
Abstract
Patient-generated device data play an important role in diabetes management. However, acquiring these data remains a challenge. This project aimed to understand whether implementing dedicated “Technology Navigator” (TN) personnel at a large academic diabetes clinic could facilitate access to device data without increasing work for clinic staff. A sample of visits pre- and post-TN implementation (n = 173) showed a 22% (41% vs. 19%) increase in patients who successfully shared their data from home before their visit and a 52% (67% vs. 15%) increase in visits where data were available to the provider for review before the appointment, whereas billing claims for continuous glucose monitor interpretation increased by 86% during the same period. Time analysis suggests that home uploads could save up to 747 h in medical assistant labor annually. Incorporating a TN may improve data availability, decrease time spent on nonbillable activities, and support data interpretation and billing.
Introduction
The current generation of diabetes technologies are collecting more precise and detailed data than in previous eras. In the clinic, these data can be a powerful tool to support both diabetes education and clinical decision making. Yet, accessing patient-generated device data remains a significant challenge for clinic personnel already short on time and overburdened by administrative and documentation tasks. 1,2 In response to this challenge, there is an emerging body of literature focused on best practices for diabetes data management. 3 –8 Within this literature, several reports have anecdotally suggested that implementing a centralized position responsible for technology support and data management can improve the efficiency of clinical workflows. 3,7
To our knowledge, however, there have been no systematic descriptions or evaluation of a position of this kind. This report thus contributes findings from a quality improvement project undertaken between 2021 and 2022 at the University of Washington Diabetes Institute (UWMDI), a large academic diabetes clinic that conducts >14,000 visits per year. This project aimed to understand whether implementing dedicated “Technology Navigator” (TN) personnel might facilitate access to device data without increasing work for staff.
Methods
In 2021, UWMDI implemented a TN (half time position) to support patients with technology and data uploads with the goal of increasing data availability and optimizing clinic efficiency. Before the TN, medical assistants (MAs) were primarily responsible for acquiring data for their respective providers, on top of their other responsibilities. The TN position both centralized the responsibilities related to device data and expanded outreach to patients for technology support (see Fig. 1).
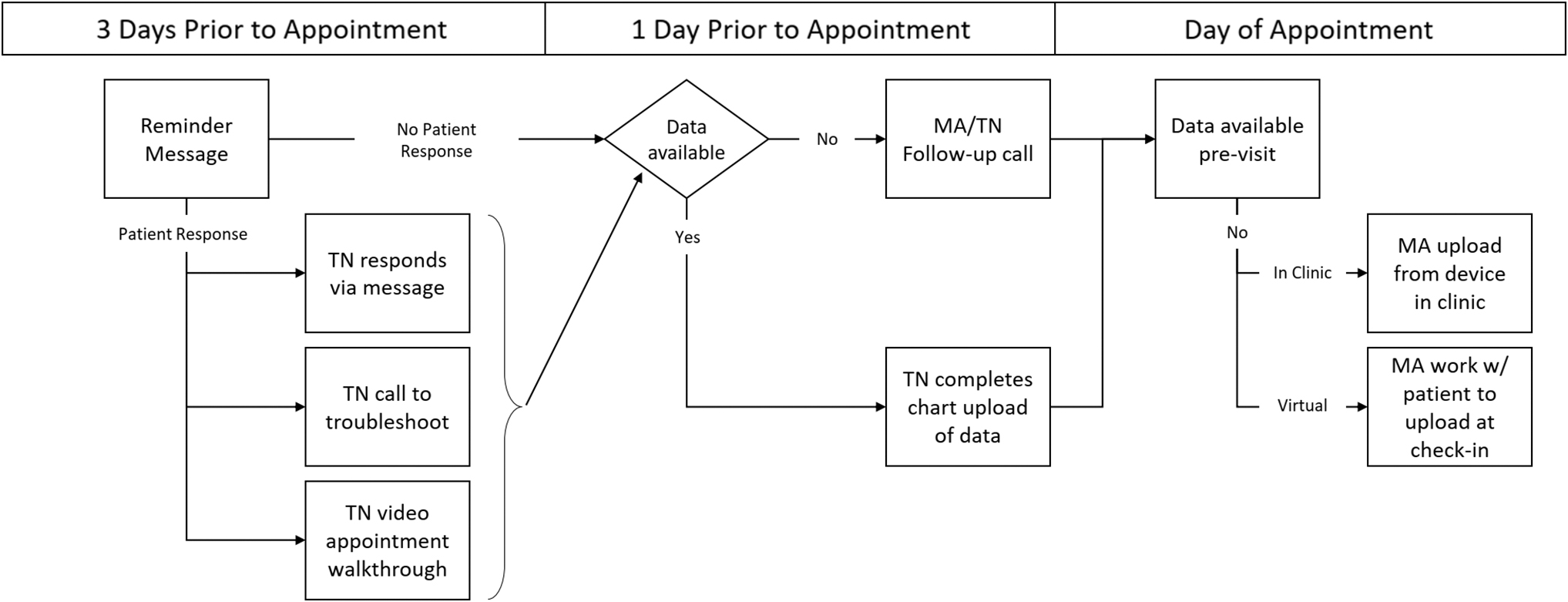
UWMDI data acquisition workflow with TN. TN, “Technology Navigator”; UWMDI, University of Washington Diabetes Institute.
