
Abstract
Background:
Since the introduction of insulin pumps into the therapy of pediatric subjects, different approaches have been taken to find optimal basal rates. Previously, the DPV registry provided circadian basal rate patterns for different age groups. As the number of pump users has increased recently and short-acting insulin analogues are now predominant, we performed a new analysis with a larger data pool.
Methods:
We included all recent basal profiles from type 1 diabetes (T1D) patients between 1 and 25 years from the DPV 2021 data pool. We excluded night-time-only pump users, human regular insulin users, and daily basal rates <0.05 and >1.0 U/(kgBW·d).
Results:
In the analysis of profiles from 25,718 young persons with T1D, differences in the daily pattern of basal rates were found between age groups. In addition, we saw significant (P < 0.001) differences in total daily basal dose between genders in all age groups except adults. In addition, the shape of the expected basal-rate pattern differed by body mass index, HbA1c, and use of continuous glucose monitoring.
Discussion:
This analysis demonstrates multiple factors influencing basal patterns and insulin requirement, including age group, gender, overweight, HbA1c, bolus frequency, and sensor use. As circadian basal rates are still mandatory for initiating insulin pump therapy with or without automation, a multimodal approach is necessary to estimate optimal basal rates.
Background
In Germany, the use of continuous subcutaneous insulin infusion (CSII) has been on the rise for children and adolescents with type 1 diabetes (T1D) across all age groups since 2000. 1 By 2021, 56% of young individuals with T1D in Germany, Austria, and Luxembourg had adopted CSII with 86% in the preschool age; it is, therefore, considered a standard therapy within this age group. The utilization of continuous glucose monitoring (CGM) also increased significantly since 2016. 2
Most studies on insulin pump therapy (CSII) for children have been conducted in Europe and the United States. 3 The first ideas of a circadian dawn–dusk profile for insulin pump basal rate patterns were described in the 1990s by Renner and colleagues 4 for adult subjects. After that, differences in basal rates throughout the day were described according to age groups. 5 –7 As a result, standard profiles have been developed and analyzed for various age groups. 8
A recent study showed that starting CSII with a circadian pattern could improve dose optimization. Optimal basal rate patterns were evaluated in a clinical setting with 150+ participants. 9 Some groups, however, have disputed the superiority of circadian profiles in adults, 10 and there is evidence that variability of basal rates, as opposed to a more constant profile, may be associated with complications in adults. 11
In a German rehabilitation center study, a clinical approach was taken with 339 adult patients to determine their basal insulin requirement through a 24-h fasting process. 12 Owing to metabolic and practical concerns, a 24-h fasting test is unsuitable for children. Shorter fasting periods are advised to assess basal insulin requirements, avoiding hormonal reactions to fasting, which may interfere with the results.
For starting insulin pump therapy, some recommendations suggest starting with a flat basal rate (e.g., 50% of total daily dose [TDD] equally distributed over 24 h). 13 Recommendations for children are comparable. 14 However, a more physiological approach is to adjust insulin delivery to a circadian insulin sensitivity pattern. Pediatric experts typically suggest a variable basal rate that includes two peaks: one in the early morning (dawn) and one in the late afternoon (dusk).
Since September 2019, the first devices with automated insulin dosage (AID) have been available in Germany, Austria, and Luxembourg.
AID data evaluation shows that automated insulin delivery in pediatrics also follows circadian patterns. 15 Although insulin requirement varies throughout the day in association with the dawn phenomenon in adults, a study by Lindmeyer et al. showed that starting CSII with a constant infusion rate is safe. 16
Among the five currently (European Union and the United States) marketed AID systems, two use a preset basal rate during the auto mode, and all five use a user-defined basal rate as a backup if the algorithm cannot implement automated mode or if the user switches this off. While using automated modes, routine basal rate adjustment in the outpatient clinic is more difficult because the traditional separation of basal and bolus insulin does not reflect the insulin dosing algorithms. 17 Therefore, when using AID systems, expected circadian profiles are still required as a basis for insulin pump settings at the start of therapy.
