
Abstract
Objective:
Continuous glucose monitors (CGMs) used for type 1 diabetes management are associated with lower hemoglobin A1c. CGMs are not approved for inpatient use, when close glucose monitoring and intensive insulin management are essential for optimal health. Accuracy data from adult hospitalizations have been published, but pediatric data are limited.
Design and Methods:
This retrospective review of Dexcom G6 data from youth with type 1 diabetes during hospitalization assessed CGMs and matched (within 5 min) point-of-care (POC) and laboratory glucose values. Glucose values >400 and <40 mg/dL were excluded due to sensor reporting capabilities. Standard methods for CGM accuracy were used including mean absolute relative difference (MARD), Clarke Error Grids, and percentage of CGM values within 15%/20%/30% if glucose value is >100 mg/dL and 15/20/30 mg/dL if value is ≤100 mg/dL.
Results:
A total of 1120 POC and 288 laboratory-matched pairs were collected from 83 unique patients (median age 12.0 years, 68.7% non-Hispanic white, 54.2% male) during 100 admissions. For POC values, overall, MARD was 11.8%, that on the medical floor was 13.5%, and that in the intensive care unit was 7.9%. The MARD for all laboratory values was 6.5%. In total, 98% of matched pairs were within Clarke Error Grid A and B zones.
Conclusions:
Findings from our pediatric population were similar to accuracy reported in hospitalized adults, indicating the potential role for CGM use during pediatric hospitalizations. Additional research is needed to assess accuracy under various conditions, including medication use, as well as development of safe hospital protocols for successful CGM implementation for routine inpatient care.
Introduction
Diabetes technologies have advanced significantly over the past several decades. Continuous glucose monitors (CGMs) consist of subcutaneously inserted filaments that provide 7–14 days of continuous glucose levels. The use of CGMs in people with type 1 diabetes has independently been tied to significant improvements in hemoglobin A1c (HbA1c) levels when used in the outpatient setting for routine care. 1,2 Recent CGMs have received FDA approval for nonadjunctive use, 3 meaning the factory-calibrated sensors were deemed accurate enough to dose insulin without verification of blood glucose levels by fingerstick.
More recently, the development of hybrid closed-loop systems has changed the landscape of diabetes care by incorporating an insulin pump with a CGM and automatically adjusting insulin dosing based on CGM values. The approval of these devices was a significant advancement in diabetes care and lends to the accuracy of and trust in CGM devices.
The American Diabetes Association recommends that people with CGMs in the hospital be allowed to continue to wear the device as the importance of glycemic management during hospitalization has been well documented 4 ; however, CGMs are currently only FDA approved for outpatient use, and many adult and pediatric hospitals continue to require fingerstick glucose values for medical decision making. To date, CGM use and accuracy in the hospital setting are limited to mostly published data in adults with type 1 or type 2 diabetes.
The importance of CGM use in hospitalized patients was highlighted during the COVID-19 pandemic, when frequent glucose monitoring was essential to improving health outcomes; however, frequent point of care (POC) glucose testing was burdensome and created unnecessary exposure of hospital staff to the coronavirus. During the COVID-19 pandemic, the FDA issued enforcement discretion to expand the use of noninvasive glucose monitoring, which allowed for increased glucose monitoring capabilities and increasing the ability to provide appropriate glycemic management. 5
Many adult hospitals took advantage of this leniency and used CGM systems, especially in COVID-positive patients. 6 –9 Despite this expansion, pediatric hospitals have been less likely to allow CGM glucose data to replace fingerstick blood glucose monitoring and, therefore, there is limited data regarding accuracy of glucose sensors in hospitalized pediatric patients.
Research Design and Methods
This study was completed as a retrospective chart review. The study was approved by the Colorado Multiple Institutional Review Board.