Other responsibilities of the TN included reminding patients to upload data before their visit, connecting patients to the clinic to facilitate ongoing data access, and providing one-on-one assistance to patients who required help uploading their device data from home. The TN was implemented as a half-time position due to funding limitations. To bridge the gap in their availability, the TN designed a workflow (Fig. 1) that incorporated tools (such as message-scheduling software) to extend the impact of the role. The MA team covered occasional time-sensitive tasks that emerged during their nonworking hours.
To evaluate the impact of this position, this project employed mixed methods including an analysis of data availability and MA time extrapolated from a sample of 173 in-person visits in 2021 and 2022. In addition, we conducted a financial analysis of TN and MA labor costs, as well as current procedural terminology (CPT) codes related to continuous glucose monitor (CGM) interpretation aided by the TN's work. Designed as a quality improvement project specific to UWMDI, this project did not require IRB review.
We collected diabetes device data availability and time data over a 2-week period in 2021. MAs documented the time required to download device data, pull reports, and upload reports into the electronic health record for in-person visits, as well as any miscellaneous time spent troubleshooting issues related to data uploads at the time of the visit. For each visit, MAs also documented whether the patient was connected to the clinic, uploaded data at home, and whether data were available to the provider before the visit. We aimed to sample 100 visits in both 2021 and 2022. From 100 sampled visits, 70 visits had completed data forms and were included in the analysis for 2021.
This data collection process was repeated in 2022 (after the implementation of the TN), during which 103 visits were sampled and successfully completed. In 2022, data collection was expanded to also document device type and software used to pull reports. From 103 unique visits, downloads for 106 CGMs, pumps, and meters were reported. Data collection activities were supported by two authors (J.D.B. in 2021 and P.E. in 2022) who were present during the collection to assist with timing and data entry. Total time savings were extrapolated from this sample.
The authors assessed the financial impact of the TN in two ways. First, we compared the TN salary with dollars saved in MA time to understand the effect on labor costs. Second, we analyzed CPT codes for CGM interpretation recorded by UWMDI between fiscal year (FY) 2020 (pre-TN) and FY 2022 (post-TN) including codes 95250 (professional CGM) and 95251 (CGM interpretation), which require 72 h of continuous data. 3,9 Interpretation and billing were made possible, in part, by the TN's work to improve data availability.
Results
Data availability
One year after the implementation of the TN in 2021, the availability of device data improved. Comparing visits sampled in 2022 (n = 103) and 2021 (n = 70), we observed a 25% (61% vs. 36%) increase in patients connected to the clinic (i.e., linking their glucose or pump data through the manufacturer's software), 22% (41% vs. 19%) increase in patients who successfully uploaded and shared their data from home before their visit, and 52% (67% vs. 15%) increase in visits where data were available to the provider for review before the appointment.
