
Abstract
Objective:
To evaluate the impact of missed or late meal boluses (MLBs) on glycemic outcomes in children and adolescents with type 1 diabetes using automated insulin delivery (AID) systems.
Research Design and Methods:
AID-treated (Tandem Control-IQ or Medtronic MiniMed 780G) children and adolescents (aged 6–21 years) from Stanford Medical Center and Steno Diabetes Center Copenhagen with ≥10 days of data were included in this two-center, binational, population-based, retrospective, 1-month cohort study. The primary outcome was the association between the number of algorithm-detected MLBs and time in target glucose range (TIR; 70–180 mg/dL).
Results:
The study included 189 children and adolescents (48% females with a mean ± standard deviation age of 13 ± 4 years). Overall, the mean number of MLBs per day in the cohort was 2.2 ± 0.9. For each additional MLB per day, TIR decreased by 9.7% points (95% confidence interval [CI] 11.3; 8.1), and compared with the quartile with fewest MLBs (Q1), the quartile with most (Q4) had 22.9% less TIR (95% CI: 27.2; 18.6). The age-, sex-, and treatment modality-adjusted probability of achieving a TIR of >70% in Q4 was 1.4% compared with 74.8% in Q1 (P < 0.001).
Conclusions:
MLBs significantly impacted glycemic outcomes in AID-treated children and adolescents. The results emphasize the importance of maintaining a focus on bolus behavior to achieve a higher TIR and support the need for further research in technological or behavioral support tools to handle MLBs.
Introduction
Optimal glycemic control in children and adolescents with type 1 diabetes is imperative to facilitate normal growth, reduce long-term complications, and counteract the increased mortality risk that has been linked to higher HbA1c during childhood. 1 –3 However, management of type 1 diabetes in youth can be challenging, and previous studies have demonstrated that missed and late meal boluses (MLBs) significantly impact glycemic outcomes. 4 –6 Current consensus guidelines recommend aiming for a HbA1c level <7% and a continuous glucose monitoring (CGM)-derived time in range (TIR; 70–180 mg/dL) of >70%, 7,8 but results from the T1D Exchange in 2022 showed that only a small percentage of youth meet the recommended targets. 9 Over the years, iterative advances in automated insulin delivery (AID) systems have provided continuous improvements in glycemic outcomes, and studies show that AID systems improve glycemic control compared with other treatment modalities. 10,11 So far, however, no real-world studies have assessed the glycemic effects of missed or mistimed meal boluses with these systems in youth—a population in which optimal bolus behavior can be particularly challenging. Thus, the objective of this study was to evaluate the impact of MLBs in AID-treated children and adolescents with type 1 diabetes.
Research Design and Methods
Study design and population
This was a two-center, binational, population-based, retrospective cohort study conducted at Stanford Pediatric Diabetes Clinic, Palo Alto, California, United States, and Steno Diabetes Center Copenhagen, Herlev, Denmark. The cohort comprised all children and adolescents (6–21 years of age, both inclusive) with type 1 diabetes at the two centers treated with either a commercially available Tandem t:slim X2 with Control-IQ (CIQ) technology (Tandem Diabetes Care, CA, USA) or Medtronic MiniMed 780G (Medtronic, CA, USA) insulin pump between January 1, 2019, and December 31, 2021. The project was approved by the Institutional Review Board at Stanford University (IRB-63984) and the Capital Region of Denmark (R-22031406).
Data sources and collection
One month of the most recently available insulin pump and CGM data were extracted from the uploading platforms t:connect (Tandem Diabetes Care, CA, USA), Diasend (Glooko, CA, USA), and CareLink (Medtronic, CA, USA) and used for data analysis. If there was <10 days of CGM data available within this 1-month period, their data were not included. Demographic and baseline characteristics (age, sex, diabetes duration, and AID use) were obtained from electronic medical records at each clinic.
