
Abstract
Background:
Advanced hybrid closed-loop (AHCL) automated insulin delivery systems are the most effective therapy in terms of assisting people with type 1 diabetes (T1D) to achieve glycemic targets; however, the cost can represent a barrier to uptake. In this study, a cost–utility analysis of the MiniMed™ 780G AHCL system (MM780G) versus intermittently scanned continuous glucose monitoring (is-CGM) plus multiple daily insulin injections (MDI) in people with T1D not achieving glycemic goals was performed across six European countries.
Methods:
Clinical input data were sourced from the ADAPT trial. Assuming a baseline HbA1c of 9.04%, HbA1c reductions of 1.54% for AHCL and 0.2% for is-CGM+MDI were modeled. The analyses were performed from a payer perspective over a time horizon of 40 years and an annual discount rate of 3% was applied.
Results:
Across all countries, the use of AHCL was projected to result in an incremental gain in quality-adjusted life expectancy of >2 quality-adjusted life years (QALYs) versus is-CGM+MDI. Lifetime direct costs were higher with AHCL resulting in incremental cost–utility ratios for AHCL versus is-CGM+MDI ranging from EUR 11,765 per QALY gained in Austria to EUR 43,963 per QALY gained in Italy.
Conclusions:
For people with T1D managed with is-CGM+MDI not achieving glycemic targets, initiation of the MM780G system was projected to improve long-term clinical outcomes; however, due to differences in health care costs between countries, the health economic outcomes differed. In all included countries, AHCL is likely to be cost-effective relative to is-CGM+MDI for people not achieving glycemic goals with is-CGM+MDI. The ADAPT trial is registered with ClinicalTrials.gov, NCT04235504.
Introduction
For people living with type 1 diabetes (T1D), the use of technologies such as insulin pumps and continuous glucose monitoring (CGM) can assist with the everyday burden of disease management and improve glycemic control, which can in turn reduce the risk for long-term complications that are associated with substantial morbidity and high direct costs. 1 As such, the uptake of intermittently scanned CGM (is-CGM), real-time CGM, and insulin pumps has steadily increased such that these devices are now considered to represent the standard of care in some settings. 2 Moreover, evidence from the recent multinational ADAPT randomized controlled trial (RCT) 3 suggests that, for people living with T1D and not achieving glycemic targets, the use of the MiniMed™ 780G (MM780G) advanced hybrid closed-loop (AHCL) system (Medtronic, Northridge, CA) can provide clinical benefits over and above those achieved with is-CGM combined with multiple daily insulin injections (MDI).
However, the initial cost of these devices and the ongoing costs for consumables, together with the limited coverage/reimbursement from payers and disparities in availability and access, have been acknowledged as major barriers to further uptake. 4 Other factors may also influence uptake, for example, in the United Kingdom, variability in the uptake of diabetes devices according to center, deprivation level, and local prescribing policies has been reported. 5,6
Given the role of cost as a barrier to uptake, long-term health economic analyses can play an important role in helping payers and policymakers to weigh the immediate short-term costs associated with device acquisition against the potential long-term savings that could result from reductions in the risk of costly long-term complications such as cardiovascular and renal disease. However, there may be some variation in the cost-effectiveness of the same device across different countries owing to differences in device acquisition costs and the direct costs associated with the treatment of complications. For example, in a recent analysis examining the costs of severe hypoglycemic events (SHEs) across nine European countries, the cost of a hospital-treated SHE ranged from EUR 279 in Bulgaria to EUR 1176 in Slovenia. 7 Similarly, willingness-to-pay thresholds may also vary across settings.
Given the increasing role of devices such as CGM and AHCL in T1D management and the value of health economic analyses in assisting payers in making informed decisions, the aim of the current analysis was to compare the cost–utility of the Medtronic 780G AHCL system versus the Abbott FreeStyle Libre is-CGM device combined with MDI across six different European countries (Austria, Greece, Italy, The Netherlands, Spain, and Sweden). The clinical input data were sourced from a head-to-head clinical trial in people living with T1D not achieving glycemic targets on is-CGM+MDI. is-CGM+MDI was chosen as the comparator as this represents the standard of care for many people with T1D in the countries included in the analysis and also allowed the analysis to be based on robust clinical data from the ADAPT RCT.
