
Abstract
Objectives:
Reaching optimal postprandial glucose dynamics is a daily challenge for people with type 1 diabetes (T1D). This study aimed to analyze the postprandial hyperglycemic excursion (PHEs) and late postprandial hypoglycemia (LPH) risk according to prandial insulin time and type.
Research Design and Methods:
Real-world, retrospective study in T1D using multiple daily injections (MDI) analyzing 5 h of paired continuous glucose monitoring and insulin injections data collected from the connected cap Insulclock® . Meal events were identified using the rate of change detection methodology. Postprandial glucometrics and LPH (glucose <70 mg/dL 2–5 h after a meal) were evaluated according to insulin injection time and rapid (RI) or ultrarapid analog, Fiasp® (URI), use.
Results:
Meal glycemic excursions (n = 2488), RI: 1211, 48.7%; UR: 1277, 51.3%, in 82 people were analyzed according to injection time around the PHE: −45 to −15 min; −15 to 0 min; and 0 to +45 min. In 63% of the meals, insulin was injected after the PHE started. Lower PHE was observed with URI versus RI (glucose peak-baseline; mg/dL; mean ± standard deviation): 106.7 ± 35.2 versus 111.2 ± 40.3 (P = 0.003), particularly in 0/+45 injections: 111.6 ± 40.2 versus 118.1 ± 43.3; (P = 0.002). One third (29.1%) of participants added a second (correction) injection. The use of URI and avoiding a second injection were independently associated with less LPH risk, even in delayed injections (0/+45), (−36%, odds ratio [OR] 0.641; confidence interval [CI]: 0.462–0.909; P = 0.012) and −56% (OR 0.641; CI: 0.462–0.909 P = 0.038), respectively.
Conclusions:
URI analog use as prandial insulin reduces postprandial hyper- and hypoglycemia, even in delayed injections.
Despite the technical and pharmacological advances in the last decades, a high percentage of people with type 1 diabetes (T1D) do not reach the recommended glycemic goals. Insufficient diabetes control translates into a higher risk of long-term complications, and reduced quality of life and mortality. The T1D Exchange registry showed that 70% of people with T1D maintained suboptimal HbA1c levels. 1 The HbA1c average was 8.4% in the whole cohort and 9% in adolescents, suggesting a critical influence of treatment adherence on glycemic control results.
People with T1D depend on insulin treatment, which is also fundamental in around 25% of the T2D population. 2 Socioeconomic factors, treatment complexity, and fear of hypoglycemia affect insulin therapy adherence. 3,4 Errors in insulin administration before meals represent a barrier to reaching optimal glycemic control. They include bolus omissions and delays. Low insulin adherence negatively influences quality of life and is associated with increased morbidity, mortality, and hospitalization due to acute complications. 5
Insulin regimens, particularly when they require multiple daily injections (MDI), represent a heavy burden. 6 Daily dose adjustments are challenging due to the multiple variables included in the decision-making process: glucose levels and trends, meal content and type, physical activity, among others. Missed and late boluses worsen glycemic control. 5,7 However, they are often unnoticed in clinical practice due to the lack of information conveyed from people with diabetes to their caregivers. Traditionally, the clinical guidelines recommend administering rapid insulin (RI) before meals. 8 Only in the case of young children or people for whom it is difficult to accurately predict the food that will be eaten at a meal, it can be advisable to wait to administer the prandial insulin after the meal. Manufacturers recommend injecting second-generation “ultrarapid” insulins––URI––at the start of a meal or within 20 min, 15 min before in the case of RI analogs, and 30–45 min for human regular insulin. 8 –10 Boluses after ingestion and excessive corrections cause difficult-to-manage initial hyperglycemia and late hypoglycemia, which impact the physical and mental health of people with diabetes. 11
Maintaining high glycemic variability in the long term favors the development of endothelial dysfunction and cardiovascular events. 12
Previous studies confirmed that the timing of prandial insulin bolus is critical in diabetes management. 8 It translates into clearly different postprandial glucose dynamics, affecting both postprandial hyperglycemic excursions (PHE) and late postprandial hypoglycemia (LPH) risk. 13 However, those studies were done in a laboratory setting (such as in pharmacokinetic/pharmacodynamic studies), or were based on self-reported data on the dose and time of insulin injections. 6,14
Some digital devices potentially transforming diabetes management are connected insulin pens and caps, integrated with continuous glucose monitoring (CGM) sensors. 15 They track the dose and time of insulin injections and can set reminders to avoid omissions or delays. Both the user and the health care professional can access a complete view describing the relationship between the timing and dose of insulin and the postprandial glucose dynamics. 16
Although it is still advisable to take the prandial bolus before food intake by at least 15 min, 13 it is difficult to expect that in real life.
New second-generation rapid (“ultrarapid”) insulins can improve postprandial dynamics even when they are injected after the meal has started, reducing both the risk of immediate HPE and LPH. 17 –19 However, these results should be confirmed and quantified in a real-life setting.