In Germany, available schemes based on aforementioned publications are widely used to determine basal patterns, with subsequent individual adjustments. This routine and patient education on technical aspects proved beneficial for overall glucose control during CSII use in an international comparison. 18
The DPV registry is a vast database on diabetes that has been collecting patient data since 1995 in Germany, Austria, Switzerland, and Luxembourg. 19 The currently recommended standard dosing schemes for pediatric subjects were published in 2008 and are based on the DPV data pool at that time. 20 A subsequent analysis was conducted in 2012. 21
Methods
Study design and participants
We included data from the DPV registry between 2015 and 2021 on all individuals with T1D using an insulin pump (CSII therapy), including AID between the ages of 1 and 25. The most up-to-date basal rate information for each person, regardless of self monitoring of blood glucose (SMBG) or sensor monitoring, was used. We excluded patients on injection therapy, patients who used CSII only during night-time, or patients with CSII but no available basal rate. We also excluded basal rates that showed no insulin delivery for >2 h.
In addition, we excluded users of human regular insulin and subjects with total daily basal rates <0.05 or >1 U/(kgBW·d) due to suspected honeymoon phase, extreme insulin resistance, or documentation errors. We did not consider profiles with >30 bolus administrations documented per day to analyze bolus frequency, assuming erroneous data entry. Individuals with missing body mass index (BMI)-standard deviation scores (SDS), HbA1c, or number of daily bolus administrations were only excluded from the analysis of the respective parameter.
Patient data
Our method for calculating BMI involved the use of SDS derived from German reference values provided by the Arbeitsgemeinschaft Adipositas im Kindes- und Jugendalter (AGA). 22 If an individual's BMI-SDS exceeded the 90th percentile for age and sex, they were classified as overweight. The HbA1c values were adjusted to the Diabetes Control and Complications Trial (DCCT) reference range of 4.05%–6.05% (20.7–42.6 mmol/mol) by using the multiple of the mean transformation method to accommodate for the variations in laboratory methods. To meet the criteria of sensor use, the individual must have used the sensor for at least 80% of the days in the 90 days before their most recent visit.
Statistical analysis
To compare age groups (1 to <6, 6 to <12, 12 to <18, and 18 to 25 years), we utilized the most recent basal rate per patient and age group. Each person could, therefore, provide one to two basal rates for this analysis, as the analysis timespan is 6 years and, therefore, individuals' age group has changed in that period for all other comparisons, each subject's most recent basal rate was used, and each individual contributed one basal rate. Stratification was conducted by weight category (normal weight/overweight), HbA1c category (<7.5% vs. >7.5%), and the number of boluses (<6 vs. ≥6). 23
We compared unadjusted means, stratified by age group, to analyze differences in basal insulin dose between sexes. The analyses according to BMI category, HbA1c category, number of boluses, and sensor use were conducted with multivariable linear regression models adjusted for age groups, sex, and diabetes duration groups (<2/≥2 years) as well as for interaction terms between age group and sex and between diabetes duration group and sex.
We calculated the absolute difference for each hourly interval using logistic regression models, again adjusted for the confounders mentioned earlier to analyze the differences in the basal rate trajectories between groups. An interaction term for the respective outcome variable and the hourly intervals as a time variable was additionally included. To determine if there were significant variations between the curves, the P-value of this interaction term was utilized. Furthermore, the absolute differences of all hourly intervals were summed up, representing the area between the curves and, therefore, a standardized and comparable value for quantification.
All calculations were performed using SAS version 9.4 (build TS1M7) on a Windows server 2019 mainframe. Significance was determined using a two-sided P-value of <0.05.
The DPV registry is approved by Ulm University's ethics board.
Results
The registry contained records of 25,718 patients whose most recent profiles met the inclusion criteria (Supplementary Fig. S1).
An “AGP-like” figure (including median and areas between the 10th, 25th, 75th, and 90th centile) shows a high variability over 24 h with a larger distance between the 10th and 90th centiles in the evening hours (Fig. 1).