Outcomes
The primary outcome was the association between the number of MLBs per day and the percentage of CGM-derived TIR. Secondary endpoints were other consensus-recommended CGM metrics, including time below range (TBR; <54 and <70 mg/dL) and time above range (TAR; >180 and 250 mg/dL), coefficient of variation (CV), mean sensor glucose, glucose management indicator (GMI), and the proportion of individuals attaining the guideline-recommended clinical targets for TIR (>70%), below 70 mg/dL (<4%), and above 180 mg/dL (<25%). 12 Additional exploratory endpoints (overall and per meal type) included 4-h postprandial TIR, TAR, TBR, and level 1 (<70 mg/dL) and level 2 (<54 mg/dL) hypoglycemia incidence. Meals were detected by an insulin bolus with carbohydrate (CHO) entry (denoted CHO bolus) or by CGM data using the following algorithm: a rise in sensor glucose >2 mg/dL/min over 20 min without a hypoglycemic episode (<70 mg/dL) within the prior 20 min. A missed meal bolus was defined as a meal without a CHO bolus within 30 min before to 90 min after the beginning of an algorithm-detected meal (timing based on initial rise of glucose). A late meal bolus was defined as a CHO bolus between 0 and 90 min after an algorithm-detected meal. Because there is about a 15-min delay in the rise of glucose after eating and a sensor lag time of 3–10 min, if the CHO bolus occurred after the CGM increase was detected, the meal bolus was considered late. The algorithm for detection of MLBs was developed by six physicians (C.L., A.G.R., J.S., L.E., B.B., and K.N.), of which four are certified pediatric/adult endocrinologists and two are engineers (T.R. and J.B.J.), over four iterations. Further information on the meal-detection algorithm is available in Figure 1.

Algorithm-based detection of missed and late meal boluses. Illustration of 24 h of continuous glucose monitoring (CGM) data (including algorithm-detected missed and late meal boluses) for a random subject in the cohort. Meals were detected by processing CGM and insulin data in MATLAB using the following criteria: a rise in sensor glucose of more than 2 mg/dL/min over 20 min without any hypoglycemic episode (<70 mg/dL) within 20 min before the beginning of the meal. A missed meal bolus (red circle) was defined as a meal without a bolus dose within 30 min before to 90 min after the beginning of the algorithm-based meal detection. A late meal bolus (black triangle) was defined as a bolus dose between 0 and 90 min after a meal. The rationale for setting the beginning of the interval to 0 min was because of the fact that (1) the meal first needs to have some absorption before there is a rise in glucose and (2) there is a small (∼3–10 min) sensor latency. Thus, the actual food consumption is estimated to have taken place ≥15 min before the algorithm-detected meal. Rescue carbohydrates (yellow cross) were identified when hypoglycemia (<70 mg/dL) had been present ≤20 min before the meal detection. These events did not count as a missed meal bolus.
Statistical analyses
Baseline characteristics are summarized using mean ± standard deviation or numbers and proportions, and all outcomes are presented as either odds ratio (OR) or estimated treatment difference (ETD) together with their 95% confidence interval (CI). Assessment of the association between MLBs and CGM-derived endpoints was performed using both a logistic regression model and pairwise comparison by dividing the population into quartiles based on the number of MLBs (Q1: fewest, Q4: most). The pairwise comparison was evaluated using a general linear model, and both crude and adjusted (sex, age, diabetes duration) P-values are provided. If the overall across-group P-value was <0.05, pairwise between-group comparisons were performed adjusting for multiple comparisons using the Bonferroni method. The 4-h postprandial glucose profiles for late and missed meal boluses were compared using repeated-measurement analysis of variance for continuous outcomes and mixed-effects logistic regression models for categorical outcomes. Non-normally distributed data with repeated measurements were analyzed using the Kruskal–Wallis test. Statistical analyses were performed in SAS 9.4 (SAS Institute, Cary, NC, USA). A two-sided P-value <0.05 was considered statistically significant.
Results
In total, 189 AID-treated children and adolescents with type 1 diabetes were included in the cohort. A study flowchart is presented in Supplementary Figure S1, and baseline characteristics are shown in Table 1. The cohort (48% females) had a mean age of 13 ± 4 years, duration of type 1 diabetes of 6 ± 4 years, and a duration of AID use of 10 ± 6 months. The proportion of individuals using Tandem Control-IQ (CIQ) and Medtronic 780G was 75% and 25%, respectively (baseline characteristics for each AID device subgroup are presented in Supplementary Table S1). Overall, the cohort of children and adolescents had a TIR of 64.3% ± 13.5, TBR<70 mg/dL of 2.0% ± 2.0, TAR>180 mg/dL of 33.7% ± 14.3, and a GMI of 7.3% ± 0.6 (Table 2). Subgroup analysis showed that females had significantly higher TIR than males (ETD: 4.0% [95% CI: 1.0; 7.1]) and that the association between age and TIR displayed the typical pattern seen for children and adolescents with slightly higher TIR in females (Supplementary Fig. S2).
