
Abstract
Introduction:
Automated insulin delivery (AID) systems reduce burden and improve glycemic management for people with type 1 diabetes (PwT1D) by automatically adjusting insulin as a response to measured glucose levels. There is a lack of evidence on AID and nutrition variables such as dietary intake, eating behaviors, and disordered eating.
Objectives:
This scoping review aims to provide a summary of the literature regarding AID and nutrition variables and to identify gaps that require further investigation.
Methods:
Two researchers conducted a blinded search of Medline (OVID) and PubMed for studies, including AID use (compared to non-AID use) and nutrition variables. Studies from January 2000 to July 2023 were included, as were PwT1D of all ages.
Results:
A total of 3132 articles were screened for appropriateness. After exclusions, 7 studies were included (2017–2023): 4 qualitative, 1 crossover, 1 randomized controlled, and 1 observational. Studies included adolescents (n = 1), adults (n = 3) or both (n = 2), and all ages (n = 1). In quantitative studies, AID was associated with lower eating distress (−0.43 ± 0.12, P = 0.004) and higher quality of life (3.1, 95% confidence interval [CI]: 0.8–5.4, P = 0.01), but not grams of carbohydrates at meals (1.0; 95% CI: −0.7 to 3.0; P = 0.24) and snacks (0.004; 95% CI: −0.8 to 0.8; P = 0.99) compared to non-AID use. In qualitative studies, AID increased the frequency and portions of food intake and led to less dietary control from parents. AID users reported eating foods higher in energy density. PwT1D were less worried about achieving accurate carbohydrate counting (CC) when using AID.
Conclusions:
AID use appears to influence eating behaviors, dietary patterns, and CC, although evidence was limited. AID may reduce food management burden due to the perception that AID can correct for CC inaccuracy.
Significance:
Further research needs to determine if AID allows for simplification of CC and improves eating behaviors while maintaining glycemic stability.
Introduction
It is not surprising that disordered eating behaviors (DEB) are an ongoing issue for people with type 1 diabetes (PwT1D). In this population, it is common for weight gain to occur once insulin therapy is initiated, given that insulin is considered an anabolic hormone. 1 Strict diet planning, along with close monitoring of weight status by health care professionals throughout life may lead PwT1D to be more concerned about what they eat and their body weight and image compared to people without type 1 diabetes (T1D). 2 The prevalence of DEB, such as restricted eating, emotional eating, or uncontrolled eating is higher in PwT1D compared to those without, and it is more likely to impact women, adolescents, and young adults. 3 –6 DEB increase the risk of T1D complications such as ketoacidosis, nephropathy, neuropathy, retinopathy, and premature death. 7,8 They may also lead to dysregulation of emotions, cognition, stress, and physical health. 9,10
Despite the high prevalence and concerning consequences, there is a lack of evidence surrounding appropriate approaches to prevent and treat these behaviors in PwT1D. 11 Although the exact reason for DEB risk in PwT1D is not known, it is believed to be related to the necessary management of food, its burden, and related practices such as carbohydrate counting (CC). 12,13
CC involves identifying, measuring, and planning carbohydrate intake to determine insulin requirements. 14 PwT1D may also be advised to limit certain foods that contain short-chain monosaccharides (i.e., simple sugars in pastries, candies, or soda) to avoid a rapid rise in postprandial glucose, which can lead to hyperglycemia. 14,15 This practice places an emphasized focus on diet, including food rules, extensive calculations, and restrictions. 12 If CC is not used, the health care provider may recommend a fixed carbohydrate amount and spacing of meals throughout the day to match fixed insulin intake, which makes eating even more rigid. Although burdensome, CC can be beneficial in better managing postprandial glycemic changes and optimize overall blood glucose stability. 16,17 One potential approach to the prevention and treatment of DEB may be to reduce the food management burden, rules, and restrictions involved in T1D nutrition counseling.
