
Abstract
Introduction and Objective:
Most patients with type 1 diabetes (T1D) in the United States are overweight (OW) or obese (OB), contributing to insulin resistance and suboptimal glucose control. The primary Food and Drug Administration-approved treatment for T1D is insulin, which may adversely affect weight. Tirzepatide is approved for managing type 2 diabetes, improves glucose control, facilitates weight loss, and improves cardiovascular disease outcomes. We assessed the use of tirzepatide in OW/OB subjects with T1D.
Methods:
This was a retrospective single-center real-world study in 62 OW/OB adult patients with T1D who were prescribed tirzepatide (treated group) and followed for 1 year. At least 3 months of use of tirzepatide was one of the inclusion criteria. Based on the inclusion criteria, this study represents 62 patients out of 184 prescribed tirzepatide. The control group included 37 OW/OB patients with T1D (computer frequency matched by age, duration of diabetes, gender, body mass index (BMI), and glucose control) who were not using any other weight-loss medications during the same period. The mean (±standard deviation [SD]) dose of weekly tirzepatide at 3 months was 5.6 ± 1.9 mg that increased to 9.7 ± 3.3 mg at 1 year.
Results:
The gender, mean baseline age, duration of diabetes, and glycosylated hemoglobin (HbA1c) were similar in the two groups, whereas BMI and weight were higher in the treated group. There were significantly larger declines in BMI and weight in the treated group than in controls across all time points among those in whom data were available. HbA1c decreased in the treated group as early as 3 months and was sustained through a 1-year follow-up (−0.67% at 1 year). As expected, insulin dose decreased at 3 months and throughout the study period. There were no reported hospitalizations from severe hypoglycemia or diabetic ketoacidosis. The mean glucose, time-in-range, time-above-range, SD, and coefficient of variation (continuous glucose monitoring metrics) significantly improved in the treated group.
Conclusions:
In this pilot (off label) study, we conclude that tirzepatide facilitated an average 18.5% weight loss (>46 pounds) and improved glucose control in OW/OB patients with T1D at 1 year. For safe use of tirzepatide in patients with T1D, we strongly recommend a large prospective randomized control trial in OW/OB patients with T1D.
Introduction
More than 30
The use of new technologies and newer insulins in patients with T1D has improved glycemic control as measured by glycosylated hemoglobin (HbA1c) and time-in-range (TIR). However, >67% of patients with T1D in the United States are either overweight (OW) or obese (OB). 8,9 The weight gain in the past 10 years in patients with T1D may be related to improvements in technologies and lack of adjunctive treatment options, inadequate physical exercise, and inappropriate dietary choices. 10
The current American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) recommendations emphasize the choice of therapy initiation for patients with T2D should be based on associated comorbidities. 11 There are many choices for patients with T2D that include glucagon-like peptide 1 receptor agonist (GLP) such as semaglutide, glucose-dependent insulinotropic polypeptide (GIP+ GLP) such as tirzepatide, and sodium-dependent glucose cotransporter inhibitors (SGLT2i) such as empagliflozin.
The GLP analogues and SGLT2i not only improve glucose control but also have significant effects on weight loss and associated comorbidities such as cardiovascular disease (CVD) and diabetic kidney disease (DKD). 12 –14
There is a global epidemic of OW and obesity that are commonly associated with multiple comorbidities such as T2D, metabolic dysfunction-associated steatotic liver disease (MASLD), metabolic dysfunction-associated steatohepatitis (MASH), hyperlipidemia, and hyperuricemia. 10
The only viable treatment option for people with T1D is insulin. The other drug approved by the Food and Drug Administration (FDA) is pramlintide (an amylin analogue), which is rarely used because of gastrointestinal (GI) side effects, risk of severe hypoglycemia, and the need for multiple injections a day. 10,15,16 None of the newer drugs such as GLP analogues or SGLT2 inhibitors are approved for patients with T1D as an adjunctive treatment option by the FDA. Many people with T1D are OW or OB and have increased insulin resistance (IR), which contributes to inadequate glucose control despite higher insulin intake and have an increased risk of CVD and DKD. In this retrospective off-label use study, we assessed the efficacy and safety of tirzepatide use in adult patients with T1D for 1 year.