Demographic and Baseline Characteristics
Data are mean ± SD or n (%).
AID, automated insulin delivery; SD, standard deviation.
CGM Metrics by Number of Missed or Late Meal Boluses
If the overall P-value was <0.05, a pairwise comparison (with Q1 as reference) was performed adjusting for multiple comparisons using the Bonferroni method.
Data are mean ± SD or n (%).
P-value (adjusted) <0.05.
P-value (adjusted) <0.01.
Adjusted for sex, age, and diabetes duration.
CGM, continuous glucose monitoring; GMI, glucose management indicator; Q1, Q2, Q3, and Q4, first, second, third, and fourth quartile for number of missed or late meal boluses per day, respectively.
The mean number of MLBs per day by quartile spanned between 1.2 ± 0.3 (Q1) and 3.5 ± 0.6 (Q4). The total number was generally comparable across age groups, but those aged 11–15 and 16–21 years had more missed meal boluses compared with those aged 6–10 years, who conversely had slightly more late meal boluses (Supplementary Fig. S3). The regression model showed that each additional MLB per day was associated with a 9.7%-point (95% CI: 11.3; 8.1) decrease in TIR (Fig. 2). The regression models for TAR>180 mg/dL and TBR<70 mg/dL also showed a statistically significant (P = 0.017 and P < 0.0001, respectively) correlation (Fig. 3). Compared with Q1 (TIR 74.6 ± 8.9%), Q4 had 22.9% (95% CI: 27.2; 18.6) less TIR (Table 2). Similarly, the group with the most MLBs (Q4) spent 24.4% (95% CI: 19.9; 28.9) more TAR>180 mg/dL, had a higher mean glucose (ETD: 46 [95% CI: 37; 54] mg/dL), higher CV (ETD: 4.2% [95% CI: 2.2; 6.2], and higher GMI (ETD: 1.0% [95% CI: 0.9; 1.3]), whereas TBR<70 mg/dL was lower (ETD: −1.1% [95% CI: 0.6; 1.4]). In the total cohort of children and adolescents, the proportion of individuals reaching targets for TIR, TBR<70 mg/dL, TAR>180 mg/dL, and combined TIR, TAR>180 mg/dL, and TBR<70 mg/dL was 37%, 87%, 30%, and 22%, respectively. The proportion of individuals obtaining the TIR, TAR>180 mg/dL, and combined TIR, TAR>180 mg/dL, and TBR<70 mg/dL targets was significantly higher for those with fewest MLBs (all P-values <0.01), whereas there was no statistically significant difference in the proportion of individuals attaining the TBR<70 mg/dL target (Fig. 4). The glycemic control in those aged 6–10, 11–15, and 16–21 years did not differ substantially (Supplementary Fig. S4). Overall, 83.3 ± 11.5% of MLBs led to hyperglycemia within 90 min, and the analysis demonstrated that both missed (P < 0.001) and late (P = 0.010) meal boluses contributed to the glycemic deterioration (Supplementary Table S2).

Association between number of missed or late meal boluses and percentage of time in range. The logistic regression model is adjusted for sex, age, and diabetes duration. Blue hatched area is the 95% confidence interval, and the dotted lines show the 95% prediction limits.
