
Abstract
Intensive therapy with exogenous insulin is the treatment of choice for individuals living with type 1 diabetes (T1D) and some with type 2 diabetes, alongside regular glucose monitoring. The development of systems allowing (semi-)automated insulin delivery (AID), by connecting glucose sensors with insulin pumps and algorithms, has revolutionized insulin therapy. Indeed, AID systems have demonstrated a proven impact on overall glucose control, as indicated by effects on glycated hemoglobin (HbA1c), risk of severe hypoglycemia, and quality of life measures. An alternative endpoint for glucose control that has arisen from the use of sensor-based continuous glucose monitoring is the time in range (TIR) measure, which offers an indication of overall glucose control, while adding information on the quality of control with regard to blood glucose level stability. A review of literature on the health-economic value of AID systems was conducted, with a focus placed on the growing place of TIR as an endpoint in studies involving AID systems. Results showed that the majority of economic evaluations of AID systems focused on individuals with T1D and found AID systems to be cost-effective. Most studies incorporated HbA1c, rather than TIR, as a clinical endpoint to determine treatment effects on glucose control and subsequent quality-adjusted life year (QALY) gains. Likely reasons for the choice of HbA1c as the chosen endpoint is the use of this metric in most validated and established economic models, as well as the limited publicly available evidence on appropriate methodologies for TIR data incorporation within conventional economic evaluations. Future studies could include the novel TIR metric in health-economic evaluations as an additional measure of treatment effects and subsequent QALY gains, to facilitate a holistic representation of the impact of AID systems on glycemic control. This would provide decision makers with robust evidence to inform future recommendations for health care interventions.
Introduction
For insulin-dependent patients living with diabetes, frequent insulin administration and glucose monitoring can be burdensome. For these individuals, the use of automated insulin delivery (AID) systems—comprising a continuous glucose monitoring (CGM) system, a controlling algorithm, and an insulin pump—has become increasingly widespread and represents an optimal intervention to achieve glycemic control. 1 –3
The rapid rate of development of AID systems has yielded devices that substantially reduce the burden on individuals with diabetes dependent on exogenous insulin. 3 However, health care budget constraints necessitate rigorous economic evaluation of AID systems to establish which represent the optimal use of health care expenditure. 4,5 Economic evaluations of diabetes health technologies have traditionally relied on glycated hemoglobin (HbA1c), a long-term and indirect biomarker and proxy for the degree of glucose control over the preceding 3-month period. 6 –12 The value of HbA1c as a biomarker for glycemic control has been established in many studies, including the landmark Diabetes Control and Complications Trial (DCCT) and United Kingdom Prospective Diabetes Study (UKPDS) studies, linking HbA1c directly to risk of complications in later life. 9,11,12
However, HbA1c (unlike other glycemic control metrics) cannot reflect periods of hyperglycemia and hypoglycemia over short time periods (e.g., detecting daily blood glucose fluctuations) 7,13,14 and can be influenced by other medical conditions. 15 One alternative metric is time-in-range (TIR), which represents the proportion of time that glucose levels fall within a predetermined range, specified by current international consensus as 3.9–10.0 mmol/l for individuals with type 1 diabetes (T1D) and type 2 diabetes (T2D), which should be achieved for at least 70% of the time per day (16 h and 48 min). 16 –18
The aims of this narrative review were twofold: (1) to identify and summarize the existing evidence on the cost-effectiveness of AID systems and the glycemic control markers used to determine health outcomes and effects, and (2) to provide a discussion on the emerging role of TIR as the clinical endpoint of choice for measuring health outcomes in future AID system-focused economic evaluations in diabetes.
Materials and Methods
Search strategy
A pragmatic literature search was conducted using the PubMed/MEDLINE and Embase databases on August 28, 2023. The search strategy was formulated using phrases such as “Automated insulin delivery,” “Cost-effectiveness,” and “Diabetes,” alongside commercial names of known AID systems. A full summary of the search terms is presented in Table 1. Studies were limited to those published in English, and a date limit of 10 years was applied. Additional hand searches were used to supplement the findings of the literature search. Finally, given this study was a literature review and did not involve direct participation of human or animal subjects, ethical approval was not applicable, and a waiver was not sought.
