
Abstract
Objective:
To assess the clinical impact of flash glucose monitoring (FGM) systems on fear of hypoglycemia (FoH) and quality of life in adults with type 1 diabetes mellitus (T1DM).
Methods:
Prospective quasi-experimental study with a 12-month follow-up. People with T1DM (18–80 years old) and self-monitoring by blood capillary glycemia controls were included. The FH15 questionnaire, a survey validated in Spanish in a comparable study population, was used to diagnose FoH with a cutoff point of 28 points.
Results:
A total of 181 participants were included, with a FoH prevalence of 69% (n = 123). A mean reduction in FH15 score of −4 points (95% confidence interval [−5.5 to −3]; P < 0.001) was observed, along with an improvement in quality of life (EsDQOL-test (Diabetes Quality of Life, Spanish version), −7 points [−10; −4], P < 0.001) and satisfaction with treatment (Diabetes Treatment Satisfaction questionnaire, self-reported version [DTSQ-s] test, +4.5 points [4; 5.5], P < 0.001). At the end of the follow-up, 64.2% of the participants saw an improved FoH intensity, compared to 35.8% who scored the same or higher. This improvement in FoH status was associated with a higher time-in-range at the end of the follow-up (P = 0.003), as well as a lower time spent in hyperglycemia (P = 0.005). In addition, it was linked to participants with a high baseline FoH levels (P < 0.001) and those who were university degree holders (P = 0.07).
Conclusions:
FGM is associated with an overall reduction of FoH in adults with T1DM and with an increase in their quality of life. Nevertheless, a significant percentage of patients may experience an increase of this phenomenon leading to clinical repercussions and a profound impact on quality of life.
Introduction
Hypoglycemia is defined as blood glucose levels below 70 mg/dL, with a high incidence among people with type 1 diabetes m
The substantial impact of hypoglycemia on both the physiological and psychological aspects of individuals with diabetes may contribute to the emergence of atypical coping mechanisms in response to these occurrences, potentially giving rise to the phenomenon referred to as “pathological fear of hypoglycemia” (FoH). 4 While fear, perceived as an adaptive response to potential threatening situations, is imperative for averting hypoglycemic episodes and effectively managing precarious scenarios, FoH is characterized by a persistent, recurring, and disproportionate trepidation of encountering such events, resulting in a pronounced detrimental effect on the quality of life for diabetic patients. 5 In certain instances, FoH can lead to the development of avoidant behaviors that impede the optimization of glycemic control, constituting a health care concern that frequently eludes detection in routine clinical practice. 6
Some of the strategies proposed for the therapeutic approach to FoH in patients with T1DM range from psychoeducational interventions based on a behavioral approach to the implementation of technological systems applied to diabetes that optimize metabolic control and reduce the frequency of hypoglycemia. 4 In this regard, interstitial glucose monitoring devices (Flash—flash glucose monitoring [FGM]—or continuous—CGM) have been shown to improve overall glycemic control in patients with T1DM, particularly in terms of reducing hypoglycemia compared to self-monitoring through capillary blood glucose controls (SMBG). 7 Among the advantages of these systems is their ability to predict the expected trend in glucose level evolution and the possibility of setting audible alarms to prevent adverse glycemic events. 8
While some studies have reported a reduction in the FoH phenomenon associated with the use of FGM systems, 9 both their impact, measured as a primary outcome variable, and the behavior in patients specifically experiencing this disorder, remains unclear to date. We propose this study with the aim of analyzing the impact of FGM systems on the FoH phenomenon in individuals with T1DM.
Materials and Methods
Study design and participants
We conducted a prospective quasi-experimental study with a 1-year follow-up in a single center. Adult patients, aged 18 to 80 years, who had a confirmed diagnosis of T1DM with at least 1 year of evolution, were on intensive insulin therapy, and performed self-monitoring with SMBG, were included. Patients without reading or writing comprehension skills, those who were already using interstitial glucose monitoring systems before the study commenced, those with a follow-up period of less than 12 months, and those lacking the ability to understand Spanish were excluded. Recruitment was carried out systematically and consecutively in the Endocrinology and Nutrition Department of our hospital during the years 2020–2021 as part of a strategic plan to implement FGM systems in the T1DM population, without following any specific prioritization criteria. The FGM systems used were the “FreeStyle Libre 2” model by Abbott Laboratories.