In the last decades, the focus for analyzing the effectiveness of RIs has been on the postprandial hyperglycemic excursion and, therefore, in the first 2 h after injection. The underlying reason being the known cumulative effect of high glucose levels on the risk of long-term diabetes complications. Therapeutic diabetes education has also prioritized immediate postprandial monitoring. Often people with diabetes inject additional (correction) insulin doses to correct postprandial peaks immediately. 11 In clinical practice, overcorrection is a frequent cause of LPH due to the “stacking insulin effect.” 20
Insulclock® is a small insulin pen cap that records the date, time, duration, and dose of injections for optimal insulin delivery. 21 The Insulclock app integrates these parameters with other relevant information, including glucose levels from CGM devices or glucometers, food intake, or physical activity. Data collected can be reviewed by the patient and shared with the health care provider to monitor trends and patterns. Our recent multicentric randomized controlled trial showed the positive effects of the Insulclock system on glycemic control and variability, adherence to insulin treatment, and quality of life in people with T1D and insufficient control. 22
This study aimed to analyze the PHE and LPH risk according to time and type of prandial insulin injection using the data from real-world system users (see Article Highlights under Supplementary Information for details).
Research Design and Methods
Design
Real-world, retrospective study analyzing anonymous data derived from the same electronic Insulclock database for the six participating centers throughout Spain (Hospital General de Segovia, Segovia; Cruces University Hospital, Barakaldo; Hospital Arquitecto Marcide, Ferrol [A Coruña]; Hospital Universitario Central de Asturias, Oviedo; Hospital Universitario 12 de Octubre, Madrid; and Hospital Universitario Infanta Sofía, San Sebastián de los Reyes). At initiation of Insulclock use, written informed consent was obtained from each participant allowing Insulcloud S.L. to collect his/her data and use the anonymized and tabulated data for scientific purposes. The study was conducted following the ethical principles of the Declaration of Helsinki. Before any study-related activities, the Research Ethics Committee of the Hospital General de Segovia, Segovia, Spain, approved the study.
Population and database
Meal excursions from consecutive T1D participants starting to use the connected insulin pen cap Insulclock 21,22 from January to June 2022 were analyzed. Only glycemic excursions started with a glucose level between 70 mg/dL (3.9 mmol/L) and 250 mg/dL (13.9 mmol/L) and with 5-h data after a meal initiation was included. The Glucose Rate Increase Detector (GRID) algorithm was used to automatically detect meal glucose excursions through the rate of change of glucose from CGM data. 23 All patients were previously using CGM (Freestyle Libre2® ) as their usual diabetes care. The baseline and 5-h paired CGM and rapid-acting insulin data were collected from the database uploaded by the Insulclock system.
The meals detected were classified as breakfast when started between 6 and 9:59 h, lunch from 12 to 15:59 h, and dinner between 19 and 23:59 h.
Outcomes
The postprandial glucose dynamics were evaluated according to time periods around PHE start. Three time periods were defined: injections from 45 to 15 min before (−45/−15), 15 min before up to PHE start (−15/0), and from 0 to 45 min after the PHE start (0/+45). PHEs were described by the delta glucose (difference between baseline and postprandial peak), total area under curve (AUC) of glucose and glucose AUC over 180 mg/dL (10 mmol/L). The LPH was defined as events of glucose levels under 70 mg/dL (3.9 mmol/L) lasting more than 15 min and % of the time below the range of glucose 70 mg/dL (3.9 mmol/L) (TBR70), occurring 2–5 h after a meal.
After confirming that the final sample of evaluable meal events included almost the same proportion of events and subjects using either rapid (lispro, aspart, and glulisine) (RI) or “ultrarapid” analog (Fiasp®, Novo Nordisk, Denmark) (URI), and the clinical and baseline glucometrics were almost identical, postprandial glucometrics and LPH risk were evaluated according to the insulin type used.
The administration of a second injection (correction doses) 1–5 h after the first insulin dose was also evaluated.
Statistical analyses
Statistical analyses were performed using the SPSS software, version 25.0 (Chicago, IL). The level of statistical significance was set at P < 0.05. Continuous variables were described by the mean and standard deviation (SD), when normally distributed, or by the median, interquartile range (IQR), when not normally distributed. Categorical variables were described by the number of valid cases and percentages. Comparisons of proportions and/or frequency distributions were performed with the Chi-square test, Kruskal–Wallis, or the analysis of variance (ANOVA) test, as appropriate, with the post hoc Bonferroni correction.
Logistic regression models were used to assess predictors of LPH <70 mg/dL (3.9 mmol/L) depending on timing of insulin injection, second injection (correction insulin), and URI use. Simple regression models were first performed, and those variables reaching statistical significance were included in the multivariable logistic regression model. In the multivariable model, a P-value <0.05 was considered significant. Those variables with a variance inflation factor >5 were removed from the models. The goodness of fit for logistic regression models was evaluated with the Hosmer–Lemeshow test. A poor fit is considered if the significance value is <0.05, while a larger P-value closer to 1 indicates a good logistic regression model fit.
Results
Population
A total of 2784 PHEs were included and 2488 were finally evaluable, from 82 participants, 40.9 ± 13.1 years old, 44 (58.7%) male, 40 participants were using URI and 42 RI analogs.
Table 1 summarizes the clinical characteristics and baseline glucometrics of the whole included population and split by the type of RI used.
Demographic and Clinical Characteristics and Glucometrics Data of Study Participants
Comparison between RI analog users and second-generation (“ultrarapid”) analog users' characteristics.
CV, coefficient of variation; GMI, glucose management indicator; RI, rapid insulin; SD, standard deviation; TAR, time above range; TBR, time below range; TIR, time in range.