Methods
Model structure
The analysis was performed using the IQVIA CORE Diabetes Model (CDM) version 9.5. A full description of the original model structure and a validation have been published by Palmer et al. 8,9 and a more recent validation is described in McEwan et al. 10 Briefly, the CDM is a validated and extensively used computer simulation model that can be used to project long-term clinical and economic outcomes for both type 1 and type 2 diabetes. Outcomes of interest for the analysis included quality-adjusted life expectancy, the cumulative incidence of complications, total lifetime costs, and the incremental cost–utility ratio (ICUR).
Baseline cohort characteristics and treatment effects
Baseline cohort characteristics were sourced from the ADAPT study (Table 1). 3 The mean (standard deviation [SD]) age of the simulated patient cohort was 40.6 (12.35) years and the mean (SD) HbA1c at baseline was 9.04 (0.85) % (75.3 [9.3] mmol/mol). Treatment effects were also sourced from 6-month data from ADAPT 3 and the same treatment effects were used across all six countries. Specifically, in the MM780G AHCL arm, an HbA1c reduction of 1.54% (16.8 mmol/mol) from baseline was assumed, while in the is-CGM+MDI arm, the corresponding decrease was assumed to be 0.2% (2.18 mmol/mol). The incidence of SHEs requiring either third-party assistance (SHE 1) or medical assistance (SHE 2) and the incidence of ketoacidosis was assumed to be zero in both arms, again based on 6-month data from ADAPT. In addition, in the base case analysis, 100% adherence with device use was assumed.
Baseline Cohort Characteristics
Source: Choudhary et al. 3 and Medtronic data on file.
SD, standard deviation.
It was also assumed that people in the simulated cohort remained on either AHCL or is-CGM+MDI for the entirety of the simulation, and HbA1c (and other physiologic parameters) was assumed to progress based on the default progression values applied in the CDM.
As ADAPT was a multinational study, default CORE model values for nonspecific mortality were used across all countries included in the analysis.
The ADAPT study was conducted in line with the principles of the Declaration of Helsinki, good clinical practice, and local legislation. 3 Approval was obtained for all study centres from competent authorities and ethics committees. 3
Costs
The incremental annualized device costs for AHCL are shown in Table 2. For the is-CGM+MDI arm, treatment costs included an anticipated use of 26 sensors per year. The cost of insulin was also included, based on a total insulin dose of 54 units per day in line with the ADAPT study.
Incremental Cost of MM780G Advanced Hybrid Closed-Loop Relative to Intermittently Scanned Continuous Glucose Monitoring+Multiple Daily Insulin Injections (Annualized)
Is-CGM+MDI costs include the cost of one reader every 2 years in Austria and Sweden and one reader per year in The Netherlands; no costs for the reader were accounted in Greece or Italy; includes cost of 26 sensors per year in all countries. Cost of insulin was based on total insulin use of 54 units per day.
MM780G AHCL costs include cost of pump (assumed to be replaced once every 4 years in all countries except Greece where pump replacement interval was 5 years), 52 sensors per year, 2 infusion sets and reservoirs per week, and 1 Guardian™ 3/4 Link kit (including Guardian 3/4 Link transmitter, charger, cleaning plugs, battery, and One-press Serter) per year in all countries except Austria where the Guardian 3/4 Link kit was assumed to be replaced every 2 years). Costs are based on the Guardian 4 sensor in Austria, Greece, The Netherlands, and Sweden, and the Guardian 3 Sensor in Italy. Insulin costs are also included based on total insulin use of 54 units per day.
Conversion to EUR is based on the average exchange rate for 2022.
AHCL, advanced hybrid closed-loop; is-CGM, intermittently scanned continuous glucose monitoring; MDI, multiple daily insulin injections.