Materials and Methods
There were 184 OW and OB adult patients with T1D who were prescribed tirzepatide between June 2022 and November 2023 at the Barbara Davis Center for Diabetes in Denver. Inclusion criterion for this analysis included (1) all adult patients between ages of 18 and 80 years of age, (2) on tirzepatide for at least 3 months, (3) body mass index (BMI) ≥27 kg/m2, (4) all patients were on intensive insulin treatment using either multiple daily injections (MDIs) or on an insulin pump or a HCL system, and (5) were using a CGM. Exclusion criteria included (1) pregnant patients, (2) patients with T2D, and (3) missing data or data not available for >3 months (Fig. 1). There was no systematic protocol for ascertainment on tirzepatide discontinuation in this (off-label use) retrospective study.

Flow chart of patients included in this study.
Sixty-two patients on tirzepatide (treated group) were included in the data analysis. We excluded 122 patients due to missing data points on weight, BMI, insulin dose, lack of insurance coverage, etc., and who were incorrectly identified as having T1D. During the same time period, 37 OW or OB controls were computer-frequency matched by 5-year age groups, 10-year duration of diabetes groups, gender, BMI group (BMI 27 to <30 kg/m2, 30 to <35 kg/m2, 35 to <40 kg/m2, and 40+ kg/m2) and glucose control groups (HbA1c <7, 7–8, and >8%). Of the 62 patients in the treated group, 52 were using insulin pump/HCL system and 10 subjects were on MDI. Similarly, 32 and 5 patients were using insulin pump/HCL system in the control group, respectively.
There were 6, 52, and 4 patients using Medtronic Guardian (3 or 4), Dexcom G6, and Libre (2 or 3) CGM, respectively, in the treated group. In the control group, 4, 30, and 3 subjects were using Medtronic, Dexcom, and Libre CGM, respectively. The necessary approval by the Colorado Multiple Institutional Review Board (COMIRB) was obtained for this retrospective chart review (electronic medical records) study. The data were deidentified for further analyses.
Baseline characteristics of the study population were compared using Student's t-test for continuous variables and chi-square test for categorical variables. We analyzed change in body weight (lbs.), BMI, and CGM metrics: TIR, time-above-range (TAR), time-below-range (TBR), standard deviation (SD), and coefficient of variation (CV), HbA1c, total daily insulin dose (TDD), and basal and bolus insulin dose at 3, 6, 9, and 12 months using mixed effects linear models with repeated measures. 15,17
We examined the change in BMI, body weight in pounds, and body weight in percentage of weight loss by treatment group univariately and then in linear mixed models with repeated measures, adjusting for the baseline BMI for analysis of change in BMI, and for baseline body weight in analysis of absolute and percentage weight loss. 15,17 Similarly, we examined the change in HbA1c, insulin dose, and CGM metrics by treatment group univariately and then in linear mixed models with repeated measures, adjusting for baseline values of each parameter.
Results
Baseline characteristics of the cohorts by treatment groups are given in Table 1. The gender distribution and mean baseline age, duration of diabetes, and HbA1c were similar in the two groups. However, the mean BMI, weight, and total and basal daily insulin dose were higher in the treated (tirzepatide) group than in the control group (Table 1). The mean (±SD) dose of tirzepatide at 12 months was 9.7 ± 3.3 mg weekly (Table 1). The number of patients reaching 10, 12.5, and 15 mg weekly was 16, 6, and 6, respectively.
Baseline Characteristics by Treatment Group
Baseline demographics were similar in the two groups. However, mean baseline BMI, weight, and total and basal insulin dosages were higher in the tirzepatide-treated group. Tirzepatide initiating dose was 2.5 mg weekly that increased to 5.6 ± 1.9 and 9.7 ± 3.3 mg weekly at 3 and 12 months, respectively.