Traditionally, fixed or flexible doses of insulin are injected at meals with a syringe or a pen (i.e., multiple daily injections [MDI]). Alternatively, insulin could be administered using continuous subcutaneous insulin infusion (CSII; nonautomated insulin pumps). 18 More recently, with the commercialization of continuous glucose monitoring (CGM) systems, other technologies have emerged such as sensor-augmented pumps (SAP). 18 Nonautomated insulin pumps have reduced the burden of diabetes management compared to MDI, by calculating insulin amounts more accurately by taking in consideration active insulin. 19 Intensive insulin therapy, either through injections or CSII, requires manual input and adjustments of prandial insulin. PwT1D are required to be diligent with CC and need high CC accuracy to optimize glycemic levels. 20 PwT1D may fear eating more or less than their predetermined amount of carbohydrates to avoid hypo- or hyperglycemia episodes, exacerbating the desire to control all aspects of their dietary intake.
New insulin delivery technologies, such as automated insulin delivery (AID) systems are increasing in use due to their ability to improve glycemic levels and reduce management burden. 21 AID systems were developed to relieve some of the burden of management like providing automated insulin adjustments. 22,23 Commercially available AID systems are known as hybrid closed loop (HCL) or advanced hybrid closed loop (AHCL) systems. Both types provide automatic basal insulin, which is adjusted based on continuously measured blood glucose levels. 21 AHCL systems additionally provide an automatic correction bolus to mitigate hyperglycemia and operate throughout the day and night. 24 Examples of HCL in Canada are MiniMed 670/770 and Omnipod 5, and AHCL are MiniMed 780G and Tandem Control IQ. AHCL have been shown to reduce emotional and behavioral burden compared to MiniMed 670G. 24 Commercial brands have regulated sensor glucose targets or ranges, aimed at ensuring safety by reducing the risk of hypoglycemia.
Some PwT1D use “Do It Yourself” (DIY) or open-source systems which use an open-source algorithm to connect a CGM to an insulin pump. 25 DIY systems allow users to choose their own sensor glucose target ranges with no restrictions. In fully closed-loop AID systems, user input for mealtime boluses (such as carbohydrate counts) is not required. 21 Since there is no user-provided information regarding the timing and content of carbohydrate in meals, postprandial hyperglycemia is a concern, therefore, trials testing the efficacy of these systems are ongoing. 26 Consensus articles have been published in the last year demonstrating the safety and effectiveness of AID systems. 22,27 –29