In the MM780G AHCL arm, device costs were annualized according to the procurement conditions in each country at the time the analysis was conducted and assumed periodic replacement of the device in line with the warranty. It was also assumed that the Guardian™ 4 Link kit (including Guardian 4 Link transmitter, charger, cleaning plugs, battery, and One-press Serter) was replaced annually (except for Austria where the Guardian 4 Link kit was assumed to be replaced every 2 years). In addition, in The Netherlands, costs were based on the Guardian 3 Link kit. Treatment costs in the AHCL arm also captured the use of 52 sensors annually and insulin costs were also included based on a total insulin dose of 54 units per day.
Direct costs for diabetes-related complications were sourced from previously published literature (Table 3) and inflated to the 2022 values for all countries (except Spain where costs were inflated to the 2023 values).
Costs of Diabetes-Related Complications
Conversion based on average exchange rate for 2022.
Includes amputation and prosthesis.
IPF, Insitut für Phamaökonomishce Forschung, LKF, Leistungsorientierte Krankenanstaltenfinanzierung; ÖGK, Österreichische Gesundheitskasse; NSHE, nonsevere hypoglycemic event; SHE 1, severe hypoglycemic event requiring third-party assistance; SHE 2, severe hypoglycemic event requiring medical assistance.
Utilities
Utility values for acute and long-term diabetes-related complications were identified from a published literature review specific to people living with T1D 11 (Supplementary Table S1). A sensitivity analysis was performed using utility values sourced from a report on CGM published by the U.K.-based National Institute for Health and Care Excellence 12 and a literature review by Beaudet et al. 13 (Supplementary Table S1).
The effect of is-CGM+MDI and AHCL on the quality of life due to reduced fear of hypoglycemia (FoH) was included in the analyses by converting FoH data from ADAPT to a utility benefit, based on previous data in which a one-point improvement in FoH (measured using the Hypoglycemia Fear Survey) corresponds to a utility benefit of 0.008 (using the EQ-5D[index]). 14 A utility benefit of 0.0544 was applied to the MM780G AHCL arm, based on 12-month data from ADAPT, and a benefit of 0.016 was assumed for the is-CGM+MDI arm, based on 6-month data from ADAPT; 12-month data were not available for the is-CGM+MDI arm as following the 6-month study period, participants in this arm were switched to MM780G AHCL for a 6-month continuation phase. 15
Time horizon, perspective, and discount rates
All base case analyses were performed from a payer perspective over a time horizon of 40 years. An annual discount rate of 3% was applied to both future costs and clinical outcomes across all six countries included in the analysis. The rationale for the use of the same discount rate across all countries was to permit comparison of results across the different settings.
Sensitivity analyses
A series of one-way sensitivity analyses were performed to determine the key drivers of results. Sensitivity analyses around treatment effects included investigating the effect of a 20% increase or decrease in terms of the reduction from baseline in HbA1c. A sensitivity analysis was also performed in which the baseline HbA1c was assumed to be 8.0%, with the between-group difference at 6 months (−1.48%) in this analysis calculated based on a regression model using individual patient-level data from the ADAPT study. In addition, the effect in terms of reduced FoH was explored by increasing and decreasing the base case value in the MM780G AHCL group by 20% (the 20% decrease was based on 6-month data from ADAPT) and a further analysis was performed in which it was assumed that there was no FoH benefit in either arm. Sensitivity analyses were performed around the rate of SHEs, one analysis was performed in which the incidence of SHE 1 (i.e., events requiring third-party assistance) was set to 64 per 100 patient-years in the is-CGM+MDI arm in line with findings from the real-world observational FUTURE study 16 and the rate in the MM780G AHCL arm was set to 0 per 100 patient-years.
A second analysis was also performed in which the SHE 1 rate was set to 64 events per 100 years in the is-CGM+MDI arm and 32 events per 100 patient-years in the MM780G AHCL arm. In addition, the base case analyses assumed 100% adherence to device use, and a sensitivity analysis was performed in which adherence was assumed to be 95.8% in the MM780G AHCL arm (based on time spent in Auto Mode in the ADAPT trial) and 87.3% in the is-CGM+MDI arm (based on time that the sensor was worn in the ADAPT trial).