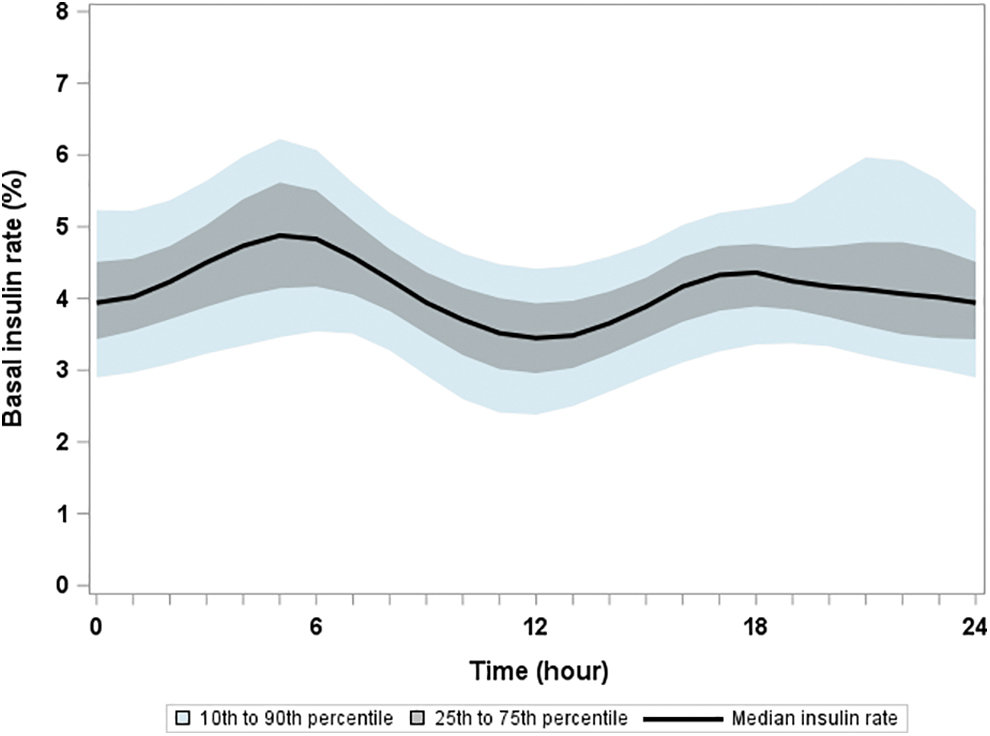
“AGP-like” overall patterns of basal rates (whole population). AGP, ambulatory glucose profile.
The median number of daily boluses administered was 6 [5;6] in all age groups without differences according to sex.
The analysis of sex differences was performed in four separate age groups (Table 1) based on the most recent basal rate per patient and age group: 1 to <6 years, n = 5716; 6 to <12 years, n = 12,116; 12 to <18 years, n = 15.494; 18 to 25 years, n = 4472. Only 486 people (1.9%) were current AID users.
Demographic Data and Insulin Doses; Groups According to Age and Gender
Data are presented as median [Q1; Q3].
Asterisk indicates statistically significant difference in individual age group according to sex (*<0.05, ** <0.01, and *** <0.001).
BMI, body mass index; SDS, standard deviation scores; TDD, total daily dose.
Patterns
The basal rates showed different circadian patterns among age groups. Figure 1 shows a wider centile curve during the evening hours, mainly due to the pattern in the youngest age group. This group has a different curve shape and a higher percentage of basal insulin in the evening than other age groups.
Comparing age groups, the proportion of insulin distribution differs most between the youngest and oldest age groups, with a difference of 19.6% of the total proportion (Fig. 2a). Figure 2b quantifies hourly differences between the youngest and the oldest age group. Differences between sexes were smaller within the individual age groups (for quantification of other group comparisons, see Supplementary Fig. S2). The most negligible sex difference was observed in the preschooler age group (1.81%).