Variables
The main study variable was the reduction in FoH after 1 year of using FGM systems, measured using the “FH15” questionnaire (Supplementary Data S1). This survey was originally validated in Spanish within a population with T1DM that had sociodemographic characteristics mirroring those of our study, thus ensuring the reproducibility of the results. The validated cutoff point of 28 points was used for the assessment of FoH. 10
In addition, participants were asked to complete the Diabetes Quality of Life Test (EsDQOL), 11 the Diabetes Treatment Satisfaction Test (DTSQ-s), 12 and the Clarke Test. 13 The Clarke test is a questionnaire used to detect hypoglycemia unawareness in individuals with DM and insulin treatment. It consists of eight items that assess aspects such as the symptoms perceived during a hypoglycemic event, the frequency of these events, and the glucose thresholds at which the patient experiences symptoms. Responses to each question can be categorized as normal (A) or abnormal (R), with the presence of three or more abnormal responses indicative of hypoglycemia unawareness. 14
In our research, we have followed the analysis of the Clarke test scores proposed in subsequent studies (Sepúlveda et al. 15 ), in which it was observed that separately analyzing items 3 and 4 of the Clarke test allows for a specific evaluation of the frequency of severe hypoglycemic events reported by subjects, while the remaining items (1, 2, 5, 6, 7, 8) assess aspects directly related to hypoglycemic awareness (Supplementary Data S1).
To assess glycemic control, changes in glycated hemoglobin (HbA1c) were investigated, and metrics related to SMBG were recorded at baseline. Variables from the Ambulatory Glucose Profile (AGP) reports were programmed for 14 days in month 1 and 12 days during the follow-up period.
Intervention
Before the implementation of the FGM devices, baseline measurements of all clinical variables were taken, and questionnaires were completed. The implementation of FGM took place as part of a structured and concise diabetes education program specifically designed to train participants to use these devices. This program comprised two 2-h sessions conducted by the same health care professional—a nurse with expertise in advanced diabetes practices. Participants were instructed in fundamental aspects of managing FGM devices, including interpreting trend arrows, configuring alarms, and self-application procedures. In addition, participants were given the choice to attend sessions either in person or remotely. Our group has previously published the clinical outcomes of this intervention, providing detailed information about its characteristics. 16
Statistical analysis
The required sample size was estimated at 161 patients for bilateral hypothesis testing, with 95% confidence and 80% statistical power, based on the results of FoH reduction after FGM use measured with the FH15 survey reported in a previous work by our group (minimally relevant reduction: 4 points). 16
Univariate hypothesis testing was conducted using Student's t-test and the Mann-Whitney U test (nonparametric) for independent quantitative variables. For related quantitative variables (before-after comparisons), the Student's t-test for paired samples or its nonparametric alternative, the Wilcoxon test, was used. For dichotomous qualitative variables, the chi-square test and Fisher's exact test were used. The influence of baseline FH15 score on the variations observed in the rest of the questionnaires was evaluated using simple linear regression models. We considered the difference between the baseline and the 12-month follow-up in each metric (ΔScore) as the dependent variable, and the baseline score in FH15 was used as the independent variable.
Predictor variables for FoH improvement (defined as obtaining a score in FH15 at 12 months lower than the baseline) were identified using a binary logistic regression model. The independent variables were selected using the stepwise method from among those who showed a significance level of P < 0.15 in the univariate analysis. The final number of included variables was determined based on the criteria of greater parsimony and better discrimination capacity, with a reference to an area under the curve (AUC) >0.75 in the ROC curve analysis. The efficacy of the model was assessed using the Hosmer-Lemeshow test.
