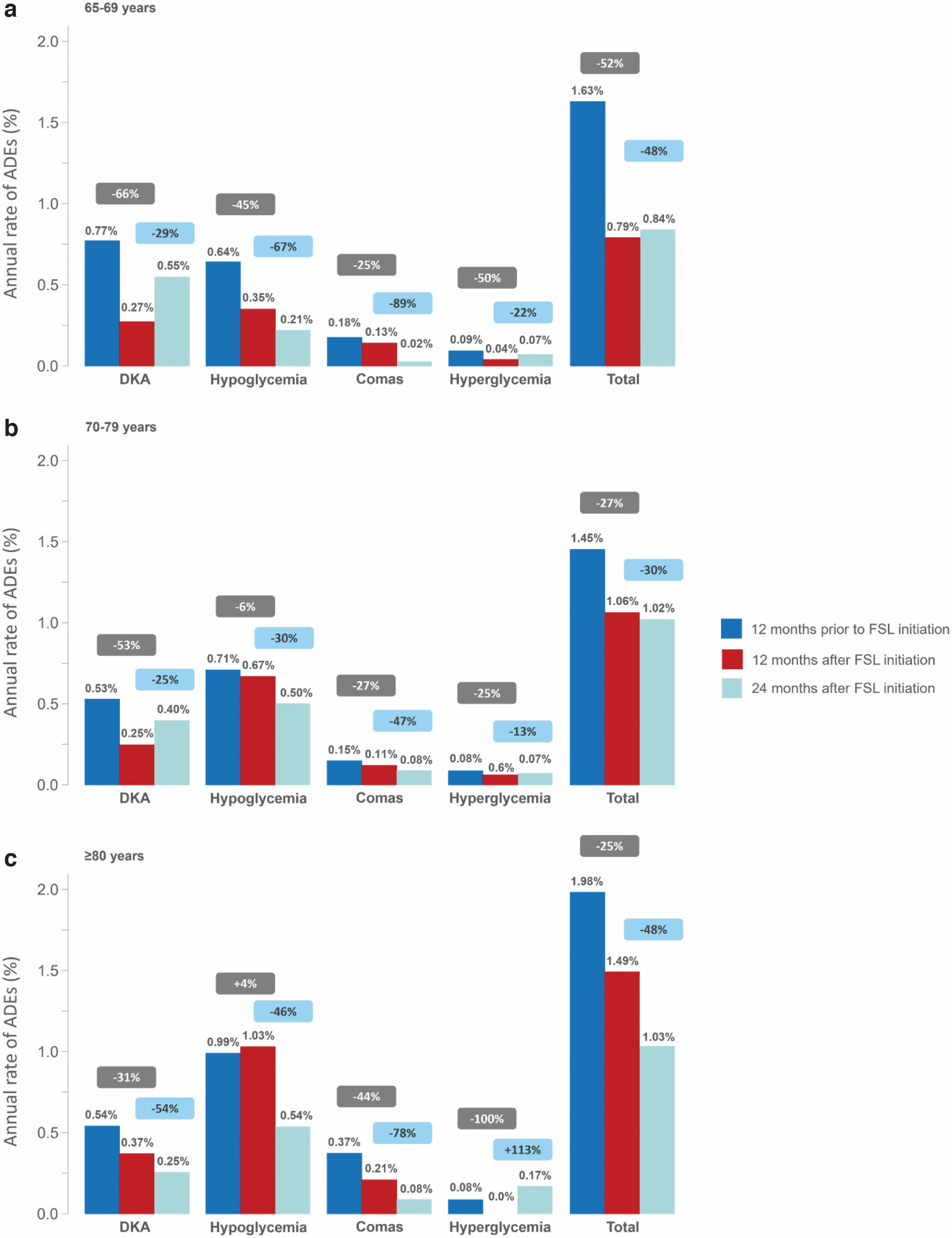
Age-group analysis for people 65 years of age or older with T2DM on intensive insulin therapy with hospital admission for ADEs 12 months before and 24 months after initiation of the FSL system. Data show % of people with T2DM, who initiated the FSL system while on intensive insulin therapy and at least one hospital admission for an ADE in the 12 months before FSL initiation and in the 12 and 24 months after initiation (cohort 2017; n = 14,147).