BMI, body mass index; HbA1c, glycosylated hemoglobin.
Change in BMI and body weight
Mean ± SD for changes in BMI and weight is given in Table 2. BMI decreased by 3.4 ± 2.0 and 6.5 ± 4.3 kg/m2 at 3 and 12 months, respectively, in the tirzepatide group. There were no significant changes in BMI in the control group at 3 or 12 months (Table 2). Similarly, weight decreased by 21.4 ± 13.0 lbs. (9.6%) at 3 months and by 46.5 lbs. (18.5%) at 12 months in the tirzepatide group. BMI, weight in pounds, and weight percentage decreased significantly at each time point in the tirzepatide group than in the control group (Table 2).
Changes in Body Mass Index, Weight, HbA1c and Insulin Dose Variables by Treatment Group
Data shown are mean ± SD; * P < 0.05, ** P < 0.001 for change from baseline. The BMI decreased by 3.4 ± 2.0 and 6.5 ± 4.3 at 3 and 12 months, respectively. Similarly, weight decreased by 21.4 ± 13.0 (9.6%) and 46.5 ± 28.1 (18.5%) at 3 and 12 months, respectively. Glucose control (HbA1c) improved by 0.50% ± 0.52% at 3 months and by 0.67 ± 0.56 at 1 year.
BMI, body mass index (kg/m2); HbA1c, glycosylated hemoglobin; lbs, pounds.
Changes in least square means for BMI, weight in pounds, and weight percentage over time are shown in Figure 1, adjusted for baseline values of these measures. The anthropometric measures assessed (BMI and weight) decreased significantly more over 1 year in tirzepatide users than in the controls.
Change in HbA1c
In univariate comparisons, mean ± SD HbA1c decreased significantly at all time points in the tirzepatide group, by 0.50% ± 0.52% at 3 months and by 0.67% ± 0.56% at 12 months (Table 2). The change in HbA1c in the tirzepatide group was significantly larger than in the control group at all timepoints (Table 2). When adjusted for baseline HbA1c in linear mixed models, changes in HbA1c remained significantly greater in the tirzepatide versus control group (P < 0.0001), as shown in Figure 1.
Change in insulin dose
TDD, basal, and bolus insulin dose decreased significantly in the tirzepatide-treated group at all timepoints (Table 2). In univariate comparisons, TDD, basal, and bolus insulin doses decreased to a greater extent in the tirzepatide group than in controls at all timepoints (Table 2). In linear mixed models with repeated measures adjusted for baseline dose, least square mean ± SE for TDD decreased on average by 24.7 ± 2.1 U/day in the treated group versus a decrease of 1.4 ± 2.8 U/day in controls (P < 0.0001).
Similarly, when calculated as the TDD per kilogram body weight, the dose decreased significantly more in the tirzepatide group (−0.33 ± 0.02 U/[kg·d]) than in controls (0.01 ± 0.02, P < 0.0001). Basal insulin doses decreased by 9.7 ± 1.0 U per day in treated group versus a decrease of 1.5 ± 1.4 U per day in controls (P < 0.0001), and bolus insulin decreased by 14.7 ± 1.4 U a day in treated group versus a decrease of 0.3 ± 1.9 U per day in controls (P < 0.0001).
Change in CGM variables
Mean CGM glucose decreased significantly at all timepoints, by 16.8 ± 17.9 mg/dL at 3 months and by 23.5 ± 29.2 mg/dL at 12 months in the tirzepatide group but did not change at any time point in controls (Table 3). The decreases in mean CGM glucose were significantly greater in the tirzepatide group than in the control group at 3, 6, and 12 months.
Change in Continuous Glucose Monitoring Metrics by Treatment Group
Data shown are mean ± SD; * P < 0.05, * P < 0.001 for change from baseline.