A significance level of P < 0.05 was considered (two-tailed hypothesis testing). The statistical analysis software used was SPSS v.26 (IBM Statistics).
Ethics
The study was conducted in accordance with the ethical standards proposed in the Declaration of Helsinki, under the approval of the Research Ethics Committee of the Hospital Universitario Virgen Macarena of Seville (code 1959-N-22).
Results
Patients, baseline characteristics and glycemic control
A total of 231 participants were initially identified as potential candidates to participate in the study. One hundred and eighty-one participants were eventually included. Fifty participants were excluded based on the following criteria: prior experience in the use of FGM devices, lack of literacy skills, and inability to follow-up (Supplementary Data S2). The clinical and sociodemographic characteristics of the excluded patients did not differ from those of the study group (data not shown).
The prevalence of FoH (FH15 score ≥28) was 69% (n = 123). A higher mean age was observed in patients with FoH compared to those without (P = 0.039), along with a higher percentage of women (P = 0.035), a longer history of DM (P < 0.001), older age at diagnosis (P = 0.015), and a higher prevalence of a history of severe hypoglycemia (P = 0.019) (Table 1).
Baseline Characteristics of the Sample, Divided into Cohorts
Data reported by 104 participants out of 181.
The CSII system used in all cases was the Medtronic (Dublin) “Minimed 640G” model, using SMBG.
Baseline blood glucose data obtained from SMBG.
CSII: subcutaneous insulin infusion system.
95% CI, 95% confidence interval; ADA, American diabetes association; BMI, body mass index; DM, diabetes mellitus; FH, pathological fear of hypoglycemia; HbA1c, glycated hemoglobin; MDI, multiple insulin doses; SMBG, self-monitoring through capillary blood glucose controls.
The use of FGM was associated with a mean reduction in HbA1c (%) of −0.34% (95% confidence interval [CI] [−0.48 to −0.2], P < 0.001), with no differences between patients with and without FoH. AGP glucometric levels were similar in both groups in the first and last months of follow-up, including the percentage of time in hypoglycemia, as well as the number of such events and their average duration (Supplementary Data S3).
Impact of FGM on FoH and quality of life
A decrease in the median FH15 score of −4 points (95% CI [−5.5 to −3]; P < 0.001) was observed, along with an increase in diabetes-related quality of life (EsDQOL −7 points, 95% CI [−10 to −4], P < 0.001) and the satisfaction with treatment (DTSQ-s +4.5 points, 95% CI [4 to 5.5], P < 0.001) (Table 2 and Fig. 1). When analyzing the experience of severe hypoglycemia using items 3 and 4 of the Clarke test, a reduction of −1 point (95% CI [−1.5 to −1], P < 0.001) was observed. No variations were found in items related to unawareness of hypoglycemia (remaining five items, P = 0.89), nor in the global score (P = 0.199, data not shown). The baseline FH15 score level served as a predictor variable of the variations in EsDQOL in the linear regression analysis, both in its total score and by subsections (Table 2).