Time savings
One of the key responsibilities of the TN is to support home uploads by patients so that patient-generated device data are available to the MA and provider before the visit. Notably, the percentage of visits that exceeded 5 min in MA time dedicated to data work was reduced by 20% (17% vs. 37%). Our time analysis suggests that home uploads can save up to 747 h in MA time annually, averaging 3.2 min in time saved per visit (n = 14,000 visits). Comparing time analyses in 2022 across device type (meter, CGM, and pump), time savings from home uploads were most notable for pump therapy (see Table 1).
Time Savings Per Device Category with Home Upload Versus No Home Upload (2022, N = 106)
CGM, continuous glucose monitor.
Financial analysis
Overall, the financial impact of the TN was positive. Though the financial analysis in labor costs remained neutral (i.e., the TN's half-time salary was equivalent to dollars saved in MA time), CGM interpretation reports at UWMDI increased from 2160 (FY 2020) to 4013 (FY 2022) after the implementation of the TN. Billing claims for CGM interpretation increased by 86% during the same period.
Discussion
This quality improvement project examined the role of the TN in the UWMDI clinic workflow. We found that the TN increased billable time and decreased the time spent on nonbillable activities (such as in-clinic uploads) that distract from direct patient care, while improving data availability and providing additional technology support to patients.
After the implementation of a TN, patient-generated device data were available in advance of visits 67% of the time compared with 15% of the time in the pre-TN workflow. From a clinician's perspective, improving device data access before visits has the potential to reduce therapeutic inertia by making data-informed treatment decisions feasible at the time of visit. Improving data availability also helps to support billing for CGM interpretation.
After the implementation of the TN, billing claims for CGM interpretation at UWMDI increased by 86%. The TN was certainly not the only factor that contributed to this increase. For example, July 2021 changes to Medicare coverage requirements for CGM undoubtedly also played a role. 10 Within the clinic workflow, the TN made a meaningful contribution by improving the availability of data required for provider interpretation and billing.
In addition to improving data availability, the implementation of a TN also improved the efficiency of data collection. After the TN, the percentage of visits that required minimal MA time (<5 min) increased to 83% from 63% pre-TN. Parsing the TN's responsibilities, this quality improvement project suggests that focusing TN efforts on supporting pre-visit home uploads is the most impactful intervention from a time savings perspective.
This project's findings support other commentaries on diabetes data management regarding the place of centralized personnel focused on technology and data within the diabetes specialty clinic. 3,7 Our report also provides an interesting point of comparison with other projects that have investigated software (vs. personnel) solutions to the data access problem. In their study of a clinic lobby device download kiosk using a standardized glucose reporting system, Mullen et al. reported 3 min in time savings per patient. 8 These time savings are consistent with our own findings, which showed an average of 3.2 min saved per visit. After the implementation of the TN, the percentage of visits that exceeded 5 min (up to 20 min) in MA time was notably reduced by 20%.
Whereas the lobby-based intervention studied by Mullen et al. facilitated in-person data uploads, the TN personnel focused on reminding and supporting patients with pre-visit home uploads to support pre-charting and facilitate data acquisition regardless of visit modality (in-person or telemedicine). In the current environment, where telemedicine is an increasingly common mode of diabetes care (and where visits may switch from face-to-face to telemedicine on the day of), supporting home uploads facilitates seamless care across modalities. 11,12
Other software solutions to the data access problem include the implementation of projects integrating CGM data directly into the electronic health record from the manufacturer's cloud, efforts that the authors support and applaud. 6,13 However, not every patient has access to or wishes to use consumer devices (such as compatible smartphones) that allow for continuous uploading to the cloud. For a variety of social and economic reasons, patients often need support uploading and transmitting their data to the clinic.