CV, coefficient of variation; SD, standard deviation; TIR, time-in-range (70–180 mg/dL); TAR, time-above-range (>180 mg/dL), TBR, time-below-range (<70 mg/dL).
TIR increased in the tirzepatide group by 10.5% ± 10.2% at 3 months and by 12.5% ± 15.0% at 12 months, although the change at 12 months did not reach statistical significance. The change in TIR was not significant at any timepoints in the control group, and the change in TIR was significantly greater in the tirzepatide group at 3 and 6 months than in the control group (Table 3). TAR decreased significantly at all timepoints in the tirzepatide group and in none of the timepoints in the control group (Table 3 and Fig. 3). Greater decreases in TAR were observed in the tirzepatide group than in control group at 3, 6, and 9 months (Table 3). TBR did not change significantly in either group at any timepoint, and there were no group differences in the change in TBR by group (Table 1S).
Glucose SD decreased from baseline at all timepoint in the tirzepatide group but in none of the timepoints for the control group (Table 3), with significantly larger decreases in glucose SD for the tirzepatide group at 6, 9, and 12 months when compared with the control group (Table 3). CV decreased significantly from baseline in the tirzepatide group at 6 and 9 months and did not change significantly in the control group at any timepoint. However, there were no significant differences in CV change by group at any timepoint (Table 3).