Persistence with the FSL system
Persistence with use of the FSL system is shown in Figure 4 for the overall population of people 65 years of age or older, with T2DM on intensive insulin therapy, who initiated FSL system between the index date in 2017 (Supplementary Fig. S1) and the end of 2018. The at-risk population shows the number of people still eligible for the calculation. The observation period was shorter for the last patients included, which explains why the population under consideration decreases over time. Persistence at 12 months was 91%, which was maintained at 24 months, with 90% of patients still using the system (Fig. 4). The Kaplan–Meier plot shows that the majority of the 10% discontinuations happened within the first 4 months of starting with the FSL system.

Persistence of FSL use over 2 years following initiation in people 65 years of age or older with T2DM on intensive insulin therapy. Kaplan–Meier survival curve for overall persistence with use of the FSL system over time among people 65 years of age or older with T2DM on intensive insulin therapy at the point of initiation (n = 38,312). Persistence was defined between first delivery of an FSL sensor and discontinuation of the FSL system. The at-risk population shows the number of people still eligible for the calculation. This number over time decreases because the length of observation is not the same for all included patients.
Impact of FSL system use on daily frequency of SMBG testing in people 65 years of age or older with T2DM on intensive insulin therapy
Analysis of the separated age-group profiles showed that, in the 12 months before starting FSL, the mean estimated daily test-strip use was similar for all age groups (Table 2), at 3.3 strips/day (65–69 and 70–79 years) and 3.4 strips/day (≥80 years). Mean estimated test-strip usage was reduced similarly across all age groups 12 months after starting FSL, by 48% (65–69 and 70–79 years) and by 52% (≥80 years), with further substantial reductions in mean estimated test-strip usage over 24 months after starting FSL, by 70% (65–70 years) and by 73% (70–79 and ≥80 years).
Age-Group Analysis of Estimated Average Daily Self-Monitored Blood Glucose Test Strip Usage Before and After Access to the FreeStyle Libre System for People 65 Years of age or Older with Type 2 Diabetes on Intensive Insulin Therapy
Data show the estimated SBMG strip usage, based on pharmacy claims, in the 12 months before and 12 and 24 months after starting the FreeStyle Libre system. Data are shown for people with T2DM on intensive insulin therapy, 65–69, 70–79, and ≥80 years of age (cohort 2017; n = 14,147).
SD, standard deviation; SMBG, self-monitored blood glucose.
Discussion
We have shown in this study that people 65 years of age and older with T2DM on intensive insulin therapy, who initiated FSL between August 1, 2017, and December 31, 2018, experienced a considerable reduction in hospital admission rates for ADEs in the 12 and 24 months period after starting FSL compared to the 12 months before starting. Since this is a retrospective observational study, the reduced admissions can be interpreted to be associated with FSL use, rather than a direct cause-and-effect relationship.
Across this older population with T2DM, the rate of admissions for ADEs overall was reduced in the 12 and 24 months after FSL initiation, compared to the 12 months prior. These reductions were driven by a fall in admissions for DKA in the first 12 months after starting FSL, and by reductions in hospitalizations for SH in the second year after FSL initiation. Age-group analysis revealed that there was a substantial reduction both in the rate of admissions for DKA and SH among subjects 65–69 years of age and that hospitalizations for SH fell further in the second year after starting FSL, compared to the 12 months before starting.
For subjects 65–69 years and 70–79 years of age, the rate of DKA admissions declined in the first 12 months after starting FSL; this result was maintained after 24 months. For subjects 80 years of age or older, the decline in the rate of admissions for SH was seen mainly at 24 months after starting FSL, whereas this elderly group had progressive declines in hospitalization for DKA at 12 and 24 months. Notably, the frequency of hospital admissions for SH and comas before initiation of FSL was increased for subjects 80 years of age or older compared to those younger than 80 years.
The RELIEF retrospective study has previously shown that using FSL is associated with substantial reductions in hospital admissions for ADEs for people with T2DM on insulin therapy. In the 12 months after starting to use FSL, admissions for ADEs among people with T2DM fell by 39.4%. 6 These reductions were driven by a reduced rate of hospitalization for DKA and were maintained over the second year after starting FSL. 8
The results of the analysis reported in this study confirm that the overall rate of ADEs resulting in hospital admission among people 65 years of age or older, with T2DM, who are on intensive insulin therapy, is considerably reduced once they start FSL. In contrast to the overall population of people with T2DM on intensive insulin therapy or basal-insulin only, use of FSL in older subjects with T2DM on intensive insulin therapy is driven by reduced hospitalization for DKA in the first 12 months after starting FSL, whereas the further fall in ADEs in the second year after starting FSL is a consequence of reduced admissions for SH.