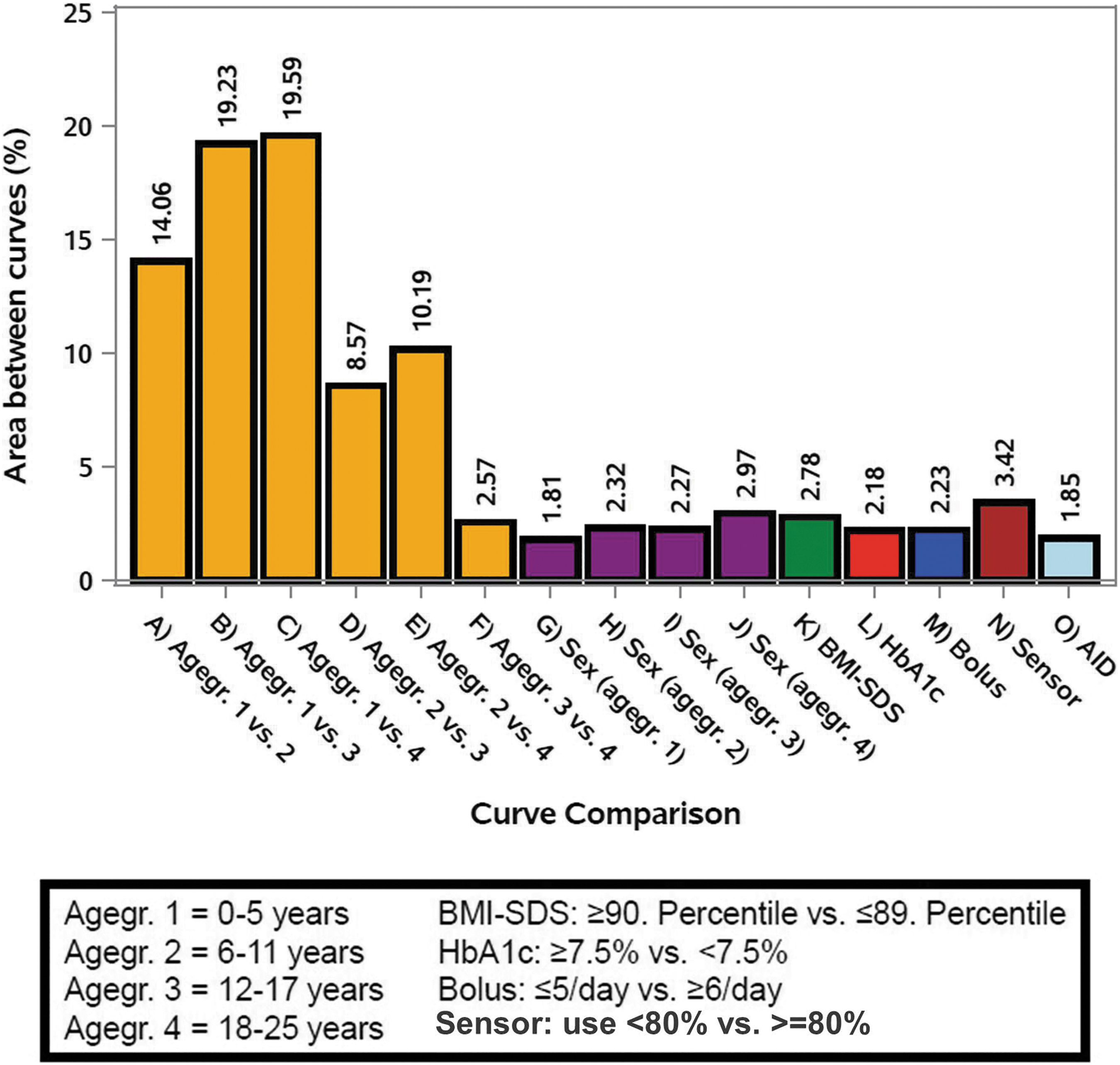
AUC differences between individual groups. For every paired comparison, the absolute number of AUC difference was calculated (Supplementary Fig. S2); results shown as bars. AUC, area under the curve.
Figure 3 shows the different shapes of basal patterns in the individual age groups (Fig. 3a–d). As the hourly delivered basal rate depends on all the aforementioned factors, the basal rate patterns are expressed as a proportion of the total daily basal insulin requirement. Therefore, the sum of all hourly intervals is 100%. Figure 3e–h shows the corresponding absolute mean hourly insulin dose.

Basal patterns stratified by subgroups.