Search Strings Used for Online Databases
AHCL, advanced hybrid closed-loop; ICER, incremental cost-effectiveness ratio; QALY, quality-adjusted life year.
Study screening
An initial screening of study title and abstracts was conducted using prespecified screening criteria. Studies that did not report the results of a cost-effectiveness (or cost-utility) analysis, did not focus on AID systems in either T1D or T2D, or took the form of reviews, narratives, protocols, or reports were excluded. In cases where the reviewer was unable to determine whether a study should be included or excluded, a second independent reviewer was consulted. For this study, all variations and generations of AID systems were included for review. Given the complexity surrounding the various nomenclature and definitions associated with AID systems, screening was informed by appropriate AID systems terminology sourced from Sherr et al. 1
Studies that reported use of seemingly simpler technologies such as sensor-augmented insulin pumps (SAPs) but did not explicitly state whether this was used alone or in conjecture with an algorithm, were therefore not excluded. After screening of studies by title and abstract, a full-text review was conducted for the studies still included. A summary of the study screening process is presented in Figure 1.
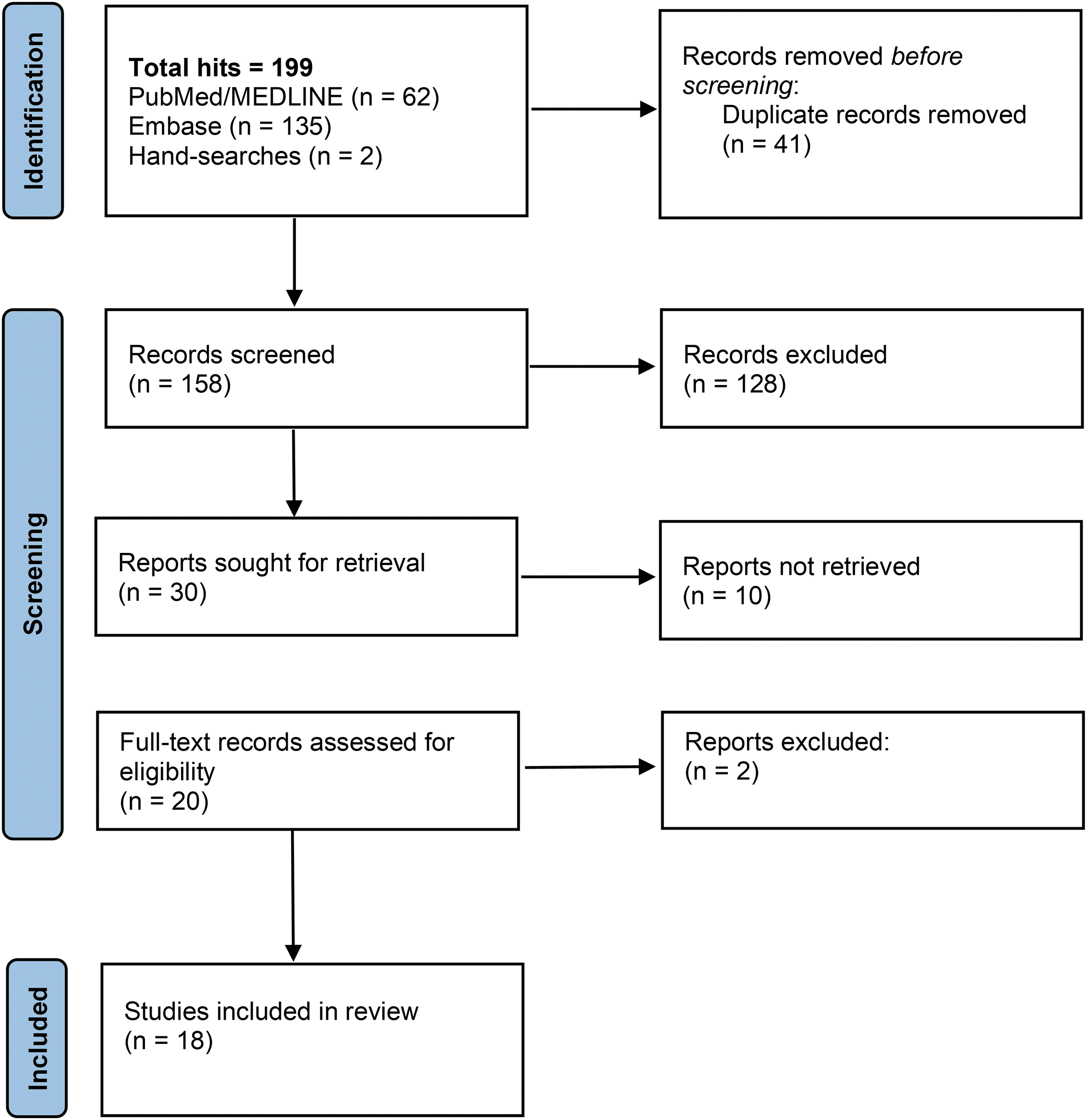
PRISMA diagram of study selection process. PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses.
Data extraction
The following data for the final 18 articles included for analysis were extracted: author name(s), year of publication, journal, setting, study design, intervention, comparator, patient population, the perspective adopted, willingness-to-pay (WTP) threshold, incremental quality-adjusted life years (QALYs) gained, incremental cost-effectiveness ratio (ICER), and the primary clinical endpoint(s) captured in the analysis.
Literature review results