Patients
Patients had a clinical diagnosis of type 1 diabetes and were active patients at the Barbara Davis Center at the University of Colorado. All patients had a hospital admission at the Children's Hospital Colorado within the previous 3 years. At the time of hospital admission, the patients were wearing their personal Dexcom G6 CGM device that was placed by the patient/family as part of their routine diabetes management before or during their hospitalization. The devices were functioning and collecting data at the time of hospitalization. Only patients with CGM data were used in this analysis.
The electronic medical record was used to obtain information on demographics, location of hospital admission, primary admission diagnosis, laboratory evaluations, and POC and laboratory glucose values.
Glucose monitoring
POC glucose monitor
The reference glucose value for this accuracy assessment was obtained using the POC glucose from the Nova Biomedical StatStrip, which has a mean absolute relative difference (MARD) of 6% 10 and was developed specifically for use in critically ill patients by measuring and correcting for clinical interference, including in pediatric hospital admissions. 11 POC glucose data were collected from the electronic medical record.
Continuous glucose monitor
The Dexcom G6 CGM was used for this analysis. The Dexcom G6 was FDA approved in 2018 for outpatient nonadjunctive use. This sensor is factory calibrated and, therefore, does not require daily calibrations; however, calibrations can be completed if necessary. In outpatient studies, the Dexcom G6 had an MARD of 7%–10%. 12 –14 This sensor was used for this study as it is the most commonly used sensor in our center's pediatric population. In addition, since each sensor brand has different outpatient accuracy, it was important to analyze only one sensor for the inpatient accuracy assessment. Sensor comma-seperated values data were obtained from the Dexcom Clarity cloud system.
POC:CGM and laboratory:CGM-matched glucose pairs
POC/laboratory and CGM values were matched if they occurred within 5 min of each other. In addition, for this analysis, any POC/laboratory values >400 mg/dL were excluded due to the Dexcom limitation of reporting only values between the ranges of 40 and 400 mg/dL, with values outside of this range not reported numerically.
Statistical analysis
Sensor accuracy was assessed by calculating the MARD. This is a standard method of accuracy assessment for fingerstick blood glucose and CGMs.
Clarke Error Grids are a form of analysis developed specifically for quantification of clinical accuracy of blood glucose values when compared with a reference glucose value. 15 Zone A consists of values within 20% of the reference sensor. Zone B consists of values outside of the 20% but would not result in inappropriate treatment. Zone C includes glucose values that may lead to unnecessary treatment. Zone D indicates potentially dangerous failure to detect hypoglycemia or hyperglycemia. Zone E indicates points that would result in erroneous treatment of hypoglycemia or hyperglycemia. Common use of Clarke Error Grids includes a calculation of the percentage of values within Zones A and B.
%15/15, %20/20, %30/30: This evaluation includes the calculation of the percentage of values within 15% (or 20% or 30%) of POC/laboratory glucose values that are >100 mg/dL and within 15 mg/dL (or 20 or 30 mg/dL) of POC/laboratory glucose values that are ≤100 mg/dL.
Results
Data from 83 unique pediatric patients with type 1 diabetes (median age 12.0 years, 54% male) during 100 unique hospital encounters were collected (see Table 1 for demographic data). Of the 100 encounters, 41 were due to diabetic ketoacidosis (DKA) requiring insulin infusion. A list of primary diagnosis is provided in Table 2.
Demographics (N = 83 Unique Patients)
HbA1c, hemoglobin A1c; IQR, interquartile range.
Admissions by Primary Diagnosis (N = 100 Inpatient Encounters)
DKA, diabetic ketoacidosis; URI, upper respiratory infection; UTI, urinary tract infection.
CGM accuracy
POC glucose value accuracy
Accuracy analysis was conducted in a total of 1120 matched pairs (Table 3). Matched pairs included POC glucose values between 40 and 400 mg/dL with a CGM value within 5 min of the documented POC value. The MARD across all matched pairs during pediatric hospitalizations was 11.8% (N = 1120). When location of admission was stratified by medical floor versus intensive care unit (ICU), the MARD was significantly better in the ICU (7.9% vs. 13.5%, P ≤ 0.01).