Discussion
We present patterns for expected basal insulin requirement during CSII therapy from a large multinational diabetes registry. The number of subjects included in the current publication increased four times compared with the previous publication in 2012. 21 The age groups are <6 years (n = 837), 6 to <12 years (n = 1739), 12 to <18 years (n = 2985), and 18 to <25 years (n = 380). It is worth noting that the currently available basal rate recommendations only include data from 743 patients. 20 Furthermore, other advancements also support this recalculation: use of CGM instead of SMBG, 24 nearly exclusive use of rapid-acting analogues, 25 new pump models, 26 earlier switch to CSII from basal-bolus regimen, 27 and lower targets for HbA1c. 28
It is worth noting that the basal patterns comparing the four age groups remained consistent with previous data. The shape and hourly proportion of CSII basal rate depends on age, sex, BMI, number of daily boluses, and quality of diabetes control. In addition to the circadian distribution, the total daily basal rate requirement differs among the groups, so both factors must be considered for recommended basal rate settings in an individual subject.
Studies have indicated that insulin regimens should be adjusted based on age 29 and the time of day. 30 In adults, age, sex, duration of insulin pump treatment, BMI, HbA1c, and triglyceride concentrations essentially predicted the individual basal insulin requirement per day. 7
Karakus et al. studied 4193 daily AID profiles to demonstrate circadian insulin needs, which are comparable with our results. They analyzed the profiles separated into microboluses and autocorrections, both features of the device used in their study. Their mean participant's age was 12.3 years. Their findings indicate that a circadian profile requires two insulin peaks: one in the morning between 4:00 and 8:00 (corresponding to the dawn phenomenon 31 ). The second peak they found was a steady increase from noon to bedtime (corresponding to the dusk phenomenon). Our data show that the two insulin peaks are similar to the basal rate pattern of 12- to 18-year-olds in our study. Therefore, the data confirm that insulin requirement corresponds to the shape of the curve presented in our study.
Physicians' clinical approach to adjusting pump treatment settings based on sensor data shows a tremendous intraindividual variety that differs from computer-generated suggestions. 32 Using empirical data from a large population can facilitate the initiation of pump therapy. The shape of the basal rate distribution in adults is similar to the curve evaluated by Nauck et al. in their clinical fasting test with adult patients, 12 but different compared with the distribution in adolescents. Thus, the profile presented reflects the need for a circadian adult basal rate, consistent with the results from Nauck et al.
Influencing factors—sex and age
The impact of sex varies depending on age. Boys and girls in the youngest age group require almost the same amount of insulin. In contrast, the 6- to 12-year-old group shows a higher total basal insulin dose in girls (Fig. 2) and a higher basal insulin dose per kg of BW (Table 1). The sex difference is reversed in young adults. One possible explanation for this phenomenon is that girls experience puberty earlier, which results in a higher demand for insulin at a younger age. Males begin puberty later and continue to undergo changes for a more extended period. 33 Furthermore, in the pubertal age groups, the circadian insulin distribution patterns differ most between the sexes (Fig. 2b, d).
During a lifetime with T1D, adolescence is the period that experiences the poorest metabolic control. In adolescence, most people with diabetes (PwD) are not meeting their metabolic targets, 18 partly due to risk-taking behavior. This group has the highest number of disruptors of glycemic control: pubertal hormone surge, nocturnal growth hormone secretion, the highest amount of TDD, and low adherence to treatment recommendations. All these factors contribute to unstable metabolic control.
Treatment result
When possible, for the individual patient and resources are available, a treatment target for HbA1c <7% is recommended. 28 Our data show that people meeting the target have different patterns than those who do not. Cross-sectional data cannot answer whether a more physiological basal rate supports better glycemic control or whether worse metabolic control influences the 24-h-pattern of basal insulin requirement.
Implications for current and future therapy
All current AID systems on the market are using sensors that need a “warming phase” of at least 1–2 h (depending on the used model). That means, every AID user has breaks in AID use regularly. Furthermore, technical issues with sensor malfunction or just prematurely solution of adhesive might lead to sudden interruptions in AID mode. For all these cases, an individual optimal basal rate, based on parameters described earlier, help the user to keep glycemic control until AID can be resumed.
Furthermore, depending on the AID system used, the preprogrammed basal rate is needed for the automated modus. All current systems use the TDD of insulin as a parameter for the AID algorithm. Some incorporate also the previous basal rate for AID calculation, some take the TDD from the past days to calculate ratios. In both cases, an optimal basal rate helps to provide an individual program with person's individual insulin need.