The meal events are quite evenly distributed along the entire subject's sample and into the groups compared. The median of events by subject in the whole sample was 29 (interquartile range [IQR] 25%–75% 23–38; min 13, max 55). In the URI and RI users the data were quite similar: 31 (IQR 25%–75% 24–38.25; min 13, max 55) versus 26 (IQR 25%–75% 22.25–37.25; min 14, max 49).
Postprandial glycemic dynamics according to prandial insulin injection timing
The distribution of injection time rate was: −45/−15 injections in 14% (n = 348), −15/0 injections in 24% (n = 612), and 0/+45 in 63% (n = 1528).
Figure 1 describes the postprandial glucose dynamics depending on the prandial insulin injection time.
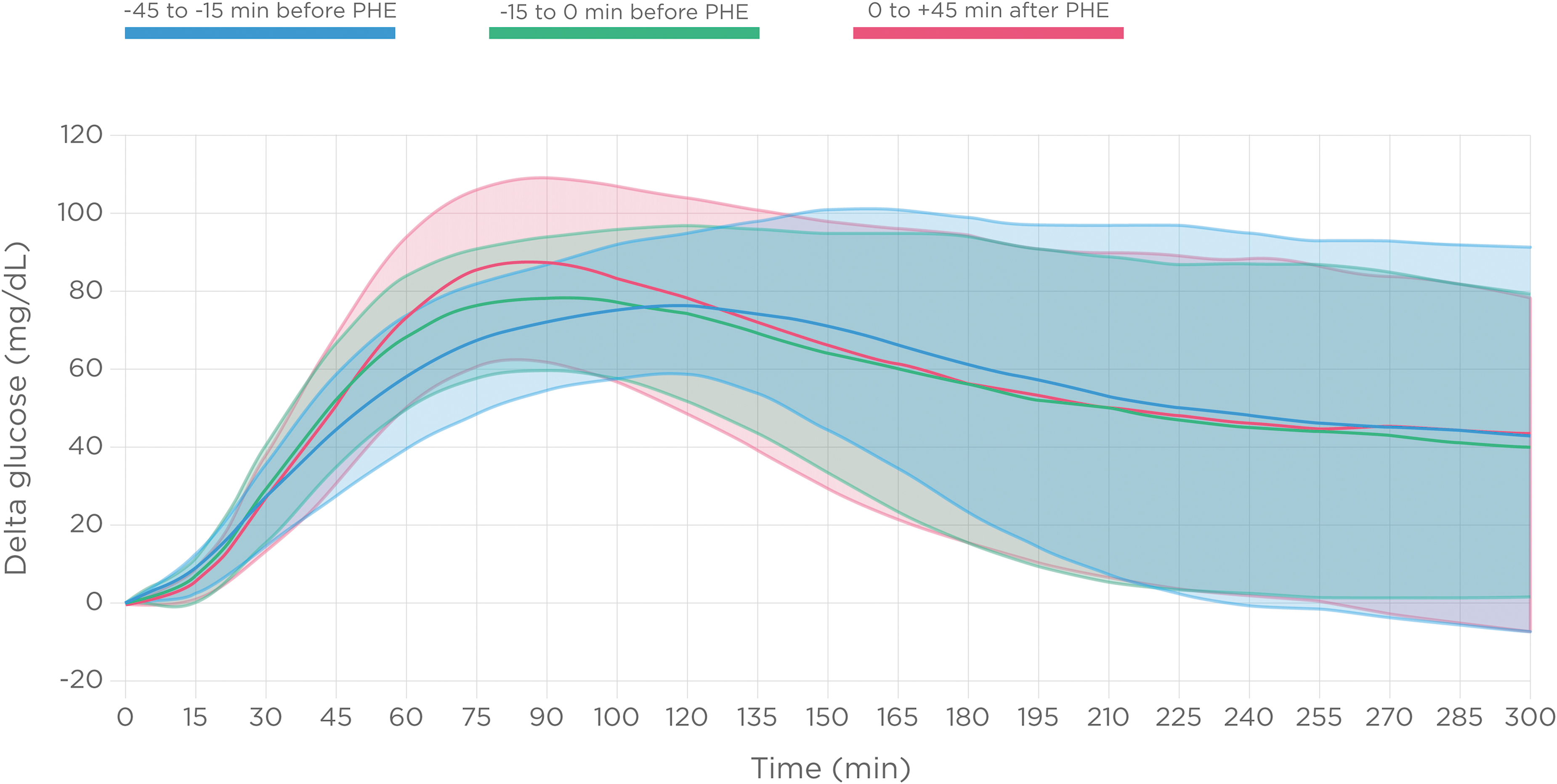
Postprandial glucose dynamics (glucose relative change from baseline) depending on the prandial insulin injection time. Delta glucose, postprandial peak-baseline; PHE, postprandial hyperglycemic excursion.
The total glucose AUC results showed statistically significant differences between groups, being higher in injections −15/0 min, median (IQR), mg/dL × h: 818.8 (688.4–960.2), 838.2 (706.4–1002.4), 793.4 (657.3–957.0), for −45/−15, −15/0, and 0/+45 injections, respectively; P < 0.0001).
It is interesting to underline that, globally, the PHE continued 5 h after meals, independently of the injection time, with glucose being on average 42 mg/dL (2.3 mmol/L) higher over baseline.
The distribution of meals during the day was: breakfast 725 (29.1%), lunch 989 (39.8%), and dinner 459 (18.4%).