A total of 199 studies were retrieved from the literature searches, and 41 duplicates were removed. Of the remaining 158 studies, 128 were excluded at the title and abstract screening stage. The most common reasons for exclusion were study types being those other than cost-effectiveness studies, and cost-effectiveness studies evaluating interventions that were not AID systems. A further 10 studies were found to only be available as conference abstracts and were therefore excluded. One further study was excluded as the full text was unavailable in English, with an additional study excluded as it did not focus solely on a specific AID system as part of the cost-effectiveness analyses. The remaining 18 studies were included after full-text review and were eligible for data extraction.
Setting and study populations
The 18 studies were conducted in various settings, with the most common settings, including Sweden (n = 4), 19 –22 Australia (n = 3), 23 –25 the Netherlands (n = 2), 26,27 and the United Kingdom (n = 2). 28,29 One study was conducted in each of the following countries: Denmark, 30 France, 31 Greece, 32 Italy, 33 Spain, 34 Turkey, 35 and the United States. 36 In all 18 studies, the population of interest was individuals with T1D (see Table 2 for full breakdown). The retrieval of studies exclusively focusing on T1D was likely a result of the insulin dependence of all individuals with T1D and the comparatively earlier onset versus T2D. 37 –40 These factors contribute to a greater unmet need in individuals with T1D and therefore likely also to greater potential QALY gains versus multiple daily injections of insulin in combination with self-monitoring of blood glucose (SMBG).
Summary of Characteristics for Included Studies
AID, automated insulin delivery; AIS, automated insulin suspension; CGM, continuous glucose monitoring; CSII, continuous subcutaneous insulin infusion; HbA1c, glycated hemoglobin; HCL, hybrid closed-loop; is-CGM, intermittently scanned continuous glucose monitoring; LGS, low-glucose suspend; MDI, multiple daily injections; PLGM, predictive low-glucose management; SAP, sensor-augmented insulin pump; SMBG, self-monitoring of blood glucose; SoC, standard of care; T1D, type 1 diabetes; UK, United Kingdom; US, United States.