In general, the concept of insulin delivery in AID mode is more “manual and automated” then “basal and bolus” as mentioned in the current ISPAD guidelines for insulin delivery. 34
By today, one system also uses the programmed basal rate during automated therapy. For users of this system, an individual fitted basal rate is the base for automated therapy. There might be factors in the algorithm, for example, a maximum of hourly basal, calculated by the programmed patterns. In this case, an optimal rate is recommended, whereas in the past, fasting tests were used to find these optimums, precalculated patterns (Supplementary Fig. S3) based on these data can provide easy access to appropriate basal rates.
The first randomized controlled trial with a so-called “open-source” AID system was recently published. 35 As these systems are not certified or approved by any authority or notified body, the risk of system failure might be more critical. Also, in these self-build systems, an applicable basal rate should be used as a backup system in case of a nonworking AID.
In general, artificial intelligence-powered systems are often seen as “the” promising treatment for T1D, with potential benefits for users and care teams. However, a recent statement by European Association for the study of Diabetes and American Diabetes Association points out some issues that need to be solved with this technology, including regulatory aspects, data harmonization, and the use of various systems. 36
Our study revealed that the difference in area under the curve between the adolescent and young age groups was smaller than the sex differences observed in the adults' group (2.57% vs. 2.97%; see Fig. 2a). This finding suggests that insulin patterns are influenced by all the investigated factors independently. Therefore, a standardized backup basal rate considering all the factors discussed earlier may provide support and safety for PwD and diabetes teams that must adopt this new technology.
Strengths and weakness
Real-life data from PwD's insulin pumps are entered into the prospective database. The current goals for therapy are to achieve an HbA1c level <7.0% 28 and a time in range >70%. 37 Nevertheless, diabetes teams can identify personalized goals with their patients; therefore, the aims might have differed in individual patients, and some documented basal rates might not be the optimal approach to achieve these glycemic targets. This might be considered as a weakness of our study. However, compared with reports from other countries, the population in our study has good diabetes control. 38 Therefore, the recommendations presented can be judged as adequate basal rates for our population.
Strength of our study is the large data set from multiple centers in four countries, the standardized documentation using one single electronic health record software, and the centralized analysis.
Conclusion
Based on the data presented, the patterns of individual basal rates and the total amount of basal insulin needed vary depending on several factors, including age, sex, BMI, and the number of boluses administered per day. These factors have not been previously investigated, but they are crucial in determining personalized recommendations for basal insulin requirements. In addition, physical activity, body composition, nutrition choices, emotional stress, and mental health are likely to affect basal rate patterns.
These multiple factors must be considered when estimating basal insulin requirement. For now, the sliding basal rate dosing schemes from the last publication have been updated (Supplementary Fig. S3). AID systems still require a programmed basal rate, either as a backup or as part of the algorithm. Therefore, a tool incorporating all these factors might be valuable in routine diabetes care.
Footnotes
Acknowledgments
We would like to thank A. Hungele and R. Ranz for their support with data management and the development and continuous improvement of the DPV documentation software (both on the DPV team at Ulm University). Special thanks to Katharina Strehle for supporting the statistical analysis. We appreciate participation of all diabetes centers in Germany, Austria, Switzerland, and Luxemburg (see annex). We like to thank DexCom Germany for development of the basal rate tool based on these results.
Authors' Contributions
T.B. and R.W.H. planned the study. A.E. performed all statistical analyses and advised the author group on data analysis. All authors contributed to interpretation of results and discussion. The manuscript's first draft was written by T.B., read, revised, and approved by all coauthors. The data were collected by all DPV centers.
Author Disclosure Statement
T.B. reports speaker's honoraria from Insulet, NovoNordisk, Medtronic, Roche, Sanofi, Synlab, and Ypsomed, Advisory board activity for Ascensia, Medtronic, and Sanofi. Member of EMA Expamed panel. B.R.-M. reports speaker's honoraria from Abbott, Insulet, Medtronic, Eli Lilly, and Ypsomed. A.E., M.B., C.B., S.G., B.H., C.K., S.M., and R.W.H. report no conflict of interest.
Funding Information
The development of a new device to predict basal rates for CSII in children, adolescents, and young adults with T1D was supported by three pediatric professional associations from German-speaking countries: the German AGPD (
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.