In 2023, a systematic review and meta-analysis of 26 randomized controlled trials in 915 children and adolescents found that youth with AID had 13% (95% confidence interval [CI]: 9.55–16.28) higher glucose time in range (TIR) compared to MDI or nonautomated pumps, while another meta-analysis of 4 studies in 359 adults found 14.5% (95% CI: 10.65 to 18.40) improvement in TIR compared to usual care. 30,31 In the Behaviors, Therapies, Technologies, and Hypoglycemic Risk (BETTER) in Type 1 Diabetes registry in Canada, about 10% of PwT1D reported using AID in 2022. 32
A growing number of PwT1D make the switch from MDI and CSII to AID. There is emerging evidence that AID improves psychosocial outcomes. For example, Polonsky et al. evaluated the psychosocial outcomes for 115 adults with T1D using the OmniPod 5 AID system. 28 The participants completed the Diabetes Distress Scale (DDS; a self-administered questionnaire focusing on emotional distress directly related to diabetes) before and after AID use over a 6-month interval. 28 They found that after AID initiation, PwT1D had 0.16 ± 0.39, P ≤ 0.001 lower mean total diabetes distress score on a 6-point scale, and less eating distress, as measured by the DDS eating subscale (−0.24, ±0.66; P ≤ 0.001). 28 Figure 1 shows the potential effect of insulin delivery technologies on food management burden. 20,33 –35
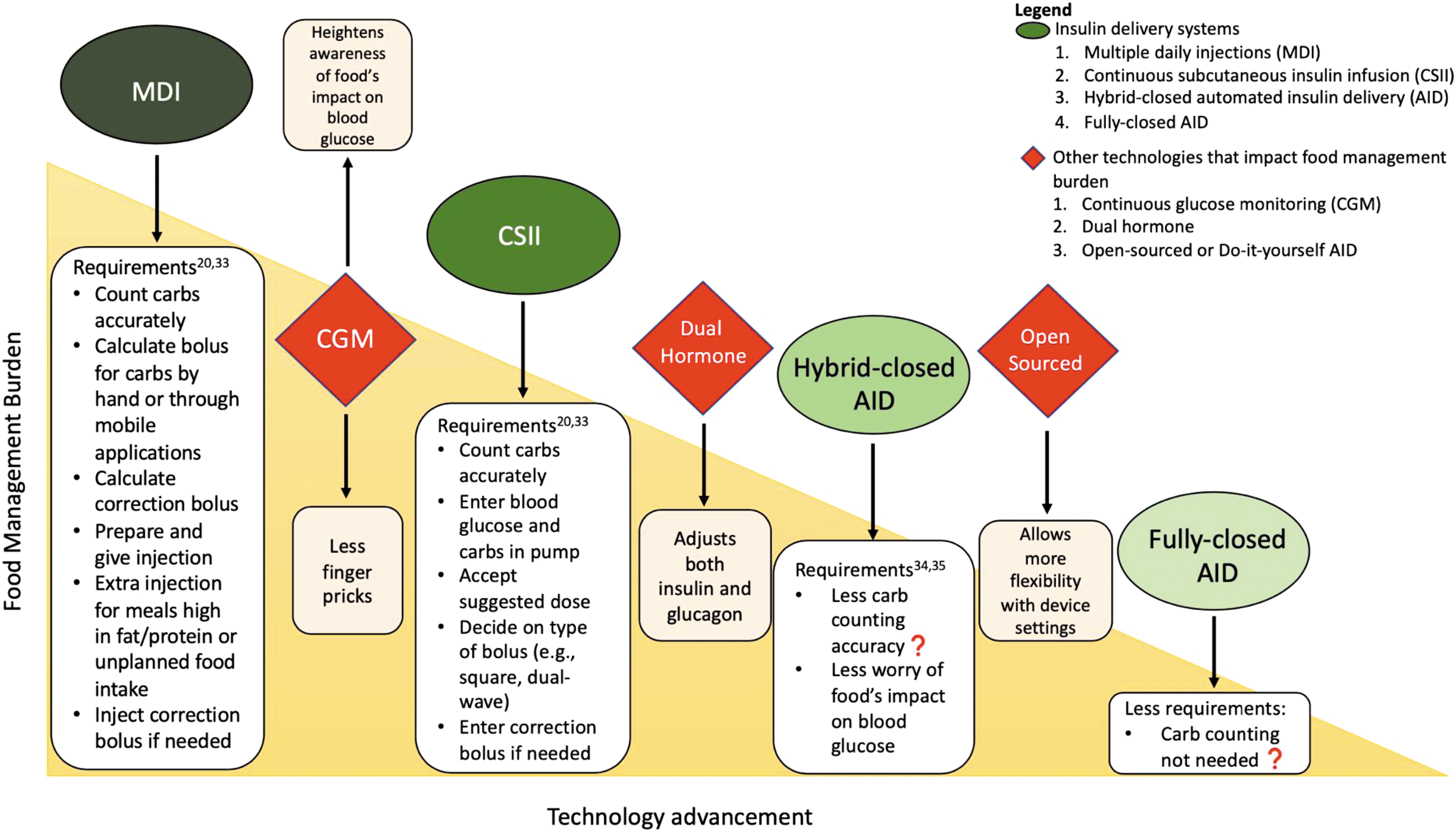
Potential effect of insulin delivery technologies on food management burden. AID, automated insulin delivery; CGM, continuous glucose monitoring; CSII, continuous subcutaneous insulin infusion; MDI, multiple daily injections;
The relationship between AID and nutrition-related outcomes such as dietary intake and eating behaviors remains a scarcely studied area. This relationship needs to be understood because AID may reduce food management burden by allowing for less CC accuracy without compromising glycemic management. This would permit more flexibility, spontaneity, and less restriction of one's intake. However, there needs to be further investigation of whether AID could be a potential treatment alternative or prevention strategy for PwT1D who engage in DEB, or if it increases the risk of binge eating behaviors.