Delta glucose of PHE was higher at lunch events (mean ± SD, mg/dL) (breakfast 106.3 ± 36.5, lunch 113.4 ± 40.1, dinner 102.3 ± 32.8; P < 0.0001).
Postprandial hyperglycemic excursions
Delta glucose (difference between postprandial peak and baseline) was higher in the 0/+45 group (mean ± SD, mg/dL): −45/−15 (n = 348), 101.8 ± 34.0; −15/0 (n = 612), 98.3 ± 29.8; 0/+45 min (n = 1528), 114.8 ± 40.2; (P < 0.001) (Supplementary Fig. S1).
The AUC of glucose over 180 mg/dL (10 mmol/L) results did not show statistically significant differences between groups, median (IQR), mg/dL × h: 323 (164–523); 357 (133–542); 393 (163–536); for −45/−15, −15/0, and 0/+45 injections, respectively; (P = 0.132).
Late postprandial hypoglycemia
The LPH rate increased in 0/+45 injections, n (%): −45/−15: 31 (8.9%); −15/0: 47 (7.7%); 0/+45: 171 (11.2%), (−15/0 vs. 0/+45 P = 0.014) (Supplementary Fig. S2).
The percentage of the time below range of glucose 70 mg/dL (3.9 mmol/L) (TBR70) showed similar results (Supplementary Fig. S3).
Analysis according to URI use
Approximately, the same proportion of participants/PHE in the study used URI (40 participants, 1277 PHE, 51.3%) or RI analogs (42 participants, 1211 PHE, 48.7%).
PHE with URI
Total PHE delta glucose was lower when URI was used compared with RI (mean ± SD; mg/dL): 106.7 ± 35.2 versus 111.2 ± 40.3 (P = 0.003).
The Figure 2 describes the postprandial glucose dynamics depending on the prandial insulin type on every injection time period.

Postprandial glucose dynamics depending on the prandial insulin type (URI- or RI- analogs) on every injection time period: injections from 45 to 15 min before PHE start
Slightly lower PHE delta glucose was observed with URI versus RI in 0/+45 injections (mean ± SD; mg/dL), −45/−15: 102.2 ± 32.2 versus 101.2 ± 36.7 (P = 0.738); −15/0: 96.6 ± 29.6 versus 99.9 ± 29.9 (P = 0.192); and 0/+45 injections: 111.6 ± 40.2 versus 118.1 ± 43.3; (P = 0.002) (Fig. 3).
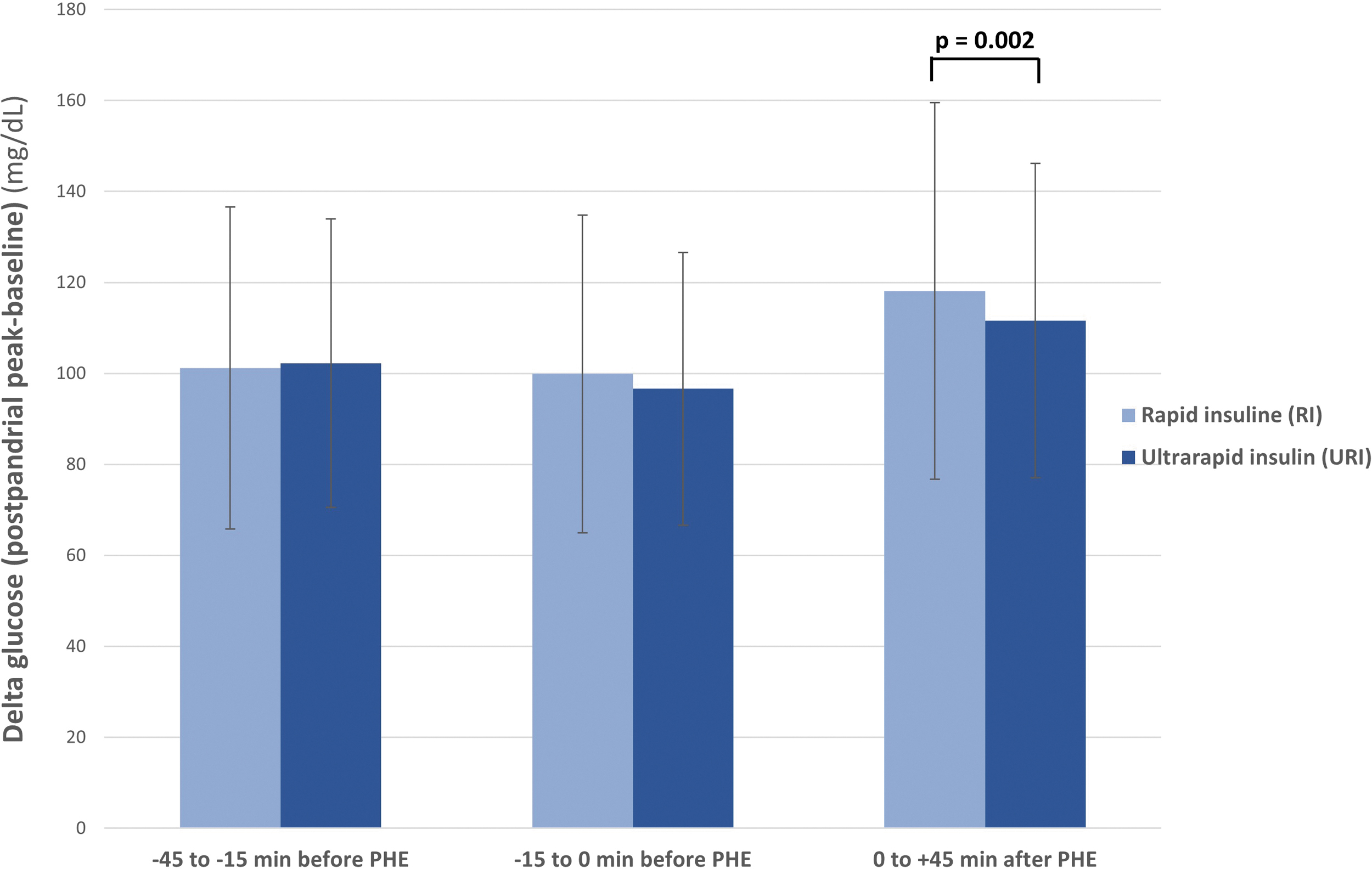
Delta glucose (postprandial peak-baseline) of PHE with URI versus RI analogs, at every injection time.