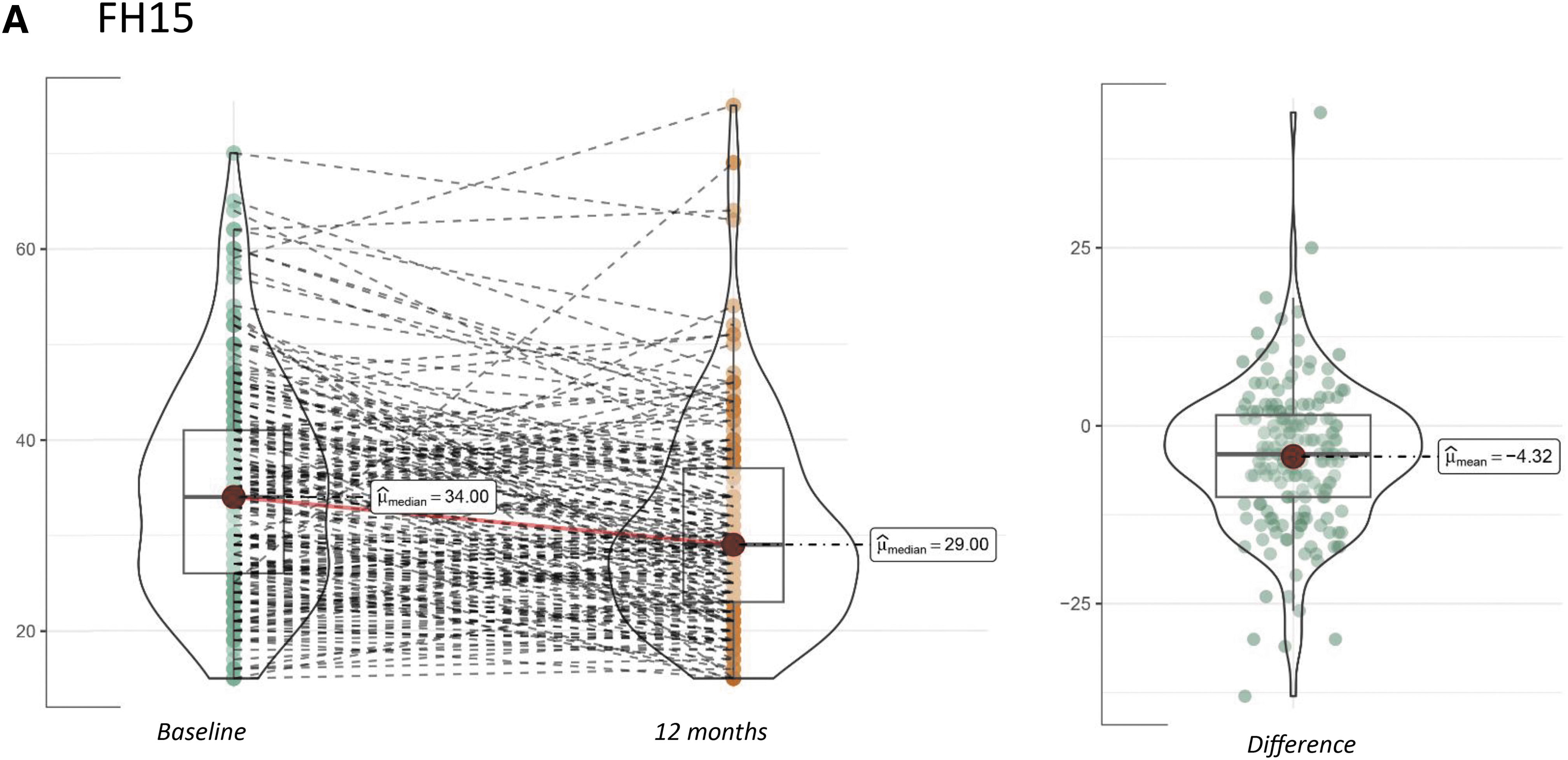
Variation in psychosocial questionnaire scores between baseline and the end of the 12-month follow-up. All analyzed individuals are shown with individual points and connecting lines in the left-hand graphs. On the right, the distribution of the differences is displayed.

Variation in Psychosocial Questionnaire Scores from Baseline (Preflash Glucose Monitoring) to the End of Follow-Up (12 Months)
Univariate analysis using T-Student for paired data. The significance level for the variation in scores (ΔS) between baseline and 12 months is shown.
Using linear regression models, the extent of the influence of baseline FoH scores (baseline FH15) on score variations in the rest of the questionnaires is shown. The models follow the equation: “y = Beta*x”; where [y = ΔS], and [x = baseline FH15 score].
Dif: difference; Q3: quartile 3, 75th percentile; Q1: quartile 1, 25th percentile.
DTSQ-s, Diabetes Treatment Satistfaction Questionnaire, self reported version; EsDQOL, Diabetes quality of life questionnaire, spanish version; FGM, flash glucose monitoring; FH15, fear of hypoglycemia 15 survey; IQR, interquartile range.