Interventions and comparators
The most evaluated intervention across the 18 studies was the SAP, which was the intervention of interest in 10 of the 18 studies. The MiniMed™ 670G hybrid closed-loop (HCL) system was the second most common intervention, evaluated in three studies 21,27,28 with an unspecified HCL system used in a further two studies. 23,24 The advanced hybrid closed-loop (AHCL) MiniMed™ 780G system was the intervention in two studies 20,32 and the Omnipod 5 AID System was the intervention of interest in one study. 36 Continuous subcutaneous insulin infusion was the most common choice of comparator, featuring in 13 studies. Other comparators used included standard of care (SoC), 24,36 current care, 23 and intermittently scanned CGM with MDI. 20,27 Only one study used an alternative AID system (SAP with predictive low-glucose management) as the comparator. 32 A full summary of the interventions and comparators used across the 18 final studies is presented in Table 2.
Perspectives
The societal perspective was most commonly adopted, featuring in 12 studies, with a health care system perspective adopted in seven of the 18 studies. 23 –25,28,29,31,34 A third-party payer perspective was adopted in two studies. 35,36 Three studies conducted analyses using more than one perspective 29,34,35 (Table 2).
Cost-effectiveness of AID systems
In all 18 studies, the AID system was associated with an incremental gain in QALYs, with figures ranging from +0.03682 QALYs to +3.724 QALYs (Table 3). In six studies, the T1D cohort was further divided into two subgroups with QALY gains and ICERs determined for each subgroup. 22,26,30,31,33,35 These subgroups comprised those individuals at an increased risk for hypoglycemic events, and those with poor glycemic control at baseline. In all six studies presenting subgroup analyses, the subgroup at higher risk of hypoglycemic events gained more incremental QALYs, and had consistently lower ICERs relative to the subgroup with poor glycemic control. 22,26,30,31,33,35
Summary of Health Economic Results for Included Studies
AUD, Australian Dollar; DKK, Danish Krone; EUR, Euro; GBP, Great British Pound; SEK, Swedish Krona; TRY, Turkish Lira; USD, United States Dollar; WTP, willingness-to-pay threshold.
In 16 studies, results demonstrated that the AID system of choice was cost-effective, with one additional study (set in Greece) demonstrating that the AHCL MiniMed™ 780G system was dominant (cost-saving while leading to higher incremental QALY gains) compared to SAP with predictive low-glucose management (PLGM). 32 Only one study (set in Australia) did not explicitly state whether AID (SAP + low-glucose suspend (LGS)) was cost-effective 25 ; however, the final ICER of 40,803 Australian dollars (AUD) per QALY gained would suggest that the combination of SAP + LGS would be cost-effective based on two other Australian cost-effectiveness studies included in the present review, which specified a WTP threshold of AUD 50,000. 23,24 A summary of the health economic results from each of the 18 studies can be found in Table 3.
Clinical endpoints considered to inform health outcomes
A considerable number of the 18 studies incorporated rate-based incidence models of diabetic ketoacidosis (DKA), severe and nonsevere hypoglycemic events, in concert with multivariable models of diabetes complication incidence, and fear of hypoglycemia (FoH) to drive utility gains or losses associated with each intervention versus the respective comparator(s). Regarding the incorporation of measures of glycemic control, many studies relied on a change from baseline HbA1c. Only one study did not use HbA1c, instead capturing glycemia control by way of the incidence of moderate and severe hypoglycemic events. 25 One further study did not explicitly state that changes to HbA1c levels were used to inform treatment effects, however, a mean HbA1c level of 7.5% was modeled as part of the baseline characteristics of the cohort. 34 Notably, none of the identified studies used TIR as an endpoint or parameter to inform treatment effects, either in combination with HbA1c or as a standalone measurement.