Accuracy Statistics
Zones refer to Clarke Error Grids.
Values include both medical floor and ICU.
ICU, intensive care unit; MARD, mean absolute relative difference.
The percentage of values within 15/15, 20/20, and 30/30 is summarized in Table 3. Around 50% of values were within 15/15, 60%–70% were within 20/20, and >80% were within 30/30.
To further quantify clinical accuracy and visualize the distribution of CGM values, we performed a Clarke Error Grid analysis with the matched POC:CGM pairs (Fig. 1). Of the total matched pairs (n = 1120), 64.2% fell within zone A (clinically accurate), 33.8% fell within zone B (benign errors), 0.7% fell within zone C (potential for overcorrection), 1.2% fell within zone D (failure to detect hypo- or hyperglycemia), and 0.1% fell within zone E (treatment error).
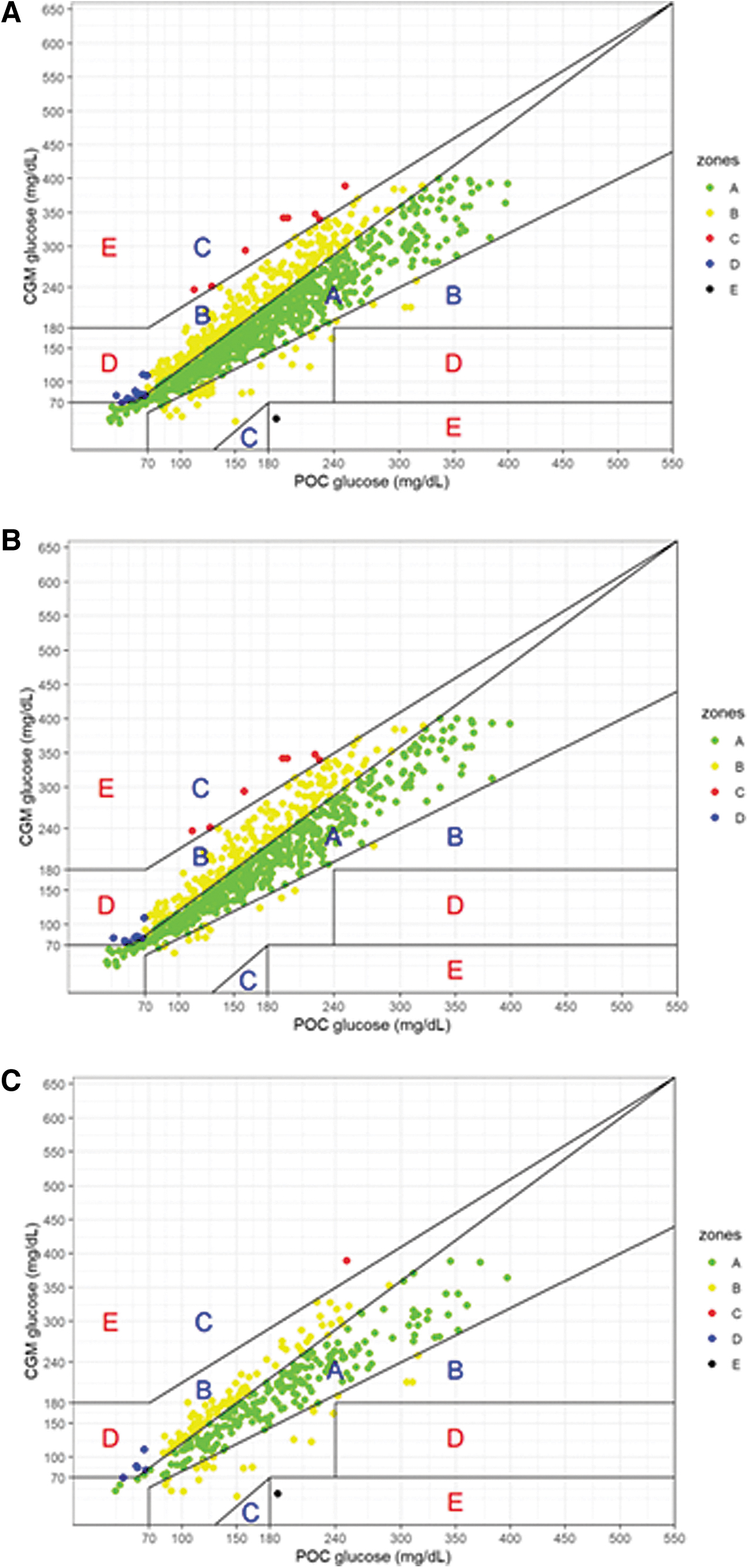
POC:CGM Clarke Error Grids by admission location.