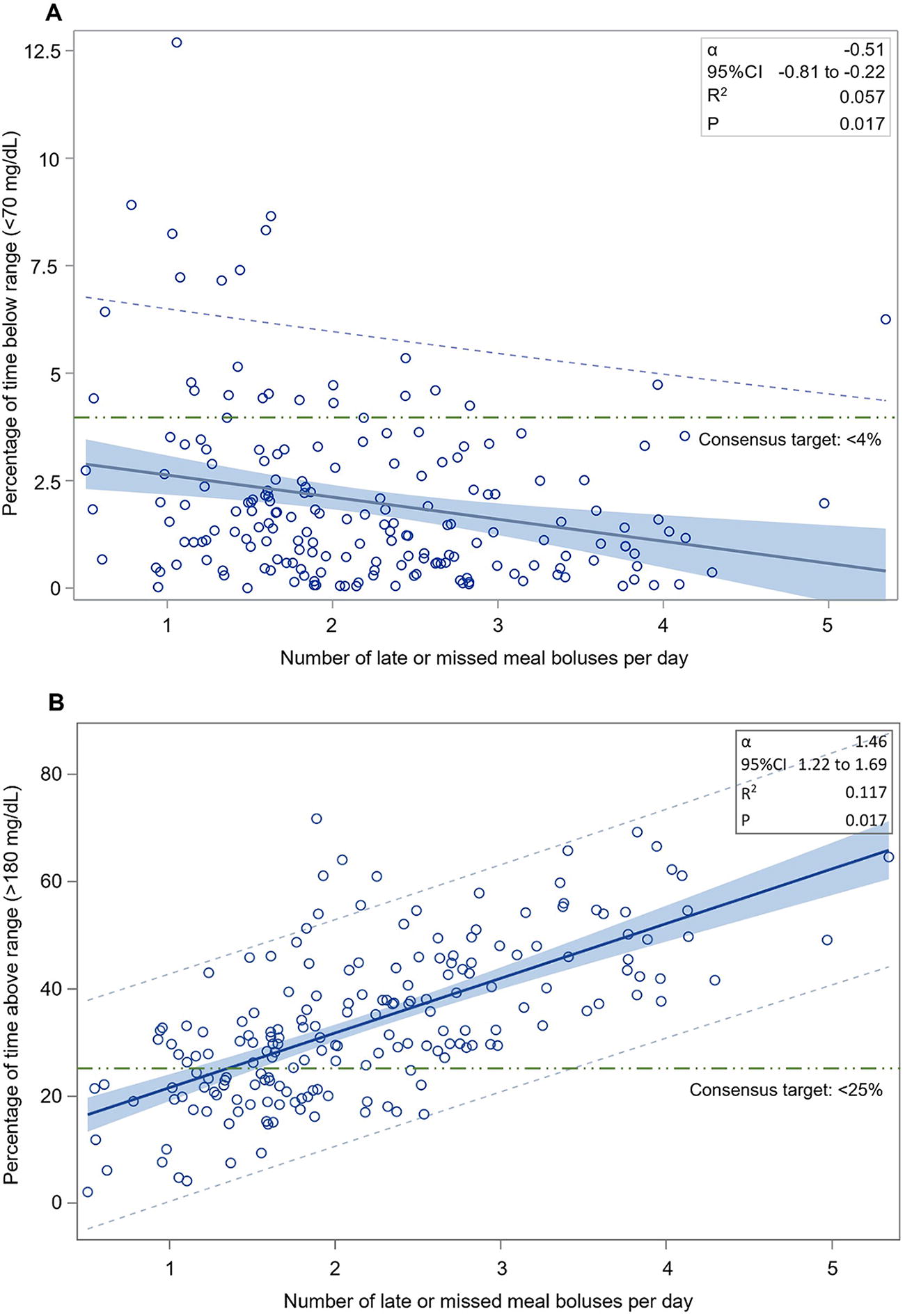
Association between number of missed or late meal boluses and percentage of time below and above range. Association between number of missed or late meal boluses per day and
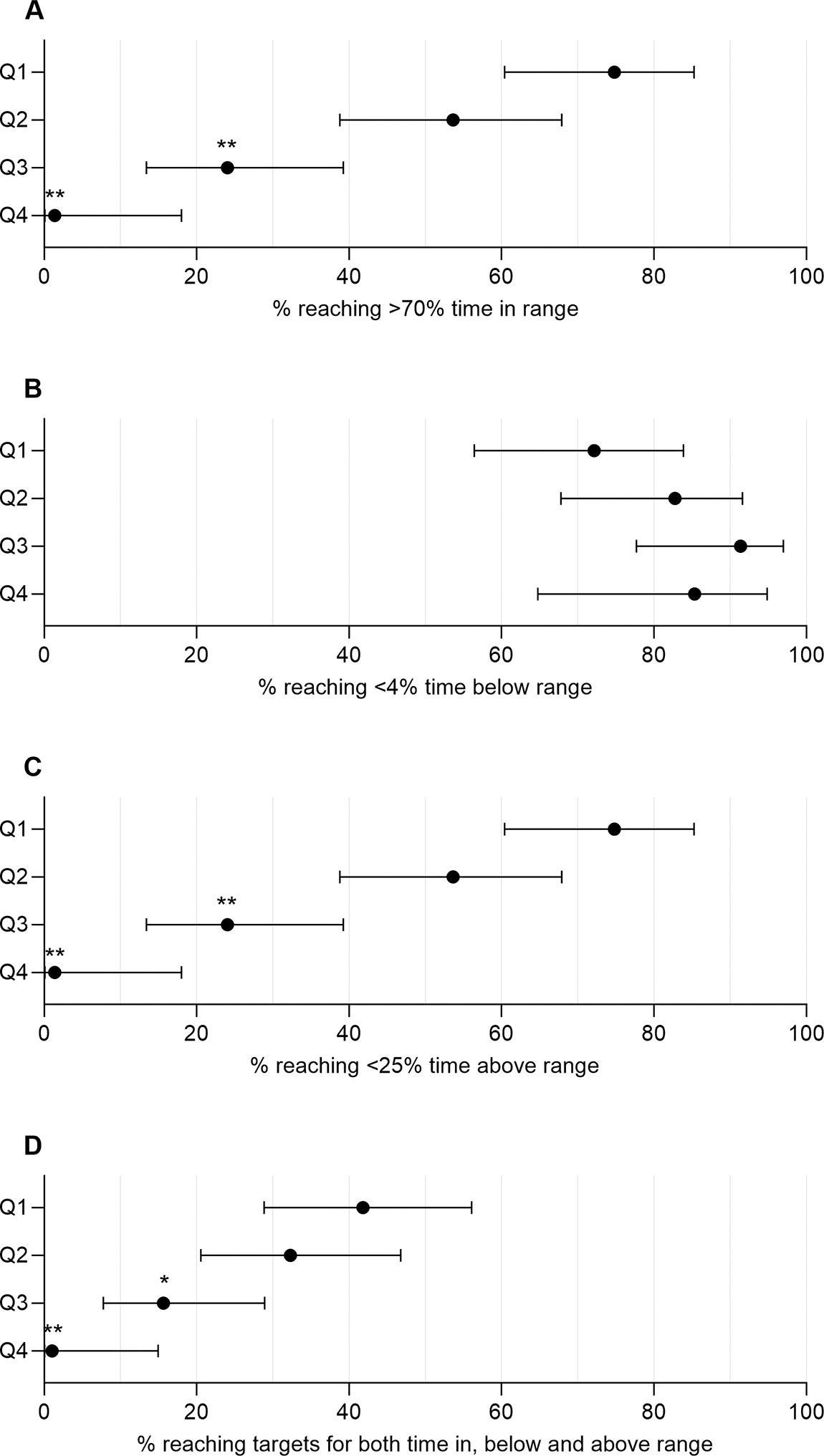
Proportion of individuals reaching recommended targets for time in range by number of missed or late meal boluses. Proportion of individuals (with 95% confidence intervals) in each quartile obtaining targets for time in
In addition to the CGM endpoints derived from the entire study duration, the 4-h postprandial CGM profile for late versus missed meal boluses was also evaluated (Table 3). This analysis demonstrated that missed meal boluses compared with late meal boluses led to statistically significantly less TIR (ETD: −4.4% [95% CI: −5.6; −3.2]) and more TAR>180 mg/dL (ETD: 4.1% [95% CI: 2.8; 5.3]). In contrast, more episodes of both level 1 and level 2 hypoglycemia were observed following late versus missed meal boluses (OR: 1.4 [95% CI: 1.2; 1.7 and 1.8 [95% CI: 1.4; 2.4], respectively). In the assessment of the 4-hour postprandial CGM profile following late and missed meal boluses for each AID device, they both displayed similar trends to those observed in the total population (Supplementary Table S3). When assessing the correlation between the lateness of a late meal bolus (i.e., how late a bolus was administered) and the 4-h TIR, a small but statistically significant (α: −0.06, P < 0.0001) association was seen (Supplementary Fig. S5).
4-H Postprandial Hypoglycemia and CGM Metrics for Late and Missed Meal Boluses
Data are mean ± SD or n (%).
CI, confidence interval; OR, odds ratio; ETD, estimated treatment difference.
Across all participants and the entire study duration, a total of 11,512 late and missed meal boluses were observed. For both late and missed boluses, more episodes were seen during lunch and dinner time than during breakfast (Table 4). At the same time, both late and missed boluses occurring in relation to lunch and dinner led to statistically significantly less TIR and more TAR in comparison with episodes experienced at breakfast.