LPH with URI
URI use was associated with a lower LPH rate in the delayed, 0/+45, injections, URI versus RI, n (%), −45/−15: 20 (9.5%) versus 11 (8.0%), (P = 0.0703); −15/0: 18 (6.4%) versus 29 (8.8%), (P = 0.288); and 0/+45: 71 (9.1%) versus 100 (13.4%), (P = 0.007) (Fig. 4).

LPH (2–5 h after prandial injection) events (%), according to the use of URI versus RI analogs, at every injection time. LPH, late postprandial hypoglycemia.
Analysis according to second insulin (correction dose) use
One third (29.1%) of participants added a second injection of insulin one to 5 h after the first dose.
Statistically significant differences were detected regarding the rate of a second dose administration depending on the timing of first prandial insulin administration, being the higher rate in earlier injections, n (%): −45/−15: 124 (35.6%); −15/0: 194 (31.7%); 0/+45: 407 (26.6%); (P = 0.001).
There was not a statistical difference in the second insulin doses rate according to the type of insulin used (P = 0.294).
Delta glucose of PHE was not different between those using or not a second insulin injection (mean ± SD; mg/dL): No (n = 1763) 108.6 ± 37.7 versus yes (n = 725) 109.7 ± 38.1; (P = 0.494). The analysis by total (0–300 min) AUC of glucose (mg/dL × h) showed that it was slightly higher in the events with a second (correction) dose, median (IQR): No (n = 1763) 796.1 (663.2–959.2) versus yes (n = 725) 824.2 (697.1–980.4); (P = 0.003).
The LPH rate was different depending on the second insulin (correction) doses, being higher in early (−45/−15) injections when a correction dose was added. Yes versus no second injection, n (%), −45/−15: 17 (13.7%) versus 14 (6.3%), (P = 0.029); −15/0: 9 (4.6%) versus 38 (9.1%), (P = 0.071); and 0/+45: 42 (10.3%) versus 129 (11.5%), (P = 0.582) (Fig. 5).
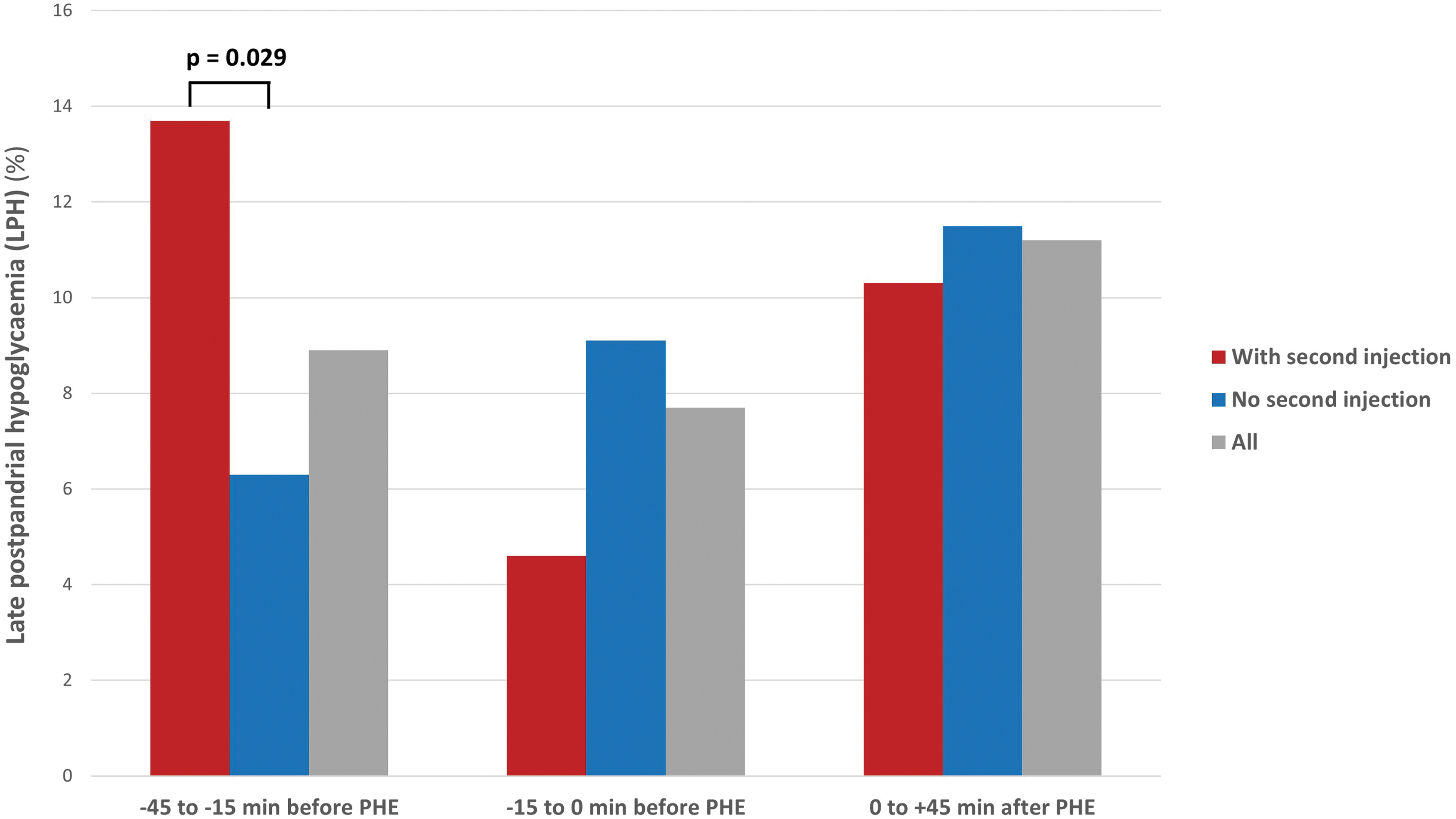
LPH (2–5 h after prandial injection) events (events of glucose <70 mg/dL lasting more than 15 min) rate (%), according to the use of second (correction) insulin doses or not, at every injection time.
Multivariable analysis
The multivariable logistic regression models, including timing of injection, use of a second injection, and insulin type, confirmed the use of URI was independently associated with a reduced risk of events of LPH <70 mg/dL (3.9 mmol/L), even on delayed injections (0/+45), by 36% (odds ratio [OR] 0.641; confidence interval: 0.462–0.909; P = 0.012).
In the same way, multivariable logistic regression models, including timing of injection, insulin type, and PHE delta glucose, confirmed that the use of a second injection was independently associated with an increased risk of events of LPH <70 mg/dL (3.9 mmol/L), mainly in the earlier injections (−45/−15) by 47%, (OR 1.468; 1.124–1.916; P = 0.005), where they were more frequently injected.