At UWMDI, 71% of the TN's individualized technology support visits were with patients aged 60 years or older, many of whom (anecdotally) did not have a consistent social support system or tech-confident caregiver to help them with their devices. By providing individualized technology assistance, the TN may help bridge the digital divide and mitigate some of the inequities that pattern the implementation of diabetes technology.
In this report, we have described how a large academic diabetes clinic integrated a TN into the clinical workflow. A comparison of time savings by device type suggests that implementing a TN (as conceived at UWMDI) may be most beneficial in clinics where patients are using a variety of diabetes technologies including pump therapy and automated insulin delivery systems (see Table 1). However, given the rapid expansion of diabetes technology (especially CGM) beyond diabetes specialty clinics, we suspect there may soon be a need for TN in some manner in a variety of clinical settings, though the specifics of the role may need to be reimagined for each context. 14 –17
For example, an alternative approach to this role might be to design the TN as a temporary transitional position to help clinic staff create the structure and workflow needed to support data acquisition and management processes. Future projects might consider the design and implementation of a TN in clinical settings such as primary care. Regardless of the setting, an ideal candidate for this nonclinical role should be adept at learning new technology and comfortable troubleshooting devices. Strong communication skills, familiarity with health care, and a commitment to helping patients would be essential.
Designed as a quality improvement initiative specific to UWMDI, limitations of this project include its small sample size and the potential for observer bias in data collection. Another limitation of this project is that data availability and time savings data were only documented for in-person visits, though we expect the impacts of both modalities—which adopted the same data acquisition workflow supported by the TN—to be similar. Future studies should also investigate the impact of TN personnel on telemedicine visits. An additional limitation of this feasibility evaluation is the dearth of staff and patient perspectives. Though we informally gathered clinician and patient perspectives on the TN role, this project did not systematically investigate their lived experiences with or perspectives on the TN.
Research on the growing role of patient-generated health data in clinical care suggests that, although often unrecognized, the labor involved in acquiring, managing, and making data meaningful—or “data work”—can be burdensome for both clinicians and patients. 18 Future studies should be designed to systematically incorporate the perspectives of both staff and patients, which can provide crucial insights into the effects of data sharing processes and efforts to improve them, such as the TN.
Conclusion
By shedding light on the often-invisible labor of device and data management in a diabetes clinic, this report illustrates that in today's time-constrained outpatient settings, reducing small but frequent disruptions can make a significant difference in clinical workflow and, by extension, patient care. In the coming years, we expect devices that improve interoperability and reduce the clinical labor required to access patient data to have a competitive advantage. At the same time, we also anticipate an ongoing need for personnel providing individualized technology assistance to patients so that everyone, regardless of technological skill or socioeconomic resources, can benefit from the expanding role of digital devices and data in diabetes management.
As digital technology grows increasingly integrated into medical care, clinics and payers will need to account not only for the material costs of these devices, but also for the various types of clinical and administrative work that is required to make the optimal use of these technologies possible.
Acknowledgments
The Technology Navigator position was made possible by philanthropic contributions to the UWMDI and Helmsley Trust grant # 2104-04483. We are thankful for this support. Our special thanks also to Cricket McCleary and the medical assistants of UWMDI for their participation in this project.
Footnotes
Authors' Contributions
P.E. contributed to investigation, data curation, and writing—original draft; S.L.K. was involved in conceptualization, visualization, and writing—review and editing; J.D.B. carried out investigation, data curation, visualization, and writing—review and editing; D.K. was involved in writing—review and editing; I.B.H took charge of supervision and writing—review and editing; S.T. was in charge of conceptualization, methodology, project administration, supervision, and writing—review and editing.
Author Disclosure Statement
I.B.H. receives research funding from Dexcom and consulting fees from Abbott, embecta, and Hagar. S.T. receives research funding from Insulet and the Bionic Pancreas Research Group. P.E., S.L.K., J.D.B., and D.K. have no disclosures to report.
Funding Information
P.E. was supported by the National Science Foundation Graduate Research Fellowship Program under Grant No. DGE 2040434.