4-H Postprandial CGM Metrics by Meal Category
Data are mean ± SD. Breakfast, lunch, and dinner are defined as 5 a.m. to 10.59 a.m., 11 a.m. to 4.59 p.m., and 5 p.m. to 0.59 a.m., respectively. A total of 698 (6.0%) events happened between 1 a.m. and 4.59 a.m. and are not included in the analysis. If the overall P-value was <0.05, pairwise comparisons between each of the meals were performed adjusting for multiple comparisons using the Tukey–Kramer method.
Significantly (P < 0.05) different from breakfast.
Significantly (P < 0.05) different from lunch.
Significantly (P < 0.05) different from dinner.
Discussion
In this two-center, binational, real-world, population-based cohort study, algorithm-detected MLBs were significantly associated with inferior glycemic outcomes in AID-treated children and adolescents with type 1 diabetes. The real-world study is the first to evaluate the effect of both MLBs in youth treated with advanced AID systems, and the results highlight the dichotomy between improving glycemic control and decreasing the burden of diabetes. Currently, more TIR is achieved by decreasing MLBs, but giving meal boluses is a burden on many children and adolescents and the consequences of MLBs are only partially mitigated by AID.
Overall, the children and adolescents in this study achieved a mean TIR of 64.3%. Previous real-world studies have evaluated the performance of Tandem CIQ and Medtronic 780G in youth 13 –15 demonstrating a mean TIR ranging between 65% and 74%. Although demographic characteristics, including age ranges, and other eligibility criteria varied between these real-world studies, the glucose outcomes demonstrated in this study are minimally lower than the previously reported studies. Both randomized clinical trials and real-world studies have demonstrated that AID provides superior glycemic outcomes compared with other treatment modalities, 16 and this real-world study confirms that, in general, these advanced systems can provide reasonable glucose control in youth.
The findings of this study are consistent with the results of previous research undertakings evaluating the effect of MLBs on both multiple daily injection therapy and non-AID insulin pumps. 17 –25 These studies, using algorithm-defined, participant-reported, or physician-based identification of MLBs, uniformly reported that a higher occurrence of these episodes was negatively associated with glycemic control. No previous studies have assessed the real-world effects of both MLBs in AID users, but studies in users transitioning from non-AID pumps to the CIQ, Medtronic 780G, and Omnipod 5 system have collectively shown that the number of user-initiated boluses decreased after starting the new AID treatment. 26 –28 In another recent study evaluating predictors of TIR in children using Tandem CIQ, it was demonstrated that the group of children with the best glycemic control also had the highest number of user-initiated boluses. 29 Although the study did not identify and evaluate the impact of MLBs, the results do support the general finding that—despite the auto-correction features—glycemic control on AID systems still improves with increasing user interaction. These data are supported by the findings in another recent post hoc analysis of a CIQ trial in children. 30 The analysis in which missed meal boluses were manually identified in 60 children aged 6–12 years demonstrated that TIR was lower on days with 1 and ≥2 missed meal boluses than days without any. The study also found that treatment with Control-IQ attenuated the glucose excursions following missed meal boluses compared with sensor-augmented pump (SAP) therapy but that suboptimal bolus behavior on CIQ treatment still did not achieve the same glucose outcomes as meal-time bolusing with SAP therapy. The study did not report the number of MLBs or the correlation to TIR or other sensor-based glycemic metrics.
Recent studies have also assessed the effect of Medtronic’s 780G meal recognition algorithm. In a small 12-day outpatient study in children and adolescents, it was demonstrated that the control algorithm was able to avoid significant increases (≥50 mg/dL) in sensor glucose levels after consumption of snacks of up to 20 g CHO. 27 The same conclusion was reached in a longer 90-day study among 780G-treated adults. 31 This study also demonstrated that, while not announcing meals ≤80 g of CHO appeared to be safe, there was still a significant difference in TIR when using the 780G system with meal announcement (TIR: 77.7%) compared with no meal announcement (TIR: 67.5%).
In our study, results showed that both missed meal boluses and late meal boluses impacted overall glycemic control. In addition, evaluation of the 4-h postprandial CGM profile showed that, as expected, TIR was markedly reduced following both a late and a missed bolus compared with the TIR observed over the full study period. The data also demonstrated that missed meal boluses compared with late meal boluses resulted in statistically significantly less TIR and more TAR. More episodes of both level 1 and level 2 hypoglycemic events were observed following late meal boluses compared with missed meal boluses; results consistent with “insulin stacking”, i.e. automated increase in insulin delivery due to the initial glucose rise with a late meal bolus plus a subseqent late mealtime bolus dose–findings resonating well observations from clinical practice. When evaluating the association between the lateness of late meal boluses and the 4-h TIR profile, it was shown that delaying bolus administration led to a statistically significantly lower TIR, although the magnitude of impact, from a clinical perspective, was rather small. The weak correlation could potentially be attributed to the fact that meals associated with steeper and larger increases in glucose levels may promote faster corrective actions, thereby blurring the underlying relationship between lateness of bolus administration and postprandial glucose levels.