Modification of the FoH phenomenon associated with FGM use
We investigated the number of participants in whom the FoH phenomenon decreased to a score <28 points on FH15 (significantly low scores for FoH). This analysis was performed on 179 participants (out of the 181 included) who correctly completed both the baseline (pre-FGM) and final (12-month) surveys.
Despite the observed reduction in the median scores of FH15 at the end of the follow-up (−4 points), when analyzing the effects at an individual level, a weak effect was evident in the majority of participants, with some cases showing an increase in scores compared to the baseline level (Fig. 1). With the aim of delving into the different patterns of FoH variation, we conducted a subgroup analysis of the study cohort based on the direction of change in FH15 scores at the end of the follow-up, disaggregated by FH15 < or ≥28 points at baseline.
We observed that in patients with high FoH (≥28 points) at baseline, n = 58/121, patients (48%) decreased their FH15 scores although they did not drop below the cutoff point of 28 points. This group had significantly higher baseline scores than the second group (n = 34/121, 28%) that improved to fall below 28 points, resulting in a change of diagnosis to low FoH. A third subgroup of n = 29/121 patients (24%) had scores equal to or higher than the baseline score, indicating persistence or worsening of FoH, despite starting from a similar pre-FGM situation as the patients who improved and changed the diagnosis to low-FoH (Fig. 2A).
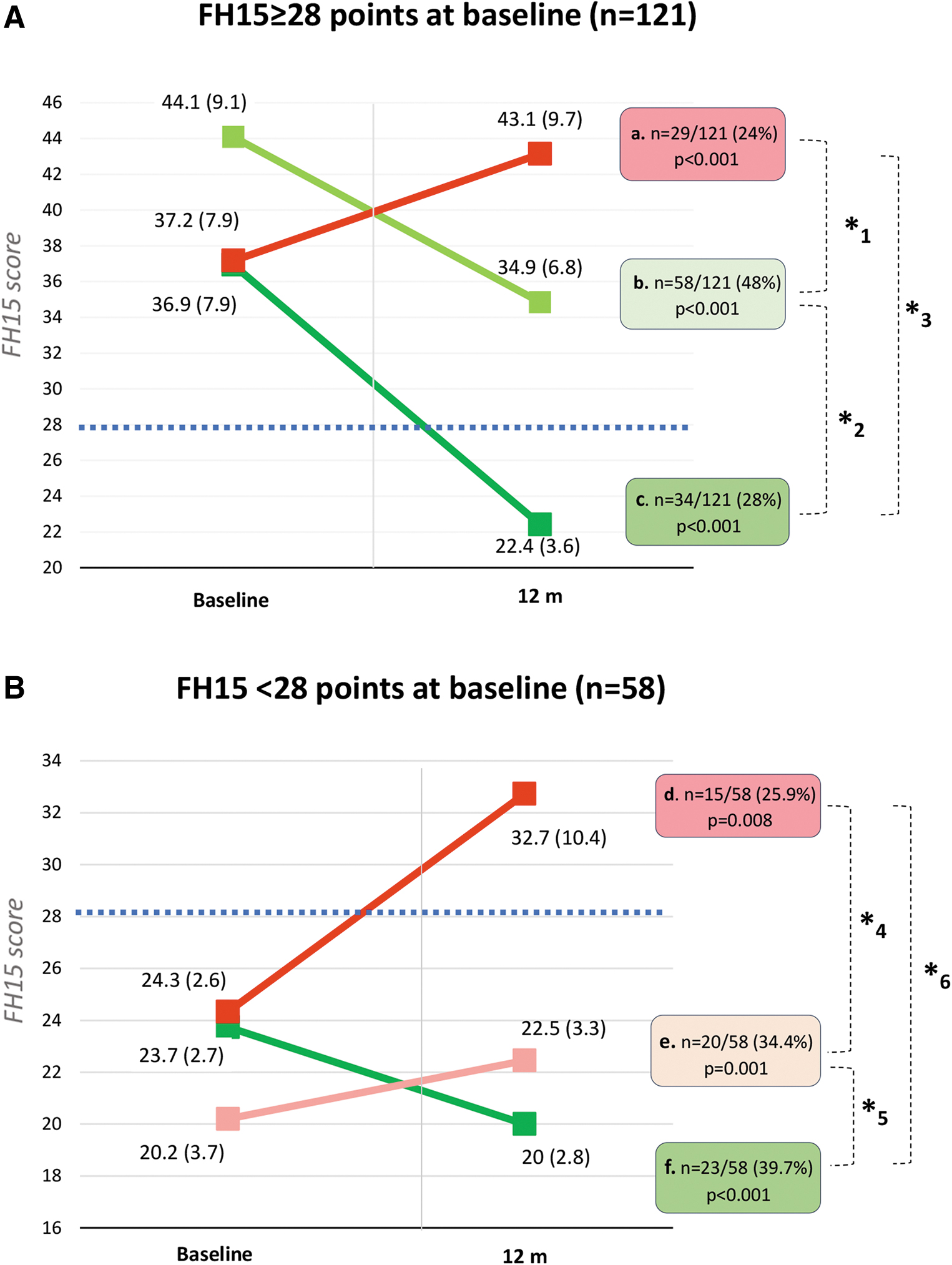
Variation in FH15 scores. The results are displayed in two groups selected based FH15 scores at baseline (FH15 cutoff point = 28 points, marked on the charts with a dashed blue line). In red, participants with an increase in FoH at the end of the follow-up
When analyzing patients with low FoH scores at baseline (<28 points), it was observed that n = 23/58 participants (39.6%) improved their FH15 scores, while n = 20/58 (34.5%) either maintained or increased their scores without surpassing the 28-point cutoff. Similar to what was described in the group with high FoH at baseline, n = 15/58 (25.9%) increased their FH15 scores and transitioned to high FoH status, despite starting with similar baseline scores as those who improved their results. In contrast, those who worsened without changing their diagnosis began with significantly lower scores than those who did switch to FoH (Fig. 2B).