Discussion
Results from the 18 studies identified in the literature review showed that AID systems were cost-effective in most cases, regardless of the comparator. While AID systems were more costly, they also resulted in substantial increases in quality-adjusted life expectancy versus standalone insulin delivery systems, blood glucose monitoring devices, or combined monitoring and insulin delivery systems only (i.e., those that lacked the control algorithm component of a modern AID system). These QALY gains were partly attributable to AID system users spending less time performing SMBG or administering insulin manually, which can carry significant time burdens that affect adherence. 45 Other evidence from the literature supports this, with AID system use relieving some daily diabetes management burdens, and improving patient sleep and reducing anxieties. 41
In most cost-effectiveness analyses of AID, HbA1c was the primary endpoint. Indeed, HbA1c has the merit of being a widely characterized risk factor for the development of complications, as demonstrated in studies such as the DCCT and UKPDS. 9,11,12 As baseline HbA1c and change from baseline HbA1c are almost universally reported in diabetes studies regardless of whether CGM is used, the use of HbA1c is commensurately prevalent as the primary measure of glycemic control in health economic evaluations. Conversely, TIR and related metrics (time above range [TAR] and time below range [TBR]) are only commonplace in studies of CGM and AID systems, but TIR is beginning to emerge as a primary endpoint in trials of novel insulins. 42,46 Relative to HbA1c, the use of TIR, TAR, and TBR offers the advantage of reflecting stability of glucose control, and particularly episodes of hyper- and hypoglycemia.
However, the question remains as to whether HbA1c and TIR are interchangeable or complementary measures of glycemic control. The DCCT-EDIC and UKPDS studies showed that daily glucose levels and patterns differed significantly in individuals with otherwise comparable HbA1c levels, 9,12 and therefore HbA1c is used as the primary metric alongside specific glycemic event rates (commonly severe and nonsevere hypoglycemia, and DKA) to capture the glucose control in the current health economic models. Nevertheless, there is a substantial body of evidence building up, indicating that short-term fluctuations in glucose levels can contribute to the development of diabetes complications, regardless of HbA1c levels. 43,47 Indeed, TIR, TAR, and TBR are complementary and, by definition, congruent measures of glycemic control.
Given this congruence, and the volume of data that feeds into their derivations, they have the potential to provide a more complete picture of glycemic control when used in conjunction with their current rough parallels of HbA1c, DKA, and hypoglycemia, respectively. Cost-effectiveness models relying solely on HbA1c as the measure of glycemic control may therefore underestimate complication incidence relative to alternative measures of glycemic control such as TIR.
Including TIR as a risk factor in health economic analyses may require a shift in the structure and conceptual framework adopted in current diabetes models typically using HbA1c alone. The reliance on HbA1c, hypoglycemic events, and DKA in health economic analyses is driven at least in part, by their prominence in the commonly-used diabetes models, and therefore in turn by the data that underpin the models.
When considering T2D specifically, most commonly-used economic models are HbA1c-centric with regard to glycemic control parameters, and do not consider TIR as a glycemic control measure either as an alternative to, or in concert with, HbA1c. Examples include the Building, Relating, Assessing, and Validating Outcomes model, 48 the UKPDS Outcomes Models (versions 1 and 2), 44,49 and the PRIME T2D Model. 50 Version 10 of the IQVIA CORE Diabetes Model includes an option to use TIR as an alternative to HbA1c as the primary measure of glycemic control, 51 but the methodology by which TIR is incorporated into the model is not currently in the public domain.
Despite the potential benefits of TIR, TAR, and TBR in modeling glycemic control, the current diabetes models using the combination of HbA1c, hypoglycemia, and DKA has thus far resulted in analyses in which the additional costs of AID systems have been balanced sufficiently by the QALY benefits to yield cost-effective outcomes. In each case, the AID system was found to be cost-effective despite their higher incremental costs, highlighting that the AID systems conferred sufficiently large QALY gains to balance the incremental costs and fall below the WTP thresholds of health care payers in 11 different countries. In these existing analyses, the QALY benefits have been driven primarily by reductions in the incidence of diabetes complications (e.g., DKA, severe hypoglycemic events, and micro- and macrovascular complications) and in some cases reduced FoH.