In mixed models with repeated measures, there were significantly greater decreases in mean CGM glucose (P = 0.0006), TAR (P = 0.0002), glucose SD (P < 0.0001), and CV (P = 0.0054), and significantly greater increases in TIR in the tirzepatide group than in the control group (Figs. 2 and 3).
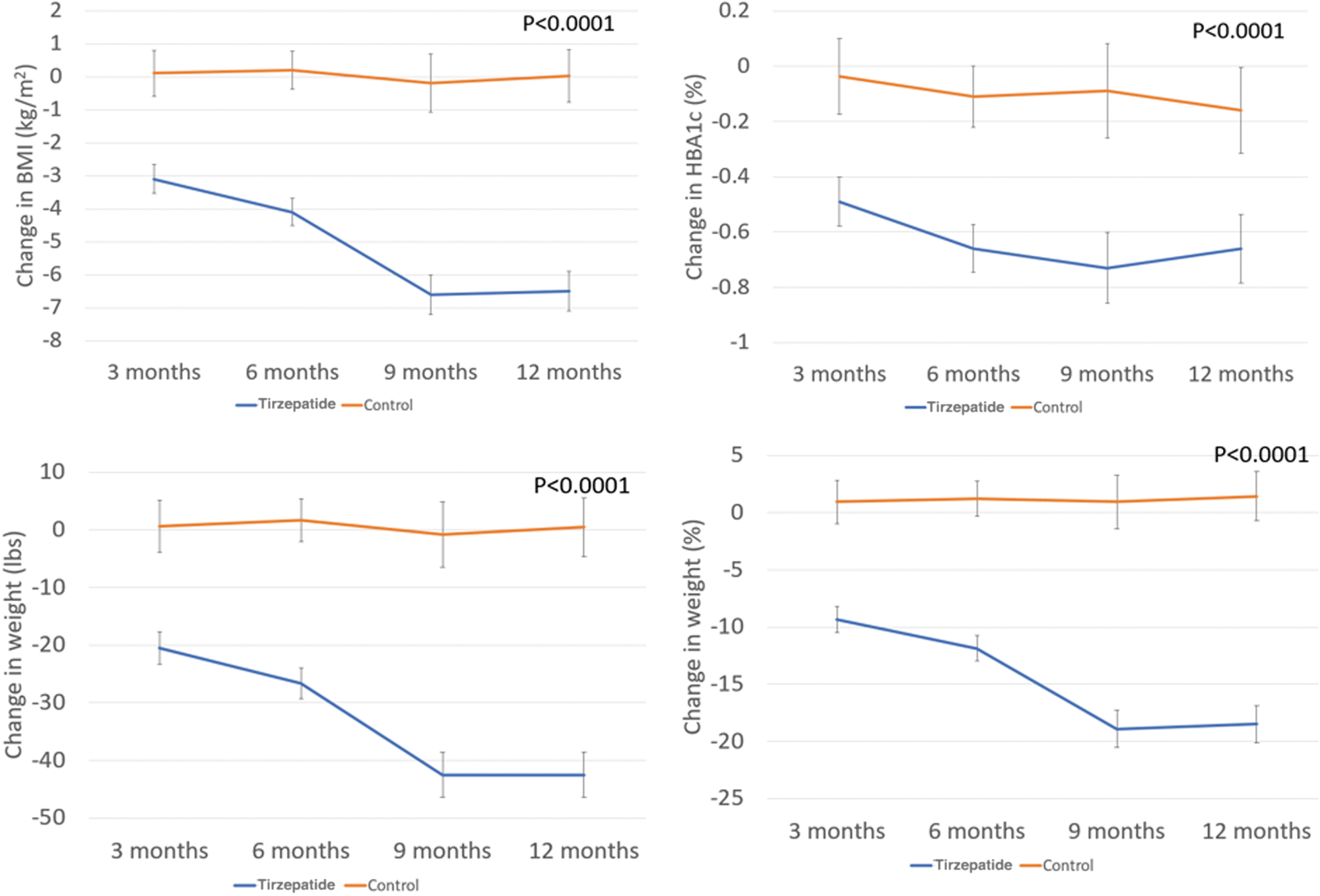
Change in BMI, weight (pounds and percent), and HbA1c over 12 months by treatment group. BMI, body mass index; HbA1c, glycosylated hemoglobin.
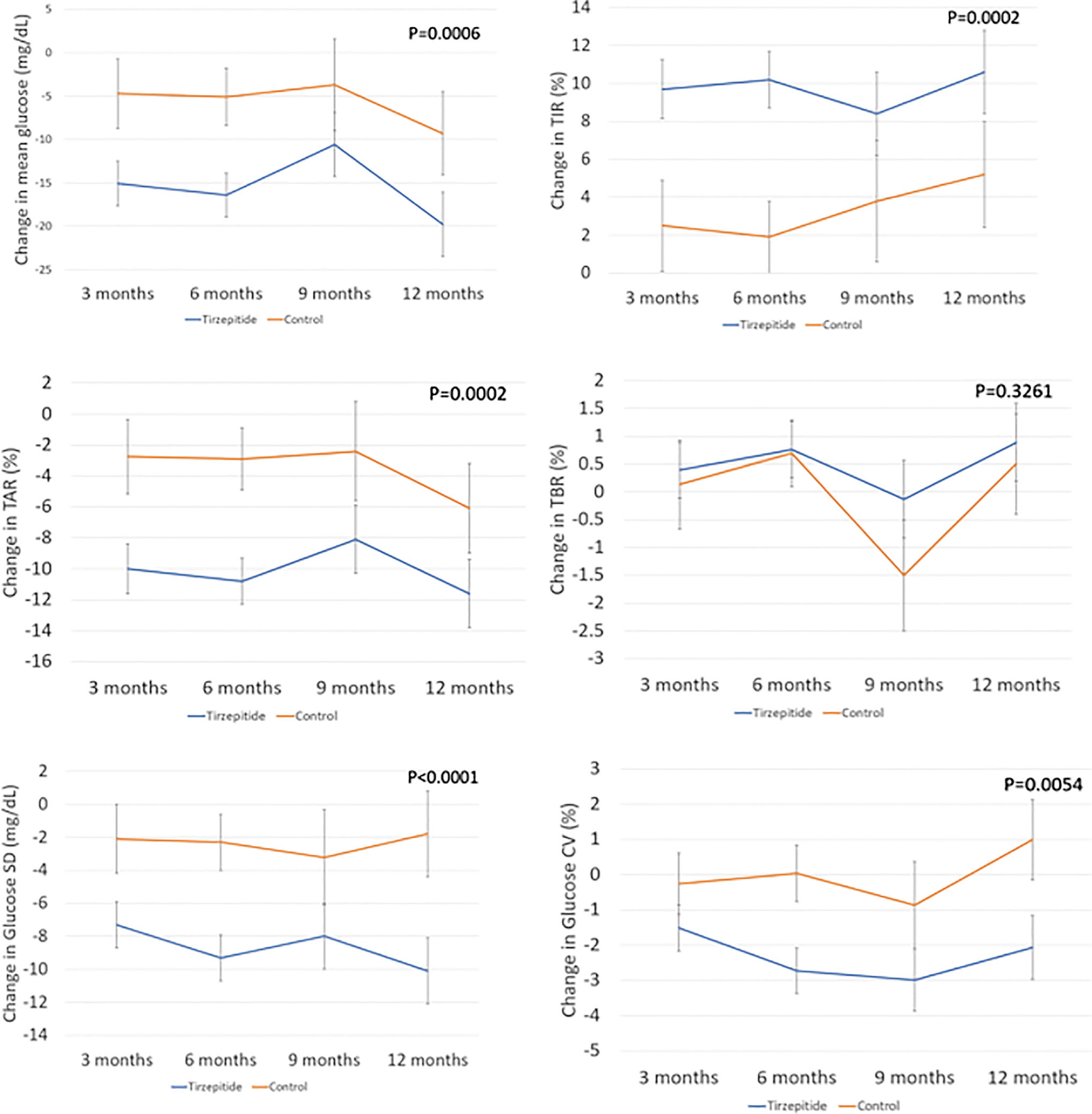
Change in CGM metrics over 12 months by treatment groups. TAR, SD, CV and TIR significantly improved throughout the study duration. The TBR was not significantly different in the 2 group throughout the study duration. CGM, continuous glucose monitoring; CV, coefficient of variation; SD, standard deviation; TAR, time above range; TBR, time below range; TIR, time in range.
Discussion
We report that use of tirzepatide in real life in OW and OB adult patients with T1D resulted in significant weight loss and change in BMI at 1 year. Patients in the tirzepatide treated arm lost >46 pounds (18.5%) with a decrease in BMI of −6.5 ± 4.3 kg/m2 at 1 year. The mean ± SD tirzepatide dose at the end of 1 year was 9.7 ± 3.3 mg per week. The majority of patients in this study did not reach the full 15 mg dose of tirzepatide as recommended for patients with T2D. The weight loss was >2 times higher in this study than in those treated with semaglutide as previously reported. 10
All patients stayed on intensive insulin treatment (MDI or HCL system) throughout the study period. The differences in weight and BMI change between the two groups using MDI or HCL system will be the topic of a future report.