For those admitted to the medical floor, 66.4% were in zone A, 31.7% were in zone B, 0.9% were in zone C, 1.0% were in zone D, and none were in zone E. For those admitted to the ICU, 59.2% were in zone A, 38.8% were in zone B, 0.3% were in zone C, 1.5% were in zone D, and 0.3% were in zone E. Therefore, ∼98% of values fell within zones A and B for all glucose values regardless of location of admission.
POC glucose values in hypoglycemia (<70 mg/dL) and hyperglycemia (250–400 mg/dL) with numeric matched CGM glucose values (excluding “low” and “high” CGM reported data) were additionally analyzed, though sample sizes were small. There were 42 matched pairs in hypoglycemia, with a MARD of 28.2% and 69% within zones A and B, respectively. Included in the analysis were five POC values <40. The four POC/CGM matched values are 36/43, 35/47, 39/51, 37/64, and 34/low. In total, 171 matched pairs in hyperglycemia had a MARD of 5.6% and 100% within zones A and B, respectively. Most variation in CGM values when POC glucose was <70 mg/dL was found in zone D, indicating that the sensor tended to read the glucose value higher than the POC value that was measured at the same time.
Laboratory glucose value accuracy
A total of 288 matched pairs with hospital laboratory and CGM glucose values were obtained from this data set (Table 3). The overall MARD was 6.5%. The location of admission MARD was not included due to fewer than 100 matched pairs existing from the ICU, therefore, increasing the potential to skew the results.
Conclusions
In this analysis, we demonstrated clinically acceptable accuracy of the factory-calibrated Dexcom G6 CGM in the pediatric hospital setting with similar or better accuracy findings to previously published analysis. Our overall POC MARD was 11.8%, on the medical floor the MARD was 13.5%, and in the ICU the MARD was 7.9%.
Although it may not be expected that the accuracy in the ICU is better than on the medical floor, it is possible that patients admitted to the ICU are less active and receiving fewer oral carbohydrates, therefore, reducing the glucose fluctuations and limiting the amount of time the CGM is lagging the blood glucose. When comparing CGM with laboratory glucose values, the MARD was even better at 6.5%, though the number of matched pairs was smaller and further subgroup analysis, including location of hospitalization, was not possible.
When assessing accuracy in the hypoglycemic range (POC values <70 mg/dL), we found that the accuracy decreased as expected, with the errors tending to result in CGM values higher than POC values. It is possible that these episodes could result in missed or delayed hypoglycemia detection, although the clinical scenario for these events was not able to be determined and may represent rapid changes in glucose and symptomatic POC testing. The POC values that were <40 and had a matched numeric CGM value <70 would have resulted in a CGM alarm for hypoglycemia (<70 mg/dL).
In the setting of hyperglycemia (250–400 mg/dL), the accuracy was very good with an MARD of 5.6% and 100% of values within clinically acceptable zones. These findings support the clinical safety of the CGM in the hospital; however, hospital-based protocols to ensure sensor safety and accuracy are important for using these devices routinely in the hospital setting for both adult and pediatric patients.