Sensitivity analyses were also performed around utility values for diabetes-related complications (Supplementary Table S1) and around HbA1c progression approaches, treatment costs, discount rates, and time horizon. Probabilistic sensitivity analysis was also performed.
Results
Base case analyses
Summary findings from the base case analyses across all six countries are presented in Table 4. Overall, the findings were relatively consistent across all six countries included in the analysis. In people failing to achieve good glycemic control with is-CGM+MDI, the use of MM780G AHCL was projected to improve quality-adjusted life expectancy compared with is-CGM+MDI. In all six countries, the incremental gain in quality-adjusted life expectancy with MM780G AHCL was 2.27 quality-adjusted life years (QALYs) (Table 4). Total lifetime mean direct costs were consistently higher with MM780G AHCL across all settings, with the incremental lifetime cost for the AHCL group ranging from EUR 26,735 in Austria to EUR 99,896 in Italy.
Summary of Base Case Findings
Conversion to EUR is based on the average exchange rate for 2022.
ICUR, incremental cost–utility ratio; QALY, quality-adjusted life year.
Across the six countries included in the analysis, the ICURs for MM780G AHCL versus is-CGM+MDI in this patient population ranged from a low of EUR 11,765 per QALY gained in Austria to a high of EUR 43,963 per QALY gained in Italy, with the findings for the remaining countries all lying within this range (Table 4).
Higher lifetime treatment costs were the main contributor to the overall higher lifetime direct costs in the AHCL arms (Supplementary Table S2). For example, in Sweden, mean lifetime treatment costs in the MM780G AHCL arm were more than four times higher (SEK 1,587,134 [EUR 148,425 based on average exchange rate for 2022]) compared with the is-CGM+MDI arm (SEK 381,948 [EUR 35,719]). However, over the 40-year time horizon, the higher treatment costs were partially mitigated by lower complication costs owing to a lower incidence of long-term complications in the MM780G AHCL arms (Supplementary Table S2). For example, the use of AHCL was projected to lead to a 38% decrease in the cumulative incidence of eye complications compared with is-CGM+MDI as well as a 19% decrease in the cumulative incidence of cardiovascular complications and stroke (data not shown).
Sensitivity analyses
A broad range of sensitivity analyses were performed to determine the effects of changing assumptions around input parameters, treatment effects and costs and the trends in the findings of the sensitivity analyses were also relatively consistent across all six countries (Table 5). In general, the results were particularly sensitive to the time horizon of the analysis and to changes in assumptions around the cost of the AHCL system and consumables as well as the anticipated effect of reduced FoH on quality of life.
Summary Findings of Sensitivity Analyses
Conversion to EUR is based on the average exchange rate for 2022.
FoH, fear of hypoglycemia; PSA, probabilistic sensitivity analysis.
If the time horizons of the analyses were reduced to 10 years (vs. 40 years in the base case), the ICURs across all six countries increased substantially. This was postulated to be at least partly attributable to the long-term nature of the disease process as well as older age and progression of other physiologic risk factors contributing to the risk of complications. The benefits of MM780G AHCL in terms of the reduction in the cumulative incidence of long-term complications such as cardiovascular disease and renal disease were more evident over longer time horizons. As anticipated, the findings were also sensitive to the acquisition cost of the MM780G AHCL system, with the ICUR increasing substantially if the cost of the MM780G AHCL system was increased (Table 5). For example, in Italy, if the acquisition cost of MM780G AHCL was increased by 20%, the ICUR increased substantially to EUR 75,781 per QALY gained.
Conversely, if a 20% decrease in acquisition cost was assumed, this led to the ICUR decreasing substantially to EUR 12,144 per QALY gained. The ICURs were also sensitive to the projected utility benefit associated with reduced FoH. If no benefit in terms of reduced FoH was assumed in either treatment arm, the ICUR increased substantially in all settings included in the analysis. Probabilistic sensitivity analysis was also performed (Table 5).