The objective of this review was to analyze the literature regarding AID and nutrition-related outcomes in PwT1D across the lifespan to provide a summary of available evidence and identify key gaps in the literature that require further investigation.
Methods
This scoping review used two databases, Medline (OVID) and PubMed, to conduct a search of available literature. The search strategy was conducted in collaboration with a McGill University librarian. The aim of this review was to identify studies with AID as the exposure variable (compared to MDI or CSII) and nutrition-related variables like eating behaviors and dietary intake as the outcome. MeSH terms used to identify studies with the exposure AID were “Insulin Infusion Systems,” “Pancreas, Artificial,” and were combined using OR with search terms “automat* insulin” or “closed-loop*” or “hybrid-loop*” or “artificial pancreas” or “bionic pancreas.” AID terms were combined, using AND, with nutrition-related outcome terms. MeSH terms to identify nutrition-related outcomes were “Feeding and Eating Disorders,” “Feeding Behavior,” and “Eating.” These were combined using OR with search terms anorexi* or bulimi* or bing* or “disorder* eat*” or feed* or diet* or nutrit* or hung*.
The inclusion criteria were studies published from January 2000 to July 2023 which included human participants of all ages. The exclusion criteria were studies that did not exclusively investigate PwT1D, did not include AID as the exposure variable or nutrition as the outcome variable, and studies that did not include a non-AID comparison.
Two reviewers (C.S. and M.K.T.) conducted a blinded screening of all articles that were identified through search terms using Rayyan software. Articles were first screened for appropriateness based on the title and abstract. If deemed appropriate, a full review of potential articles was conducted to assess if they met the inclusion and exclusion criteria. In addition, articles such as commentaries, letter to editor, or duplicates were excluded. C.S. and M.K.T. made the final decision of articles that were included in the review.