Tirzepatide is a twincretin (GIP+GLP) with its predominant effects through GIP on HbA1c and weight loss. 18 Since the drug has significant GI side effects such as nausea, vomiting, diarrhea, and/or constipation, tirzepatide dose escalations should be done gradually every month in patients with obesity associated with or without T2D. All adult T1D patients in this study were initiated on tirzepatide 2.5 mg weekly. However, the dose increases were done slower based on our clinical experience (every 1–2 months) to minimize side effects. 19
Excessive weight gain is associated with inadequate control in patients with T1D in the T1D Exchange study cohort. 20 Increased body weight also results in IR and higher insulin needs to adequately control glycemia. In this study, there was a significant decrease in TDD at the end of 1 year that started as early as 3 months. Despite decrease in TDD, there was an improvement in glucose control in the treated group at 1 year when compared with the control group (−67%; P < 0.004).
All patients wore CGM throughout the study with or without an insulin pump or HCL system. Corresponding to improvement in the glucose control as measured by HbA1c values, TIR between 70 and 180 mg/dL was significantly higher throughout the study in the treated group (CGM data). Similarly, TAR >180 mg/dL was significantly lower in the treated group than in controls at 1 year with no change in TBR throughout the study duration. The SD and CV for glucose values were also lower after 6 and 9 months in the tirzepatide-treated group than in controls.