Cost–utility acceptability curves and scatterplots are shown in Figures 1 and 2, respectively.
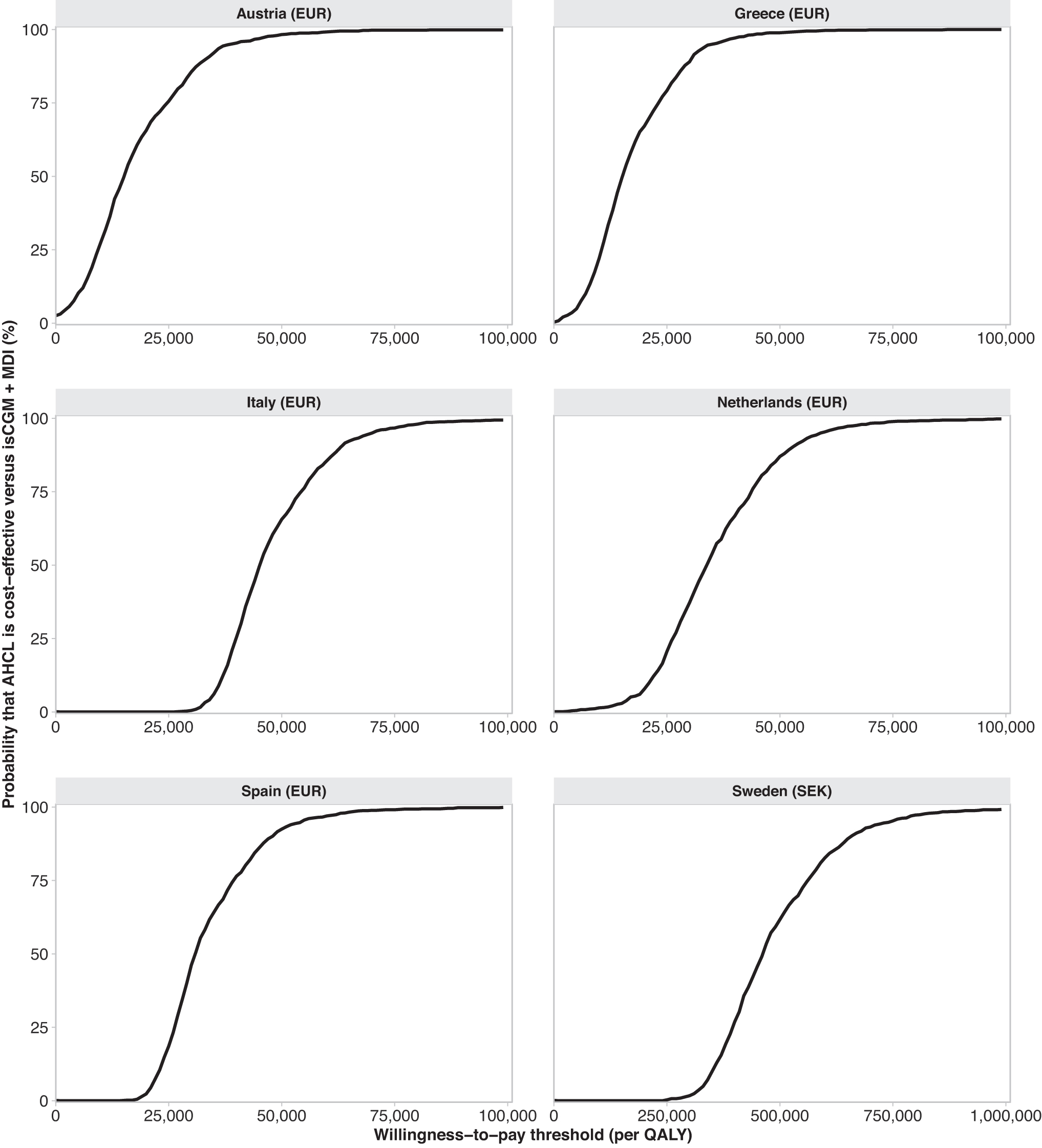
Cost–utility acceptability curves across all countries. AHCL, advanced hybrid closed-loop; is-CGM, intermittently scanned continuous glucose monitoring; MDI, multiple daily insulin injections; QALY, quality-adjusted life year.