Results
Study selection
A total of 3132 articles were screened for appropriateness after removing duplicates. Of those, 83 articles were read, and 77 articles were excluded based on the prespecified criteria (Fig. 2).
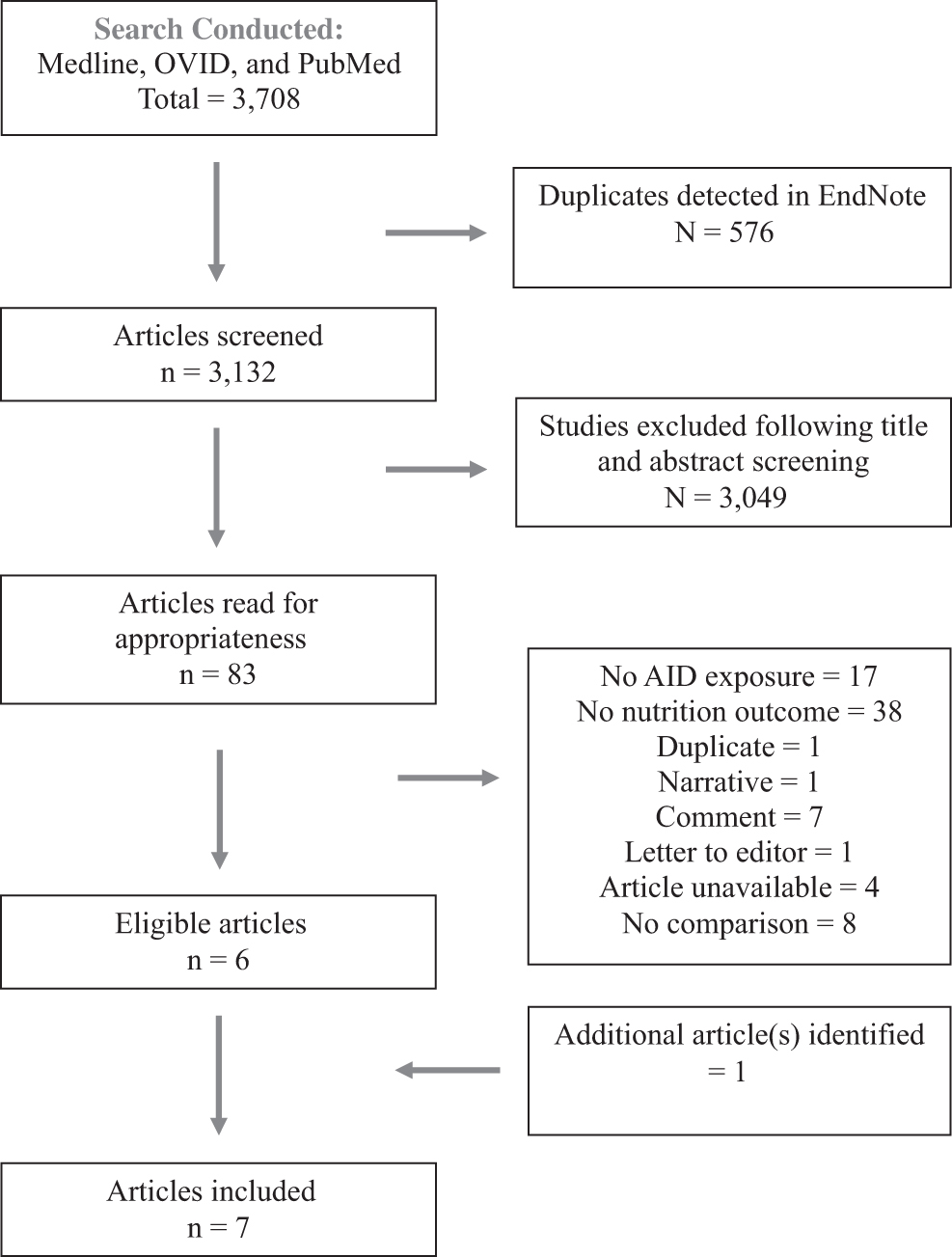
Flowchart of articles included in the review
A summary of the articles is shown in Table 1. Studies included either adolescent (n = 1), adults (n = 3), adolescents and adults (n = 2), or all ages (n = 1). The total number of participants included in this review was 303 with sample sizes ranging from 22 to 107. Of the participants, 33 were adolescents, 226 were adults, and 44 were parents or children. On average, the proportion of female participants ranged from 43% to 78%. The relationship between HCL systems and nutrition was investigated in five studies and two studies included AHCL systems.
Summary of Articles Included in the Review
AID, automated insulin delivery; CC, carbohydrate counting; CI, confidence interval; DDS, Diabetes Distress Scale; MDI, multiple daily injections; QoL, quality of life; SAP, sensor-augmented pumps.
The outcome variables included discussion around changes in dietary patterns, eating habits, or food choices for the qualitative studies (n = 4). 13,23,35,36 For quantitative measures, change in daily patterns of meals and snacks, eating constraints measured through the DDS eating subscale, or the quality of life (QoL) “eating as I would like” subscale was used. 27,37 The eating subscale measured by the DDS provides a score, with a higher value representing higher distress to responses such as “Feeling that I don't eat as carefully as I probably should,” “Feeling that thoughts about food and eating control my life,” and “Feeling that my eating is out of control.” 27 The QoL subscale demonstrates the emotional autonomy connected to eating such as feelings of joy and flexibility with food choices. 38 Through review of studies included, nutrition-related outcomes such as eating behaviors, dietary patterns, and CC were shown to be influenced after the initiation of AID.