Figure 6 summarizes the effect of insulin type and second insulin doses on the rates of LPH events in every time period, differentiating the event proportion depending on the use of URI and correction doses.
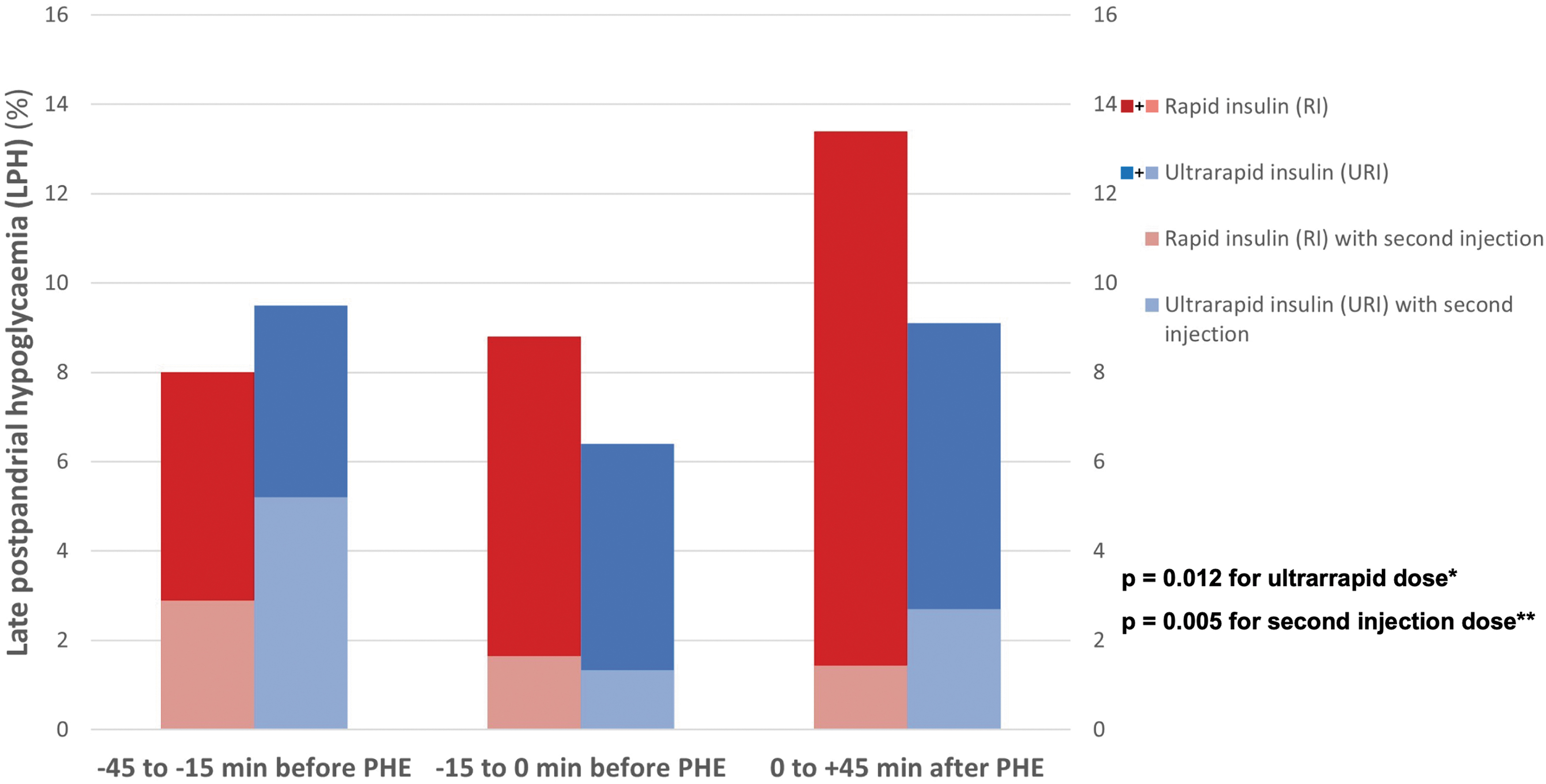
The effect of insulin type and second insulin doses on the LPH (2–5 h after prandial injection) rate (events of glucose <70 mg/dL lasting more than 15 min) in every time period, differentiating the event proportion depending on the use of URI versus RI analogs and correction doses. *Refers to the results of the multivariable logistic regression models, including the timing of injection, use of a second injection and insulin type, confirming the use of URI was independently associated with a reduced risk of events of LPH <70 mg/dL (3.9 mmol/L) by 36% (OR 0.641; CI: 0.462–0.909; P = 0.012). **Refers to the model, including the timing of injection, insulin type, and PHE delta glucose, confirming that the use of a second injection was independently associated with an increased risk of events of LPH <70 mg/dL (3.9 mmol/L) by 47%, (OR 1.468; 1.124–1.916; P = 0.005). CI, confidence interval; OR, odds ratio.
Conclusions
Adjusting the dose and timing of prandial insulin to the meal composition represents a main task and burden in the daily life of people with T1D. 24 Assessment and counseling on this issue are also a major daily challenge for health care providers. The access to CGM technology put light on the whole postprandial glucose dynamics picture. However, in a real-life basis, the analysis is very complex because of the need to consider the exact moment of injection and the frequent use of second insulin doses for correction. The users and caregivers of insulin pumps can have access to the exact time of boluses. However, only very recently, the availability of connected insulin pens and caps allow for the integration of CGM and insulin therapy data accurately.
In youths with T1D, a systematic review, including 13 studies published between 2002 and 2022 described that prandial insulin injected before a meal, particularly at breakfast, provides better postprandial glycemia and HbA1c without increasing the risk of hypoglycemia. 7