Cost–utility scatterplots across all countries.
Discussion
Overall, the results of the analyses performed here across six different countries suggest that, in people living with T1D not achieving glycemic targets with is-CGM+MDI, the use of the MM780G AHCL system was projected to lead to an incremental gain in mean quality-adjusted life expectancy more than two QALYs across all six countries. The gain in quality-adjusted life expectancy was driven largely by the large decrease in HbA1c in the MM780G AHCL arms, based on the findings of the ADAPT trial. Over a time horizon of 40 years, this treatment effect was projected to reduce the cumulative incidence of diabetes-related complications and increase the time alive and free-of-any complications by up to 3 years in the MM780G AHCL arms compared with is-CGM+MDI arms (data not shown).
However, mean lifetime treatment costs were consistently higher in the MM780G AHCL arms and the high acquisition costs associated with devices such as AHCL have been acknowledged as a barrier to uptake. 5 The findings reported here suggest that the improvement in long-term outcomes, and the subsequent reduction in complication costs, associated with the use of the MM780G AHCL system, can at least partly mitigate the higher treatment costs.
Willingness-to-pay thresholds may vary substantially from country to country. For example, in Sweden, the threshold value has been estimated to range from approximately EUR 80,000–135,000 per QALY gained (approximately SEK 855,000–1,444,000 based on the average exchange rate for 2022), while in The Netherlands, the corresponding range has been estimated at EUR 10,000–80,000 per QALY gained, with the threshold being influenced by the severity of the condition. 17,18 In addition, in Austria, Greece, and Spain, there is no formal threshold value for cost-effectiveness. 19 –21 In the analyses presented here, the ICURs ranged from a low of EUR 11,765 per QALY gained (Austria) to a high of EUR 43,963 per QALY gained (Italy).
In both Greece and Austria, the ICURs were below EUR 20,000 per QALY gained, the ICUR for Spain was EUR 29,718 per QALY gained, and in both The Netherlands and Sweden, the ICURs were below the higher bands of threshold values for these settings. 17,18 The ICUR reported in the Italian analysis was higher than those seen in other settings, but nevertheless was under EUR 50,000 per QALY gained.
Of note, the analyses presented here were conducted from a payer perspective, which therefore considered only direct costs. If the findings were considered from the societal perspective, which also include indirect costs associated with lost productivity, the ICUR ranged from EUR 6170 per QALY gained for Austria to EUR 36,816 per QALY gained for Italy. In addition, the overall trends in the sensitivity analyses were relatively consistent across all six countries. In particular, the cost-effectiveness of the MM780G AHCL system was strongly influenced by the time horizon of the analysis, such that over a short-term time horizon (10 years), AHCL would be unlikely to be considered cost-effective. However, sensitivity analyses also showed that the cost-effectiveness of AHCL remained relatively robust despite changes in assumptions around the efficacy, costs of complications, HbA1c progression approach, and the utility values used.
It should also be noted that, as shown in Table 3, the costs associated with treating and managing long-term complications varied considerably across the different countries included in the analyses. For example, the cost associated with the treatment of a myocardial infarction ranged from a low of EUR 4977 in Greece to a high of EUR 13,399 in Austria. Despite these cost differences, the use of AHCL relative to is-CGM+MDI was associated with cost-savings in all countries in terms of long-term complications avoided or delayed (Supplementary Table S2). Differences in costs may also be compounded by different methodologies used across different costing studies, slightly different payer perspectives, and differences in the cost components falling in scope (e.g., whether diagnostic tests are included).
These differences should not adversely affect the validity of analyses in any given country setting and indeed, conversely, idiosyncrasies in country-specific cost collection methodologies are often driven by the aspiration to enhance the relevance and applicability to a given payer perspective. These differences may, however, limit the validity of comparisons of findings across different geographies.