To identify determinants of FoH improvement or worsening associated with the use of FGM, between-group differences were analyzed based on the variation in FH15 (Supplementary Data S4). The percentage of patients who improved their scores (without differentiating between scores greater than or less than 28 points) was 64.2% (n = 115/179).
Both patient subgroups, those who reduced their FoH scores at the end of follow-up, and those who did not, started with similar baseline HbA1c levels. After 12 months of follow-up, the group that reduced their FoH scores demonstrated lower HbA1c levels compared to those who achieved equal or higher scores (difference: −0.3% [−0.6; −0.07], P = 0.013). In terms of AGP variables, the group with improved FoH had a higher time in range at the end of follow-up (+9.5%, 95% CI [3.3 to 15.7], P = 0.003) and spent less time in hyperglycemia ≥181 mg/dL (Time Above Range I+Time Above Range II) (−9%, 95% CI [−16 to −3], P = 0.005). These differences were already noticeable from the first month of device use.
Other variables that were associated with an improvement in FoH were the presence of baseline FoH (odds ratio [OR]: 0.2, 95% CI [0.1 to 0.4], P < 0.001), the diagnosis of diabetic retinopathy (OR: 0.5, 95% CI [0.2 to 1.1], P = 0.064), and holding a university degree (OR: 0.5; 95% CI [0.2 to 1.1], P = 0.077). In the multivariate logistic regression model, the presence of baseline FoH, holding a university degree, and spending less time in hyperglycemia ≥181 mg/dL after 12 months of follow-up demonstrated a high discriminatory ability for the improvement of FoH associated with the use of FGM (AUC: 0.788 [0.7; 0.9], P < 0.001) (Supplementary Data S4).
Discussion
The present study assesses the impact of FGM on FoH in individuals with T1DM in real-life settings and is the first of its kind as far as we know. 17 Some authors have reported a FoH prevalence of 40%–70%, 18 which is consistent with the findings in our study (68%). These data highlight the need to deepen our understanding of this condition, aiming at identifying determinants for the development of FoH, as well as exploring the impact of the different strategies used in its management.