There were no reported hospitalizations from severe hypoglycemia or diabetic ketoacidosis (DKA) in this study from both cohorts. Since insulin dose decreases significantly to avoid hypoglycemia with tirzepatide treatment, this may put patients at higher risk for DKA especially those on an insulin pump or an HCL system. The risk of DKA adds extra cost and inconvenience for daily ketone monitoring. The continuous ketone monitoring (CKM) may become available like CGM on the same sensor that was announced during the Annual ADA Scientific Session meeting in New Orleans, LA, by Abbott in June 2022. 21
There have been several recent reports on short-term side effects in patients treated with tirzepatide. 22 These include gastroparesis, acute bowel obstruction, pancreatitis, gall bladder stone, and cholecystitis. 22 Recently we reported some of the challenges of using off-label tirzepatide in adult patients with T1D and the best clinical practices to avoid such risks. 19 Long-term side effects of tirzepatide are not known as the drug has only been available for <2 years.
Tirzepatide (MounjaroR) was approved for T2D in May 2022 and ZepboundR was approved in November of 2023 for weight management in patients with BMI >27 kg/m2 associated with at least one comorbidity. 23 To the best of our knowledge, this is the first report of its use in OW and OB patients with T1D for up to 1 year. The strengths of our article include real-world use of antiobesity drug in OW and OB patients with T1D, follow-up for 1 year, computer-matched controls during the same time period, assessment of CGM metrics, and glucose control (HbA1C) throughout the study period.
The weaknesses are retrospective chart review, small sample size, lack of systematic/structured protocol for initiating tirzepatide, off-label use of tirzepatide in patients with T1D, lack of data from diverse populations (∼90% of subjects were non-Hispanic Caucasians), and data from different CGMs in both cohorts. In addition, we had data for only 50% (92 out of 184 were excluded in the final analyses due to lack of data beyond 3 months) of the subjects beyond 3 months of use of tirzepatide. There were insufficient OW or OB patients available for one-to-one matching, and although matching variables did include BMI, frequency matching was done and there was a difference in BMI at baseline.
It remains to be determined whether patients with T1D will need to stay on tirzepatide to maintain body weight especially due to cost burden and long-term safety concerns. The patients on GLP analogue may be at high risk of getting sarcopenia and other nutritional deficiencies and many pharmaceutical companies are going to address this concern by focusing myostatin antibody. 24 Also, it is not known whether lower dosages of tirzepatide will be required to maintain the body weight without significant side effects in patients with OW and OB patients with T1D as an adjunctive treatment. 19
It is also imperative to adjust insulin doses to prevent hypoglycemia while using tirzepatide in patients with diabetes. Every attempt (with proper counseling for lifestyle modifications) should be made to discontinue tirzepatide treatment since its use is off label in patients with T1D. 19 However, the data from patients with T2D with or without obesity show that only <20% can keep their weight off once the drug is discontinued. 25
Conclusions and Summary
We conclude that in this pilot study, tirzepatide was safe and effective in lowering body weight in OW and OB adult patients with T1D at 1 year. We also report significant improvements in glucose control as measured by HbA1c or TIR, TAR, SD, and CV. Since weight loss is significant in OW and OB patients with T1D, it is likely that patients with T1D would benefit in the long run from reductions in CVD and DKD. We strongly recommend of doing large randomized control trials in this high-risk patient population to avoid off-label and ensure safe use of tirzepatide.
Footnotes
Acknowledgments
We acknowledge the hard work of all the educators and providers in the Adult Clinic at the Barbara Davis Center for Diabetes for initiating and educating patients on safe use of tirzepatide in patients with T1D. We thank Bing Wang for data downloads from EPIC.
Authors' Contributions
All authors contributed to data collection, writing, and editing of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No external funding or support for this study report.