Late and missed boluses were more frequently observed during lunch and dinner and led to increased deterioration in the 4-h CGM profile compared with episodes occurring at breakfast. These patterns could potentially be explained by the morning routine behavior, for example, increased parent supervision, fewer disturbances, and less day-to-day variation in meals and habit structure and an overall increased interference of daily life activities with bolus behavior during lunch and dinner time. Importantly, however, late and missed meal boluses occurred regularly for all meals and had clinically meaningful impact on glycemic control across meal types, stressing the importance of addressing bolus behavior across the whole day.
Despite the fact that AID-treated children and adolescents are also impacted by late and missed meal boluses, AID systems can, in comparison with other treatment modalities, still be an effective way to moderate the glycemic deterioration resulting from missed or late boluses. In a small retrospective study, it was demonstrated that adults with minimal or no user-initiated boluses experienced a significant improvement in HbA1c and TIR after transitioning to Tandem CIQ therapy 32 —results that confirm the findings in early in-clinic evaluations of AID’s ability to handle missed or underestimated meal boluses compared with conventional pump therapy. 33,34 Another recent study found that the introduction of a mobile bolus feature in both young and adult CIQ users with preceding low bolus frequency resulted in an increase in the number of user-initiated boluses, which, as observed in other studies, remains an important predictor of glycemic outcomes. 35 More recently, a small proof-of-concept study demonstrated that treatment with Medtronic 780G in combination with a smartphone-paired smartwatch KLUE application—detecting eating and drinking gestures and transmitting these to the pump for automatic bolusing—provided relatively similar glucose control (mean change of −2.8% in TIR from baseline) to usual manual meal bolusing. 36 Thus, looking ahead, new solutions for managing the challenges with late or missed meal boluses, as demonstrated by this study, may be nearing clinical practice.
The study has some limitations—the main ones being the general constraints related to observational study designs and the inherent lack of method for true meal detection. Currently, no gold standard exists for meal detection. Some early studies have used participant-reported or physician-based identification of MLBs, which, despite having some benefits, comes with significant biases and limitations for large-scale application. 17,18,20 Most recent studies, however, have used CGM-based approaches by applying a rule-based rate-of-change (RoC) algorithm to detect meals. Although these different meal detection algorithms may vary a bit, they all apply the same fundamental approach and many use a very similar RoC criteria. 21 –23,25,37 –39 Similar to these studies, the current study applied a rule-based RoC algorithm to detect missed meals. The strengths of CGM-enabled rule-based RoC algorithms, including ours, compared with participant-reported or physician-based identification of MLBs, include the possibility to implement these on a large scale—including in AID systems and in data analysis and visualization platforms—and the lack of recall bias inherently attributed to manually reported bolus behavior. Neither our meal detection algorithm nor any of those previously referred to are currently used in any commercial devices or analytical software, except for Medtronic’s meal detection algorithm. The Medtronic meal detection module uses a weighted average of sensor glucose RoC to identify a meal that was missed or a meal whose CHO content was underestimated. Similarly, the algorithm applied in our study was based on a RoC design although simpler than Medtronic’s proprietary algorithm. The detection rate effectiveness of the algorithm in identifying late or missed meal boluses was evaluated by six physicians, including pediatric and adult endocrinologists, and optimized over four iterations. Nevertheless, the inherent lack of true meal detection remains a limitation.
The present study is the first to report the real-world glycemic effects of both MLBs in AID-treated children and adolescents as well the glycemic impact based on meal type. The strengths of this study include the two-center, binational, population-based design and the real-world data, enabling evaluation of glycemic control and behavioral patterns in a representative, unselected population using two widely used AID systems—data that are important to acquire complementary evidence to randomized clinical studies.