These outcomes are important because it is known that the risk of severe or fatal hypoglycemia is considerably increased in elderly individuals with diabetes, who are treated with insulinotropic medications, 18 –20 and the risk of adverse events among elderly people with T2DM treated with insulin is increased compared to those on oral-only medication. 21
The reduction in hospital admissions for SH is evident after using FSL for 24 months for all people 65 years of age or older with T2DM on intensive insulin therapy (−40%), but is most notable among the 65–70-year age group, with a 67% decrease in admissions for SH. This age group also had a 45% reduction in hospitalization for SH in the 12-month period after starting FSL (Fig. 3), not evident in the over 70-year groups. The value of using FSL in all older people with T2DM on insulin therapy is supported by our data, but is arguably more important in the 65–79-year age group, who may have more-active daily lives than the very elderly ≥80-year age group, and for whom the adverse consequences of hypoglycemia may have a considerable impact. 29,30
The pattern of SMBG test-strip use among older people with T2DM on intensive insulin therapy, who initiated the FSL system, matched those of people with T1DM or T2DM on insulin therapy. This showed a considerable reduction in estimated daily SMBG test frequency after 12 and 24 months of using the system (Table 2), as noted in previous studies 6,8,26 and as recommended in clinical guidelines for using CGM in clinical practice in France, 31 endorsed by the Société francophone du diabète (SFD) and the Société française d'endocrinologie (SFE).
The older population studied here were estimated to be similarly adherent with SMBG testing, with the general population of people with T1DM or T2DM, which we had previously identified, 8 based on pharmacy claims data, with no age-dependent difference in daily SMBG test frequency. Estimated use of SMBG tests strips declined by 48% in the 12 months after starting FSL and by 73% over the second year. This may reflect an improvement in patients' confidence as they use the FSL system to manage daily glucose levels and reduce their experience of hypoglycemia or hyperglycemia events compared to SMBG testing.
Another important observation from our study is the persistence of people 65 years of age and older with FSL as part of their diabetes care (Fig. 4). The lack of studies that include significant numbers of older people with T2DM using FSL or rtCGM has led to caution regarding the efficacy of glucose-sensing technologies in this community. However, the available data on smaller groups of older people with diabetes confirm that being older does not reduce either the commitment to use FSL or rtCGM, nor limit the efficacy of glucose-sensing technology as people with diabetes age. In the REPLACE RCT, the subgroup of participants with T2DM on intensive insulin therapy ≥65 years of age (n = 44) scanned their FSL sensors at the same frequency as the younger adult population of people with T2DM. 2
Since the RELIEF study has been conducted using a national claims database without other quantitative data collection, we are not able to analyze scan rates in support of this earlier observation. The DIAMOND study found that using rtCGM for 24 weeks in adults (n = 43) with T2DM on intensive insulin therapy favored improved glycemic control in all age groups, with no difference in outcomes for participants ≥60 years old. 10 Our data confirm in a very large population of people ≥65 years of age with T2DM on intensive insulin therapy (n = 38,312) that starting FSL is associated with substantial reductions in hospital admissions for ADEs, including DKA and SH, after 12 and 24 months of use, and that this is associated with persistence rates of 91% at 12 months and 90% at 24 months (Fig. 4).
The reductions in SH were particularly noticeable for the 65–70-year age group. The persistence in this group was not different from the overall population studied, which was high across all age groups (data not shown). Since the feasibility and acceptability of CGM in very old adults up to 91 years of age have also been demonstrated, 32 the case for wider access and application of FSL in older and elderly people with T2DM on insulin therapy is clear. As stated, the outcomes reported in this study are associated with starting the first generation FSL sensor, without optional glucose alarms. Subsequent generations of FSL sensors allow the user to receive high and low glucose alerts, which may further support avoidance of ADEs and associated risk of hospitalization, as has been indicated by the ALERTT1 study. 33
Strengths and limitations of our study
Strengths of the study include its large size and the nationwide scope, in the context of a national reimbursement scheme. The observational time frame of 24 months is also a strength of the study. Our study also has limitations. We have presented data on people 65 years of age or older, with T2DM on intensive insulin therapy who have been prescribed FSL. This is a highly selected group and the outcomes cannot be generalized to the whole population of people with T2DM in France on FSL, nor to the subgroup of people 65 years of age and older with T2DM, not on intensive insulin therapy.