Eating behaviors
Most studies included in this review covered nutrition outcomes related to eating behaviors following the adoption of AID. Of the studies included, two discussed eating behaviors through qualitative interviews, and two quantitative studies investigated the relationship between AID and eating behaviors, through use of the DDS and QoL eating subscale. 13,35
Among the qualitative studies, similar changes in eating behaviors were reported. 35 In both adolescents and adults, before initiation of AID, it was reported that PwT1D would control their portion sizes to avoid blood glucose fluctuations. 13,35 However, after initiation of AID, participants reported that the control algorithm would provide insulin automatically after the meal. 35 This reduced anxiety and improved confidence around eating, especially for spontaneous occasions such as eating out at restaurants. 35 For adolescents with T1D whose parents were interviewed, it was reported that family conflict around food was lower, as parents perceived the AID would provide more flexibility in eating. 13 Parents did not restrict foods such as higher carbohydrate foods, or food with added sugar, when their children were using AID. 13 Although PwT1D did not exhibit the level of unrestrained eating as Lawton et al. expected, participants were more likely to snack in between meals.
The findings from Weissberg-Benchell et al., a two-arm, randomized crossover study (11 days usual care vs. 11 days AID), complemented the findings from the qualitative work. 37 People who switched to a advanced hybrid dual hormone AID (meaning it provides both insulin and glucagon to lower risk of hypoglycemia), from their usual insulin delivery system, had a significantly lower eating distress subscale score than usual care (−0.43 ± 0.12, P = 0.004). 37 Similar findings were reported in the randomized controlled, parallel group study conducted by Cyranka et al. 38 Individuals in the treatment group (n = 20) who switched from MDI to an advanced hybrid AID for 3 months had a significantly higher QoL “eating as I would like” score (3.1, 95% CI: 0.8–5.4, P = 0.01). 38
Dietary patterns
Three studies focused on dietary pattern changes that occurred with AID use. In qualitative studies, PwT1D reported feeling more comfortable eating foods higher in fat and carbohydrate and energy density, as well as foods considered as treats. 35,36 This change in dietary pattern was explained by participants who trusted the AID system to effectively provide insulin automatically, as a response to increased glycemic levels resulting from the intake of these foods. 35,36
An observational study using a retrospective cohort (Emami et al.) did not find a statistically significant relationship between AID (compared to SAP) and the frequency of food intakes or the amount of carbohydrates in meals and snacks. 27
Carbohydrate counting
There were three studies that discussed changes in CC with AID use. In one study, PwT1D were less worried about inaccurate CC estimates and making correction boluses. 23 In qualitative studies, PwT1D expressed concerns that skills and knowledge of CC would decrease as AID requires less accuracy to achieve stable glycemic levels. 35 For example, after switching to AID, participants reported that they were less likely to weigh and analyze food labels to improve their CC accuracy. 35 Parents of youth with T1D were less concerned about their child forgetting to input carbohydrate counts, when using the AID system. 13
Discussion
In this scoping review of seven studies, four qualitative and three quantitative, we found that AID systems can influence eating behaviors, dietary patterns, and CC, although the evidence is limited. These data primarily came from qualitative studies which found that AID appeared to reduce distress around dietary situations and CC accuracy. 13,23,35,36 This seemed to encourage PwT1D to eat not only foods they may have cognitively restricted in the past, such as higher fat and carbohydrate-rich food, but also eat larger portions and snack more often. 13,35,36 It was also found in qualitative studies that both caregivers and PwT1D were less concerned about CC accuracy and believed AID would adequately compensate for any miscalculations in carbohydrate intake. 23,35
Through quantitative studies it was found that after switching to AID, PwT1D had lower eating distress, and higher flexibility in eating, 37 but there was insufficient evidence of a difference in carbohydrate intake at meals and snacks. 27 Considering this evidence, AID may provide the ability for PwT1D to adopt eating patterns more like someone without diabetes, such as less CC and concern regarding glycemic levels, and thereafter reduced food preoccupation. However, research needs to confirm that increased diet flexibility and CC inaccuracy while using AID will not compromise blood glucose levels or predispose to medical complications (i.e., neuropathy, and nephropathy, ketoacidosis), or comorbidities (i.e., hypertension, and dyslipidemia).