Looking ahead, further research in meal detection and bolus behavior and evaluation of potential commercial applications of these concepts are needed. These topics, among other things, include assessment of the comparative handling of late and missed meal boluses between commercial AID systems and how sleep, activity, and active insulin time settings may influence the pumps’ ability to correct postprandial hyperglycemia following late and missed meal boluses. Although AID devices overall share many features, the systems do vary in different aspects, including, for example, the algorithms used for auto-correction; the Medtronic 780G system delivers auto-corrections with a frequency up to every 5 min (with a sensor glucose target of 120 mg/dL) if the SmartGuard feature determines that a correction bolus is necessary, 40 whereas Tandem CIQ delivers automatic correct boluses of 60% of the calculated dose up to once an hour (with a sensor glucose target of 110 mg/dL) when glucose levels are predicted to rise above 180 mg/dL in the next 30 min. 41 Importantly, these differences should also be viewed in the context of different basal adjustment algorithms. Therefore, evaluation of the handling of late and missed meal boluses on each system is of clinical relevance.
In the present retrospective cohort study, the AID systems were not randomly assigned to study participants resulting in measurable differences in demographic and baseline characteristics as well as a significant risk of confounding factors (e.g., sociodemographic differences). In addition, use of the different AID systems was not distributed equally between centers, and the accessibility to and selection of device are highly dependent on the geographical location (treatment center). Therefore, the current study was not designed to evaluate the comparative effectiveness in handling late and missed boluses. However, the performed device subgroup analyses did demonstrate that the 4-h postprandial CGM profiles following late and missed meal boluses were affected by both AID devices and that the trends displayed for late versus missed meal boluses in the total populations were observed for both systems. These data suggest that, as expected and as indicated from previous studies, bolus behavior is important when using both AID devices. Nevertheless, the effectiveness of different AID systems and the impact of pump settings on the occurrence of late and missed boluses should be addressed in future studies to enable implementation of these patterns into clinical decision-making. In addition, continued evaluation of new and existing wearable-integrated meal detection methods is of importance. Also, CGM-enabled algorithm-based detection strategies for late and missed meal boluses in health care provider-facing analytical software could serve as a tool to identify bolus behavior challenges and to optimize patient engagement. Lastly, future meal recognition incorporation into AID software may allow for fully closed-loop systems eliminating the need for CHO counting and meal bolusing while meeting glycemic targets; all of these are areas of research in need of further exploration.
Conclusions
In conclusion, this study demonstrated a significant impact of MLBs on glycemic control in AID-treated children and adolescents. The results emphasize the importance of maintaining a focus on bolus behavior to achieve higher TIR and support the need for further research in technological or behavioral tools to handle MLBs.
Footnotes
Authors’ Contributions
All authors were involved in the design of the study. C.L. collected the data at Steno Diabetes Center Copenhagen and Stanford Pediatric Diabetes Clinic (performed as a visiting scholar at Stanford) and wrote the first draft of the report. T.R. implemented and ran the meal-detection algorithm, and A.G.R. performed the statistical analysis. All authors contributed to analyzing and interpreting the data, and to drafting and critically revising the report. C.L., B.B., and K.N. are the guarantors of this work and, as such, had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. All authors had access to the study results, reviewed the article, and approved the final version of the report for submission.
Author Disclosure Statement
C.L. was employed by Steno Diabetes Center Copenhagen during the conduct of the study but as of November 1, 2022, is employed by, and owns shares in, Novo Nordisk. B.B. has been on the advisory boards for Medtronic, Lilly, and Novo Nordisk and has received research support from Insulet, Medtronic Diabetes, and Tandem. J.S. owns shares in Novo Nordisk and has received teacher and speaker honorarium from Medtronic, Novo Nordisk, Rubin Medical, and Sanofi Aventis. K.N. owns shares in Novo Nordisk, has been a paid consultant for Novo Nordisk and Medtronic, and has received speaker and advisory board honorarium for her institution from Medtronic, Novo Nordisk, Insulet, and Convatec, and her institution has received research funding from Zealand Pharma, Novo Nordisk, Medtronic, and Dexcom. L.E. receives salary support from National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK); has served on the advisory board of Diabetes Center Berne, Sequel, and Metronic; has received research support from Juvenile Diabetes Research Foundation (JDFR), Medtronic, Abbot and Mankind; has received consulting fees from Jaeb, Tandem Diabetes Care and Ypsomed; and has served as a speaker for Insulet. No other potential conflicts of interest relevant to this article were reported.
Funding Information
This research was supported financially by grants from the William Demant Foundation (21-2636), the Danish Diabetes Association, Julie Von Müllen’s Foundation, and A.V. Lykfeldt and Wife.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.