A large percentage of people with diabetes recognize not observing the timing for prandial insulin injection. In the current report, at least 63% of participants injected the prandial insulin after the meal started. This result is in line with a systematic literature review showing that 20%–45% reported mistiming insulin, which was associated with higher rates of hypoglycemia and HbA1c levels. 5 Peters et al., reported in a cross-sectional study of 21,533 T1D patients from the T1D Exchange registry that 31% of adults routinely injected their insulin during or after the meal. 25 Tamborlane and others also described that 31.6% of people with T1D and type 2 diabetes (T2D) delayed bolus insulin. The main weakness of this previous scientific evidence is the self-reported source of information. In our study, including only T1D adults, and with data automatically uploaded on a real-life basis, a significant majority (over 63%) of people with T1D administer prandial insulin after the meal starts. It is probably a much more accurate picture of reality. On the other hand, people with diabetes recognize it is difficult to change due to real-life circumstances. 6 Solutions are needed to reduce the consequences of injecting after starting a meal instead of insisting on the ‘canonical’ recommendation.
The insulin's pharmacokinetic/pharmacodynamic (PK/PD) profile compared with the glucose slope and duration after meals explains the difficulties in reaching optimal post meal glucose excursions. Insulins with a more similar PK/PD profile to the physiological (fast and short) would be better adapted to the effect of carb intake. It would improve the peak of the PHE and reduce the risk of LPH. Regular insulin is far from this profile. Subsequent RI analogs (lispro, aspart, and glulisine) have improved it with almost identical characteristics between them. 14 However, they are still far from that optimal profile and require administration before starting the meal. 8 The development of so-called “ultrarapid” insulin analogs aims to improve the results of first-generation analogs. Currently, two different “ultrarapid” or second-generation analogs, Fast-acting insulin aspart (Fiasp© ) and insulin Ultra-rapid lispro (URLi) have been internationally marketed. Currently, only the first one is available in Spain. Faster aspart contains two additional excipients, niacinamide and L-arginine. Niacinamide acts to increase subcutaneous blood flow to improve absorption, while the amino acid L-arginine serves as a stabilizing agent. 26 Recent phase 3 trials in T1D and T2D showed that Fiasp© , compared with conventional aspart, achieved lower HPE. 27 However, randomized controlled trials in T1D on MDI do not always show positive results regarding hypoglycemia. 19,28,29 The evidence from real-world studies using CGM is scarce and has not confirmed the benefits on hypoglycemia. 30 Our results, in a real-world study and using CGM, show a clear benefit by using Faster aspart insulin mainly reducing the LPH, even after delayed injections.