Several limitations were identified from this review on AID and nutrition-related outcomes. It is unknown if the observed changes in behavior can be generalized to all PwT1D, since these findings were reported in small sample sizes and lacked diversity as only one study included children. In qualitative studies, the interpretation of responses might also be limited by the subjectivity of the researcher who extracted the findings. In addition, those participating in studies designed to test the impact of AID may be subject to an intervention bias, which may modify their behavior and opinions. Strengths of this review include the diversity and breadth of search terms used to identify relevant literature, including eating behaviors, dietary intake, as well as DEB. This discovered the need for empirical evidence about AID and nutrition and studies, including DEB outcomes to improve the generalizability and clinical relevancy of findings to PwT1D.
The progression of insulin delivery technologies continues to relieve the management burden for PwT1D. Previous literature has shown a relationship between the transition from MDI to CSII and eating behaviors and thereafter glycemic levels. 39 For example, Peters et al. found in an observational study of 18 children and adolescents with T1D that 18 months after switching to CSII, energy and macronutrient intake was similar, although on average, there was a decrease of 1.2 snacks per day (P = 0.009), and 9.5% calories from snacks (P = 0.05). 39 The authors concluded that CSII allowed for more diet flexibility in snacking due to improved flexibility in insulin dosing and administration, glucose monitoring, and control. 39
Furthermore, there is evidence to suggest improvement in DEB after transition from MDI to CSII in PwT1D. 40 Markowitz et al. investigated 43 youth with T1D aged 10 to 17 years who switched from MDI to CSII, and at baseline, it was reported that females and PwT1D with overweight/obesity had higher DEB scores. 40 They found, after 1 (P = 0.01) and 6 months (P = 0.02), the Diabetes-specific Eating Problems Survey-Revised (DEPS-R) score, a validated measure of DEB risk, significantly decreased. 40 The proposed reason for the observed change was PwT1D having greater ability to adjust insulin delivery using CSII compared to MDI. 40 As more PwT1D are using AID, they may have even more diet flexibility due to the technology's ability to make automatic correction boluses and adjust basal insulin without user input, which mimics a functioning pancreas more closely.
However, a cross-sectional study (n = 271) found insufficient evidence to suggest that PwT1D who used CSII compared to MDI had lower eating distress (CSII: 2.83, standard deviation: 1.22, vs. MDI: 3.09, SD: 1.28; P = 0.77), as measured by the DDS eating subscale. 41 This suggests that the decrease in eating distress may only occur for those who switched from MDI to CSII rather than existing users of these technologies at one point in time. 41
Eating distress may be reduced by other methods separate from insulin delivery technology. For example, Fisher et al. conducted a randomized, two-arm study (n = 301) where adults with type 1 diabetes, mainly using a nonautomated pump, were assigned to either a health condition management program or emotional management program. It was found after 9 months (compared to baseline) that the mean DDS eating subscale score was lower (3.45 [SD: 1.23] vs. 2.63 [SD: 1.11]; P ≤ 0.001) for both groups. 42 However, the programs consisted of one full day workshop, and four 1-h online video meetings, over 3 months. 42 Advancement in insulin delivery technologies may offer a more timely, sustainable impact on reducing eating distress, as it addresses the underlying burden of diabetes management through reduction in required tasks for insulin administration. More studies directly comparing the impact of insulin delivery technologies and educational management programs on eating behaviors are needed.