Our study has several limitations, including the retrospective study design. In this method, we rely on the accuracy of the documentation from the hospital record, including the timing of the glucose measurements, as errors in documentation of timing of values can significantly skew the results of the POC:CGM comparisons. As the blood glucose meters used in the hospital are linked, this is unlikely to contribute significantly to any errors in our calculations. In addition, as we were not placing the CGM sensor as part of the study, we were not able to determine the exact date and time of sensor insertion and, therefore, could not assess the accuracy based on sensor age.
This needs to be studied further as it is known that accuracy is lower in the initial days of sensor wear and this could impact use in the hospital setting when a sensor may be placed for medical management. This study design also does not allow for assessment of the clinical scenario associated with each POC glucose test. addition, although we had an overall large sample size (N = 1120), we had a small sample size of ICU (N = 343), and laboratory (N = 288) glucose values.
Small samples sizes can influence the MARD value in either direction, falsely more accurate or more inaccurate, and, therefore, may make interpretation difficult. And finally, the use of POC values as the reference is not ideal for device accuracy studies as the blood glucose meter (Nova Biomedical StatStrip at our hospital) itself has an MARD; however, the retrospective nature of this study limited the ability to collect reference data from a laboratory or yellow springs instrument sample, and minimal laboratory glucose values were obtained as part of the standard care of these patients during their hospitalizations.
Adult hospital studies assessed CGM use under a variety of conditions and settings, including on the medical floor, ICU, during hemodialysis, and with patients with COVID, and found MARD values between 10% and 15%. 7 –9,16 Pediatric data have been limited and the majority published to date have been in children without type 1 diabetes and those undergoing procedures or who are critically ill.
One study in children without type 1 diabetes in the ICU after total pancreatectomy with islet autotransplantation found an overall MARD of 13.4%, 17 another study in children hospitalized for DKA found 95% of values were within the A and B zones on the Clarke Error Grid, 18 and a study in children without type 1 diabetes undergoing hematopoietic stem cell transplantation for leukemia reported an MARD of 20%. 19 All publications, including adult and pediatric cohorts regardless of their condition, reported clinically sufficient accuracy for inpatient use of CGMs, with proper protocols and safety precautions in place.
Although the data collected from this study are encouraging, additional research is needed to identify variations in CGM accuracy under different settings, including admission diagnosis (e.g., DKA, infections, and organ dysfunction), medication administration (e.g., insulin infusion, acetaminophen, and vasoactive medications), laboratory abnormalities (e.g., acute kidney injury or hemodialysis dependence, and acid–base imbalance), and reference glucose values (POC vs. laboratory). In addition, the development of safety and efficacy protocols will be vital to successful hospital CGM use.
Footnotes
Authors' Contributions
E.C.C. developed the research idea, analysis plan, collected data, and wrote and edited the article. L.P., G.P.F., and R.P.W. developed the research idea and analysis plan and reviewed and edited the article. L.A.W., L.T., A.J.K., E.J., and C.B. collected data and reviewed and edited the article. All authors approved the final version of the article.
Author Disclosure Statement
E.C.C. has been a speaker and served on an advisory board for Dexcom. L.P., L.A.W., A.J.K., L.T., and E.J. have no conflicts of interest to report. G.P.F. conducts research sponsored by Medtronic, Dexcom, Abbott, Tandem, Insulet, Lilly, and Beta Bionics; and has been a consultant, speaker, or advisory board member for Medtronic, Dexcom, Abbott, Tandem, Insulet, Lilly, and Beta Bionics. C.B. has been a speaker and consultant for Insulet and speaker for Dexcom and Embecta. R.P.W. has received research support from Dexcom, Eli Lilly & Co, and Tandem Diabetes Care; received conference travel support from Dexcom and Eli Lilly & Co.; and received speaking/consulting honorarium from Dexcom and served on advisory boards for Eli Lilly & Co. and Provention Bio.
Funding Information
This study is supported by Juvenile Diabetes Research Foundation (5-ECR-2022-1179-A-N).