Improvements in user convenience arising from the use of AID systems have not been captured, however, in the currently available health economics models and analyses. As AID systems become more sophisticated, glycemic control benefits versus existing AID systems are likely to diminish, and the benefits of increased convenience and reduced fear of acute events is likely to play a greater role in differentiating between systems. Attempts to capture reduced FoH in health economic analyses of AID systems are already widespread, 52 and findings from a recent review showed that FoH can have a significant effect on the quality of life (QoL) of individuals living with diabetes, with sleep disruption, anxiety and stress, and anger being common effects. 53
Regarding increased convenience, carbohydrate counting has long been an important aspect of intensive insulin therapy, as carbohydrate consumption is routinely used to determine the dose of bolus insulin required. 54 Even modern AHCL systems require users to enter their estimated carbohydrate consumption by way of a “meal announcement,” but the effect of carbohydrate counting and other dietary control measures on QoL has not yet been quantified, despite the day-to-day inconvenience and potential contribution to fears associated with diabetes.
Future QoL studies could therefore look toward developing and validating patient-reported outcome measures to determine the holistic impacts that AID systems have on patient QoL. Another key area of interest that has been commonly overlooked would be the impact of AID systems on caregiver QoL, with a focus placed on the caregiving burden and psychological stress alleviated by the more advanced capabilities of AID systems present and future. 55,56 Such efforts to capture these more nuanced effects that AID systems exert on QoL should aid in conducting economic evaluations that accurately capture the user benefits arising from recent and future innovations in these devices.
Conclusion
AID systems are cost-effective interventions in individuals living with T1D when compared to a range of non-AID comparators across numerous health care settings. Existing cost-effectiveness studies incorporate data from clinical studies using HbA1c as a proxy for glycemic control. Further work is needed to establish how TIR could be used in conjunction with HbA1c levels in cost-effectiveness analyses to ensure that the impact of AID systems on glycemic control is comprehensively captured in future economic evaluations. Further research would also be welcome around the QoL benefits of stable TIR measurements, improved user convenience, and reduced burden on diabetes caregivers. Together, such research would provide decision makers with evidence to ensure that individuals with insulin-dependent diabetes have access to the most effective treatment options available given the budget constraints faced by health care systems globally.
Footnotes
Acknowledgments
Input on the literature review design and editorial support were provided by Richard Pollock and Jayne Smith-Palmer of Covalence Research Ltd, and funded by Medtronic International Trading Sàrl.
Authors' Contributions
C.M., P.G., O.C., R.V., S.d.P., and A.Z.O.S. conceived of the premise for the study. W.A. conducted the literature review and summarized relevant results from the available literature. W.A. prepared the first draft of the article, which was revised critically for intellectual content by all authors. All authors approved the final version to be published. All authors agree to be accountable for all aspects of the work.
Author Disclosure Statement
W.A. is a full-time employee of Covalence Research Ltd, which received consultancy fees from Medtronic International Trading Sàrl conduct the literature review and prepare the article. R.V., O.C., S.d.P., and A.Z.O.S. are current full-time employees and shareholders of Medtronic. C.M. serves or has served on the advisory panel for Novo Nordisk, Sanofi, Merck Sharp and Dohme Ltd., Eli Lilly and Company, Novartis, AstraZeneca, Boehringer Ingelheim, Roche, Medtronic, ActoBio Therapeutics, Pfizer, Imcyse, Insulet, Zealand Pharma, Avotres, Mannkind, Sandoz, and Vertex. Financial compensation for these activities has been received by KU Leuven; KU Leuven has received research support for C.M. from Medtronic, Imcyse, Novo Nordisk, Sanofi, and ActoBio Therapeutics; C.M. serves or has served on the speakers bureau for Novo Nordisk, Sanofi, Eli Lilly and Company, Boehringer Ingelheim, Astra Zeneca, and Novartis.
Financial compensation for these activities has been received by KU Leuven. C.M. is president of EASD. All external support of EASD is to be found on
Funding Information
The literature review, preparation of the article, and the article publishing fee were funded by Medtronic International Trading Sàrl.