Findings from this review complement a theoretical framework previously proposed by Kahkoska et al. 12 They hypothesized that due to the necessary food management required to manage diabetes, PwT1D may adopt a cognitive response to eating rather than following innate physiological cues, such as natural hunger cues. 12 However, with AID, less reliance on a cognitive response to eating (such as restricting portions or carbohydrate containing foods), and more flexibility to follow a physiological response (hunger cues), may lead to a more intuitive approach to eating (eating when hungry, stopping when full), or can lead to uncontrolled or binge eating. 12 It was found in the literature that AID systems' perceived benefit may lead to less worry around dietary choices and CC, however, DEB such as binge eating has not been explored.
AID may reduce the need for CC accuracy. Petrovski et al. conducted a 12-week randomized controlled trial of 34 adolescents (12 to 18 years) who switched from MDI or CSII to AID with simplified meal announcements (MiniMed 780G). 43 They found that those who used CC (compared to simple meal announcements: regular 40–70 g, large 60–90 g, and snack 15–20 g) had higher glucose TIR (P = 0.04), yet, had similar hemoglobin A1c (P = 0.17), and had glucose time below range (P = 0.28). 43 If AID lowers the need for CC accuracy, PwT1D may be able to focus less on the exact quantity and timing of carbohydrates and focus more on intuitive and balanced eating.
As technologies advance to fully closed loop where CC is not required, the impact on PwT1D's relationship with food may be even greater but further research is needed to confirm this. An intuitive eater has been described as someone who eats according to their internal hunger and fullness cues, while considering their preferences, rather than as a response to external pressures, such as media and food rules. 44 This practice may help reduce the cognitive restraint to eat certain foods, prevent DEB and eating disorders, improve glycemic levels, and overall minimize diabetes-related morbidity and mortality. 44 Still, there is a need to know if this is helpful such as reducing food restriction, or harmful as it may lead to an increase in behaviors such as uncontrolled or emotional eating. 12
Interestingly, it has been made clear from this review that there is a lack of evidence regarding the relationship between AID and DEB such as restrained or unrestrained eating and emotional eating. This is an important future research direction due to the known risk that DEB has on the medical management, and diabetes-related complications for PwT1D, as well as the consequences to cognitive, mental, and physical health. 3 There is also a need to investigate the potential impact that CC inaccuracy has on glycemic levels, identify an acceptable error margin and compare this relationship from PwT1D who use AID versus CSII and MDI. In addition, it should be explored if changes in eating behaviors and dietary patterns for AID users lead to potential health risks, such as higher cardiovascular risk or microvascular complications.
People with chronic conditions such as T1D should be counseled on food and nutrition through the perspective of DEB informed care. This means that health care professionals ought to acknowledge the disproportionate risk that PwT1D have for DEB. Moving away from strict food identification, measurement, and planning may help move toward this philosophy. Technologies are perceived by those living with T1D to warrant more flexibility in food choices and behaviors.
Conclusion
There is limited evidence that AID influences change in nutrition-related outcomes in PwT1D. This is due to the limited number of studies that have been published in this area. To further advance nutrition recommendations for PwT1D, research needs to be done to identify if AID allows for more flexibility in diet education. This will ultimately help reduce the risk of DEB for PwT1D, improve health, and prevent medical complications.
Footnotes
Acknowledgments
The authors thank Emily Jaeger-McEnroe, librarian with McGill University, MacDonald Campus, School of Human Nutrition for her advice on the search strategy for this review.
Author Disclosure Statement
M.K.T., A.M.F., D.N., and T.M.P. have no conflicts of interest to disclose. C.S. reports a research scholarship from Diabète Québec. T.M.P., A.S.B., and S.I. are Fonds de recherche du Québec en Santé Research Scholars. A.S.B. reports research grants from Canadian Institutes of Health Research, Juvenile Diabetes Research Foundation, Diabète Québec. She has received speaker fees from Dexcom, and E Lilly. S.I. reports research grants from Takeda and Diabetes Canada and has been a consultant or member on advisory panels for Takeda, Nova Nordisk, and Bausch Health.
Funding Information
No funding was received for this article.