We found that the use of FGM was associated with an improvement in FoH after 1 year of follow-up, with a median reduction of −4 points in the FH15 score. Similarly, we observed a significant improvement in the scores of the quality-of-life test and its subcategories, as well as in satisfaction with diabetes treatment. These results are consistent with those reported in the literature for similar interventions in an adult population with T1DM. 19 Some factors such as easier access to glycemia values compared to SMBG, the possibility of setting alarms to prevent the development of hyper- or hypoglycemia events, or the availability of trend arrows (among others) could justify these results. 20 Regarding the FoH specifically, Kłak et al. recently published a meta-analysis focusing on FoH reduction outcomes after the implementation of continuous glucose monitoring systems, demonstrating their superiority over SMBG. 9
The reduction in the frequency and intensity of hypoglycemia is considered one of the main mediators in decreasing FoH. 4 Numerous studies have demonstrated a close relationship between the use of FGM and a decrease in hypoglycemia. 7,21 Unfortunately, in our study, we could not specifically evaluate the reduction of hypoglycemia time, as we did not perform a blinded follow-up before FGM implementation. However, we can highlight some outcomes that indirectly suggest a decrease in hypoglycemic events after the use of these devices. A significant decrease was observed when analyzing the items related to the perception of severe hypoglycemia in the Clarke test (items 3 and 4). However, no significant changes were observed in the rest of the items, which assess inadvertent hypoglycemia.
The data indicate a decrease in subject-reported severe hypoglycemic episodes, suggesting an apparent decrease also in the percentage of hypoglycemic events. In this regard, the presence of a history of severe hypoglycemia was one of the main risk factors for FoH found in our study (in addition to female sex, age, or duration of diabetes), in accordance with the literature. 22 –25 A reduction in severe hypoglycemic events could have contributed significantly to the perceived decrease in FoH in our study. However, these results should be interpreted with caution, as the specific reduction in severe hypoglycemic episodes was not specifically assessed in our study.
FoH improvement was more frequent in patients with a diagnosis of diabetic retinopathy and high baseline FH15 scores. These results are consistent with the idea that enhancing confidence in self-care and decision-making in diabetes is particularly relevant for individuals starting from a more vulnerable situation. 26
Another novel aspect of this research is the fact that, despite the average reduction in the overall FH15 scores, a high percentage of participants (71.9%) still had scores indicative of FoH. Those participants started from higher baseline scores than those who did. However, unexpectedly, we found that a significant subgroup of patients had worsening scores compared to their pre-FGM situation. From these results, it is possible to infer that, despite the mostly positive impact of FGM on the reduction of FoH, there is a non-negligible percentage of patients who experience a worsening of FoH and a decline in their quality of life associated with the use of these devices.
Despite the significant benefits associated with the use of these systems in terms of metabolic control and quality of life, there are barriers that may justify an increased emotional burden and anxiety in diabetes self-care for some patients, which could potentially affect hypoglycemia management. Some of these barriers include a lack of confidence in the device, interference from alarms at inconvenient times (such as during sleep or work), difficulty in understanding its use, or potential inaccuracy of measurements in specific situations. 27 On the contrary, managing the large amount of real-time information on glycemic control provided by these systems compared to SMBG may be perceived as overwhelming by some patients, as reported in parents of young children with T1DM. 28 The higher percentage of university education among patients who improved their FoH compared to those who did not improve reinforces this hypothesis.
In our study, we recorded a clinically significant decrease in HbA1c associated with the use of FGM (−0.34%), which is consistent with what has been reported in the published literature. 7 We found no association between the presence of FoH and elevated HbA1c levels, and there were no differences between groups in terms of AGP variables during follow-up. This lack of association has been previously reported by numerous authors, 29 –31 in contrast to previous studies where the presence of FoH was linked to the development of avoidance behaviors aimed at increasing hyperglycemic periods to decrease the likelihood of hypoglycemic events. 32,33 The results of our study suggest that the presence of FoH may translate into poorer glycemic control through the adoption of such behavioral alterations in only a subset of patients, but not consistently in all individuals with T1DM.