The analysis presented here is the first cost–utility analysis of MM780G AHCL versus is-CGM+MDI to utilize clinical input data from a long-term RCT. Previous analyses have been based on clinical data sourced from short-term and/or nonrandomized studies. Nevertheless, the findings presented here are consistent or better than those from previous analyses examining the cost–utility of AHCL versus is-CGM+MDI in Greece and Sweden, which assumed a more conservative effect due to the lack of direct comparison provided by the ADAPT study. 22,23 Despite the robust nature of the clinical input data utilized here, it is important to note that the generalizability of the findings is limited to people living with T1D not achieving glycemic targets while on is-CGM+MDI (the baseline HbA1c of the simulated patient population was 9.04% [75.3 mmol/mol]).
The analysis does not examine health economic outcomes in those people who are able to achieve glycemic targets with is-CGM+MDI or those with baseline HbA1c value between target levels and 9%. However, a sensitivity analysis in people with a baseline HbA1c of 8% suggested that the use of AHCL versus is-CGM plus MDI was also associated with clinical benefits and slightly higher ICURs relative to the base case analyses but still likely to be considered cost-effective. Further clinical studies are needed to examine the incremental benefits and cost-effectiveness of AHCL versus is-CGM+MDI in groups with different baseline HbA1c values. In addition, the advantages of AHCL systems in those who maintain good HbA1c control are likely more related to quality of life and a reduction in the everyday burden of disease management, which is not readily quantifiable using the CDM.
The present analysis is associated with limitations. First, projections were made over 40 years based on 6-month HbA1c data (although recent data have shown that the HbA1c effect with AHCL is sustained over 12 months 24 ); however, this is a common limitation inherent in all long-term cost–utility analyses. Second, a discount rate of 3% per annum was used across all countries for the base case analyses, rather than the discount rates recommended in national guidelines, although a discount rate of 3% is recommended in Austria, Italy, Spain, and Sweden. 25 –28 Although this methodology deviates from the recommended methodologies for analyses in Greece and The Netherlands, it permits better comparability of the findings across the different geographies. Where necessary, sensitivity analyses were performed using the recommended discount rates.
Overall, the findings of the analyses suggest that, in people living with T1D and not achieving HbA1c target levels while on is-CGM+MDI, the use of AHCL over a long-term time horizon is projected to provide an incremental benefit of over two QALYs, thereby corresponding to a substantial gain in quality-adjusted life expectancy. Given the substantial long-term clinical benefits that are projected in this specific group of people, it is likely that many payers would consider the higher acquisition costs associated with AHCL to be a justifiable expense, particularly given the potential future economic implications associated with the projected lower rate of long-term complications. In conclusion, the MM780G AHCL system is likely to be considered to represent good value for money for people living with T1D across all of the countries included in the analysis.
Footnotes
Authors' Contributions
J.J.: writing and review and editing (equal); M.I.B.: writing, review and editing (equal), data curation (equal), formal analysis (lead), conceptualization (equal), and methodology (equal); A.Z.O.S.: writing, review and editing (equal), data curation (equal), formal analysis (lead), conceptualization (equal), and methodology (equal); S.d.P.: writing, review and editing (equal), conceptualization (equal), and methodology (equal); J.S.-P.: writing, original draft (lead); R.F.P.: writing, review and editing (equal), data visualization (lead), and data curation (equal); O.C.: writing, review and editing (equal), conceptualization (equal), and methodology (equal).
Author Disclosure Statement
J.J. has been a lecturer/member of the scientific advisory board in the following companies: Abbott, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Insulet, Medtronic, Nordic InfuCare, Novo Nordisk A/S, and Sanofi. M.I.B., A.Z.O.S., S.d.P., and O.C. are current employees and shareholders of Medtronic. J.S.-P. and R.F.P. are current employees of Covalence Research Ltd., which has received consulting fees from Medtronic related to the preparation of this article.
Funding Information
Funding relating to the preparation of this article was provided by Medtronic International Trading Sàrl.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.