Equally, we cannot exclude a selection bias toward an older population who were also particularly prone to ADEs, and thus required an intervention with FSL. Since the reported outcomes of the RELIEF study are derived from a longitudinal retrospective cohort analysis, it is possible that confounding factors, other than use of the FSL system, may have affected the outcomes. For example, diabetes education and more focused time with healthcare professionals during the FSL initiation process may have empowered the patients to improve their diabetes self-care behavior in a way that affected the frequency of ADEs. The inclusion of a control group could have both mitigated a recruitment bias and also highlighted the impact of factors other than FSL itself on the incidence of ADEs over the 24-month study period. The lack of such a group is a major limitation.
Nevertheless, since the reductions in DKA and SH persist for at least 2 years after initiation, we can argue that the observed fall in hospital admissions for ADEs is related to use of the FSL system. The lack of a matched control population does not allow us to draw this as a firm conclusion. Another limitation in this context is that we do not have data on CGM devices other than the FSL system, which was the only system reimbursed in France at the time. Also, the SNDS claims data do not provide sensor scan rates, nor does it include clinical or biological data, such as HbA1c measurements, and these are limitations.
Conclusion
This further analysis of our previous RELIEF study population confirms the association of the FSL system with reductions in hospital admissions for ADEs in people 65 years of age or older, with T2DM on intensive insulin therapy, in France. As with our previous studies, the reductions in admissions for ADEs are persistent at 2 years. 8 This emphasizes that FSL should be more widely prescribed as part of individualized care for older and elderly patients with T2DM treated with intensive insulin regimens, who may be at risk of DKA or SH requiring hospitalization, and in whom the consequences of SH can extend beyond falls and fractures, to dementia and cardiovascular events.
Footnotes
Authors' Contributions
B.G. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of data and the accuracy of the data analysis. F.L.-G. contributed to the methodology, the analyses, and the article writing. E.V. contributed to the methodology, the analyses, and the article writing. G.D.P. contributed to the methodology, the analyses, and the article writing. B.D. and C.E. contributed to the methodology, conducted the statistical analyses, and contributed to the article writing. J.-P.R. contributed to the methodology, the analyses, and the article writing. Editorial assistance in the preparation of this article was provided by Dr Robert Brines of Bite Medical Consulting.
Disclaimer
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Compliance with Ethics Guidelines
This article does not contain any study with human participants or animals performed by any of the authors.
Data Availability
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Author Disclosure Statement
B.G. is an advisory board member for Sanofi, Eli Lilly, NovoNordisk, Novartis, GSK, MSD, Boehringer Ingelheim, AstraZeneca, Abbott, Medtronic, and Roche Diagnostics. He is a clinical investigator for Sanofi, Eli Lilly, NovoNordisk, GSK, BMS, AstraZeneca, Medtronic, Abbott, Roche Diagnostics, MSD, Novartis, Janssen, and Boehringer Ingelheim. He receives research support from Medtronic, Vitalaire, Sanofi, Eli Lilly, and Novo Nordisk. F.L.-G. is employed by Abbott Diabetes Care. E.V. is a consultant specializing in the methodology and statistical analysis of clinical trials for Abbott, Bristol-Myers Squibb, Celgene, Edwards, Novartis, Pfizer, and Sanofi. He has received honoraria for his participation. G.D.P. is a health economist and an advisory board member for the following companies: Abbott, Amgen, Astra-Zeneca, Bayer, BMS, Boehringer-Ingelheim, Janssen, MSD, Novartis, Novo Nordisk, Roche, and Sanofi. He has received research funding from Amgen, BMS, Boerhinger-Ingelheim, MSD, Novartis, Roche, and Sanofi. He has received honoraria for his participation to the RELIEF study advisory board. B.D. and C.E. are employees of CEMKA, a French Healthcare CRO. B.D. has also received advisory board and lecture fees from Sanofi, MSD, Eli Lilly, Novo-Nordisk, Pfizer, and Janssen. J.-P.R. is an advisory panel member for Sanofi, MSD, Eli Lilly, Novo Nordisk, AstraZeneca, Abbott, Dexcom, Alphadiab, and Medtronic; and has received research funding and provided research support to Abbott, Air liquide, Sanofi, and Novo Nordisk.
Funding Information
The authors acknowledge funding support from Abbott Diabetes Care. The funding did not affect the collection, analysis, or presentation of data.
Supplementary Material
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.