It is possible that the absence of systematic screening for FoH in adults with T1DM in routine clinical practice leads to a selection bias, with underdiagnosis in patients with good glycemic control who experience this phenomenon, and overdiagnosis in those with poorer control and in whom this or other causes of psychological distress are proactively identified.
On the contrary, although we did not find differences in metabolic control between groups, we did observe that the improvement of FoH in terms of FH15 score reduction, translated into better glycemic control outcomes, independently of baseline HbA1c level, and FoH intensity. These results support the theory of a global impact of the FGM systems on individuals with T1DM, showing that the reduction in HbA1c induced by these systems occurs simultaneously and in association with the reduction in FoH and improvement in quality of life. 17
Limitations
The study we have conducted has certain limitations that need to be considered. Firstly, it has not been possible to establish a control group for comparison with the observed results. We recognize that this limitation restricts the conclusions drawn, as it is challenging to confidently attribute the changes observed in FoH at the end of the follow-up solely to the use of FGM. We recognize that FoH is a complex phenomenon, in which there are many reasons why some people might continue to experience it even after having used FGM. In addition, it cannot be ruled out that the observed changes in questionnaire scores might have been influenced by a regression to the mean bias. Consequently, our findings should be validated through randomized and placebo-controlled studies.
Second, it was not possible to conduct a more precise assessment of the impact of FGM on glycemic control due to the absence of continuous monitoring data (blinded or professional monitoring) before the intervention. Consequently, we were unable to explore the degree of association between changes in FoH and the variation in the percentage of hypoglycemic events.
Third, the implementation of FGM devices took place within the context of a targeted educational intervention aimed at providing patients with fundamental knowledge of using this tool. To ensure uniformity in the intervention, all participants received identical two sessions from the same health care professional, using the same teaching materials. Even though the content of said intervention was specifically aimed at training patients in the technical aspects of device use, we recognize that this educational intervention may have contributed to the improvement of FoH.
Finally, the questionnaire used to measure the FoH (FH15) has not been validated in English. This fact could be a limitation when it comes to accurately reproducing these results in an English-speaking population. However, the questionnaire was originally validated in a population with similar sociodemographic and geographic characteristics to the study population, which guarantees the reproducibility of the results. 10 Moreover, the validation performed in Spanish, 10 Italian, 34 or Chinese 35 showed excellent internal consistency data, making it highly specific for evaluating the “fear” of hypoglycemia. In addition, unlike other FoH questionnaires, FH15 includes a cutoff point that allows the study of populations with a high incidence of this phenomenon.
Conclusions
The results of our study show that the use of FGM is associated with a general reduction in the FoH phenomenon, an improvement in overall quality of life and treatment satisfaction, as well as enhanced glycemic control in terms of HbA1c. Nevertheless, some patients may experience worsening in relationship to FoH, which should be comprehensively assessed in the context of clinical practice.
Footnotes
Acknowledgments
To Dr Ángel Vilches Arenas for his help regarding methodology and statistical analysis and to Alicia Muñoz Fernández for the translation and proofreading work.
Authors' Contributions
P.R.d.V.G.: term, conceptualization, methodology, formal analysis, investigation, and writing-original draft. C.M.R.: conceptualization, resources, and investigation. B.R.J.: data curation and visualization. L.H.S.: conceptualization, resources, and investigation. M.P.R.: data curation and visualization. E.T.d.C.: data curation and visualization. D.R-.A.: conceptualization and writing-review and editing. I.S.O.: conceptualization and writing-review and editing. Á.C.M.: data curation and visualization. M.A.M-.B.: term, conceptualization, methodology, formal analysis, investigation, and writing-review and editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data S1
Supplementary Data S2
Supplementary Data S3
Supplementary Data S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.