A study exploring the burden of mealtime insulin in T1D indicates that 57% of adults recognize needing extra insulin to correct additional food intake at least once a week and 7% daily. 6 In the present study, one-third of the participants injected a correction insulin dose, which was more frequent in earlier first injections, as expected. It increased the risk of LPH. A broader view of postprandial glucose dynamics focusing not only on the immediate hyperglycemia but also on late hypoglycemia risk should be requested to improve this behavior.
The present analysis did not only look at HPE but also LPH, and it confirmed the best balance of both endpoints for injections done 15–0 min before HPE. The relative importance of both events is difficult to assess. However, from an individual perspective, LPH is a source of disease burden, acute health risk, and one of the leading causes of hyperglycemia due to overcorrections. 11
The large sample, real-world source, CGM-based, and automatically tracked insulin data methodology are the strengths of the study. However, it can have limitations. Meal content is not analyzed and could modify the analysis. The GRID methodology limits the description to hyperglycemic excursions; then meals following insulin injections not causing a glucose increase are not included. But these are extremely unusual situations. Some other factors can explain that some meal events were not captured. Real-world evidence studies reported that at least 11% of people using CGM Freestyle Libre did not reach the 70% of sensor use requested by the clinical guidelines, 31 and up to 40% of users delay the sensor change by more than 24 h. 32 It means those subjects can lose up to one-third of complete meal events CGM records. Only excursions starting with a glucose level between 70 and 250 mg/dL were included. Finally, bolus omissions are quite frequent in this population. Our previous randomized controlled trial using Insulclock in a T1D population described up to 28 boluses missed every month. 3 Additionally, we must understand that we are detecting glucose excursions by CGM sensors in interstitial fluid not the meal start itself. There is a known lag time between the glucose detected in interstitial fluid and glucose in the blood, particularly in rapid changing periods. 33 Moreover, another physiological delay exists from food ingestion to blood glucose appearance. Some previous studies described both lags to be about 10 min each, on average. 34 Then, all the times in the study should be increased by 10–20 min when a clinical recommendation is given regarding optimal insulin injection time before meals start. A possible objection could be about the absence of an analysis by insulin dose. However, the study research work hypothesis starts by assuming that the dose selection is made depending on the carbohydrate counting and carbohydrate/insulin ratio previously set for every subject, as per standard of care.
In conclusion, new second-generation rapid (“ultrarapid”) insulins can improve postprandial dynamics even when administered with the meal started, reducing both the risk of immediate postprandial hyperglycemia and delayed postprandial hypoglycemia. URI should be a therapeutic consideration in individuals who delay their insulin boluses and who do not achieve recommended glycemic targets.
Footnotes
Acknowledgments
The authors acknowledge the editorial assistance of Nicole Quinn, Always English S.L. The study concept and design were developed, and the data collection, analysis, and interpretation performed, thanks to the unconditional efforts of all the investigators.
Authors' Contributions
F.G.P. designed and supervised the study, researched data, and wrote the article. C.A., D.B., E.M.T., S.G., E.F.R., L.C., and P.P. researched data and reviewed the article. S.R.V., H.B., X.V., J.J.P.G., and L.R.V. analyzed data and reviewed the article.
Author Disclosure Statement
F.G.-P. has taken part in advisory panels for Insulcloud S.L., Sanofi, and Novo Nordisk; has received research support from Sanofi, Novo Nordisk, Boehringer Ingelheim Pharmaceuticals and Lilly; and has acted as a speaker for Sanofi, Novo Nordisk, Boehringer Ingelheim Pharmaceuticals, AstraZeneca Pharmaceuticals LP, Bristol-Myers Squibb Co. and Lilly. C.A. has received research support from Sanofi, Novo Nordisk, Boehringer Ingelheim Pharmaceuticals and Lilly and has acted as a speaker for Sanofi, Novo Nordisk, Boehringer Ingelheim Pharmaceuticals, AstraZeneca Pharmaceuticals LP, and Bristol-Myers Squibb Co. E.F.-R. has acted as a speaker for Novo Nordisk, Lilly, and AstraZeneca Pharmaceuticals. L.C. has acted as a speaker for Sanofi, Novo Nordisk, Boehringer Ingelheim Pharmaceuticals, AstraZeneca Pharmaceuticals LP, and Lilly. P.P. has received research support from Novo Nordisk, and has acted as a speaker for Sanofi, Novo Nordisk, Boehringer Ingelheim Pharmaceuticals, AstraZeneca Pharmaceuticals LP, and Lilly. E.G.F. has taken part in advisory panels for Abbott, Mundipharma, and Novo Nordisk; has received research support from Novo Nordisk; and has acted as a speaker for Sanofi, Novo Nordisk, Boehringer Ingelheim Pharmaceuticals, AstraZeneca Pharmaceuticals LP, Lilly, Novartis, Abbott, Dexcom, Mundipharma, and Almirall. S.A. has acted as a speaker for Amgen, Abbott, Dexcom, Sanofi, Novo Nordisk, Novartis, Roche, Boehringer Ingelheim Pharmaceuticals, AstraZeneca Pharmaceuticals LP, and Lilly. R.C. declares that she has received consultancy fees from Novo Nordisk and speakers' fees or support for attending meetings or research from Novo Nordisk, Lilly, Sanofi, Roche, Medtronic, and Novalab-Air Liquide. The remaining authors have no conflicts of interest to disclose.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Information
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.