
Abstract
Aims/Hypotheses:
To investigate the frequency and characteristics of partial remission in Swedish children with type 1 diabetes and whether the insulin delivery method, that is, continuous subcutaneous insulin infusion (CSII) or multiple daily injections (MDIs), affects incidence and duration of this period, 2007–2011. Factors that increase the proportion of subjects who enter partial remission and extend this period can improve long-term metabolic control and reduce the risk of severe hypoglycemia, improve quality of life, and, in the long run, reduce late complications.
Methods:
Longitudinal data from 2007 to 2020 were extracted from the Swedish National Quality Register (SWEDIABKIDS) with all reported newly diagnosed children. Data on C-peptide from the participants in the Better Diabetes Diagnosis study from 2007 to 2010 were used. The definition of partial remission was insulin dose–adjusted HbA1c: HbA1c (%) + [4 × total daily insulin dose (U/kg/day)] ≤9.
Results:
Of the 3887 patients, 56% were boys. More boys than girls were in partial remission throughout the follow-up period until 24 months after diabetes onset. Fewer children 0–6 years old had partial remission at 3 and 12 months but not at 24 months compared with older age-groups. A larger proportion of patients using CSII at 12 and 24 months remained in partial remission compared with those with MDI (37% vs. 33%, P = 0.02 and 31% vs. 27%, P = 0.01, respectively). The level of C-peptide was higher in the group with partial remission and mean HbA1c was lower (both P < 0.001). Partial remission at 12 months after diabetes onset was associated with CSII (odds ratio [OR]: 1.39, confidence interval [CI]:1.13, 1.71), shorter diabetes duration (OR: 0.80, CI: 0.76, 0.84), and male sex (OR: 1.23, CI: 1.04, 1.46).
Conclusions/Interpretation:
Insulin through MDI, longer duration of diabetes, and female sex were associated with lower frequency of partial remission. Use of CSII seems to contribute to longer partial remission among Swedish children with type 1 diabetes.
Introduction
In the vast majority of children and adolescents who have recently developed type 1 diabetes, the need for insulin decreases temporarily some weeks after insulin treatment is started. 1 This is due to a partial recovery of the beta cells where they regain their ability to secrete insulin as well as an increased peripheral insulin sensitivity. The partial remission period, often referred to as the “honeymoon phase,” can last for weeks to several years and is characterized by relatively stable glucose levels (within the normal range) despite variations in diet and physical activity. 2 By identifying factors that increase the proportion of those who enter partial remission and its duration, metabolic control could be improved, 3 and the risk of late complications could be reduced. 4 Several studies indicate that a combination of inflammatory, hormonal, immune, and genetic factors predicts the occurrence and duration of partial remission. 5 –9 At present, there are some immunological, disease-modifying treatments that aim to stop the decline in beta-cell function. 10 –12 To date, there is, however, no treatment that can restore beta cell function for an extended period of time, and therefore, it is still important to try to preserve as much beta cell function as possible as studies have shown that this reduces the risk of developing vascular complications, ketoacidosis, and severe hypoglycemia. 13 –16 Residual beta cell function is reflected in maintained secretion of C-peptide, which seems to have physiological properties on its own, for example, improve the microvascular blood flow and endothelial function through the release of endothelial nitric oxide. 17,18
Previous studies have shown that ketoacidosis, young age, and infection at onset reduce the likelihood of an extended partial remission phase. 19 –22 It has, however, been difficult to compare studies of partial clinical remission since there have been many different definitions. 2,20,23 –27 We used the internationally accepted definition for partial remission insulin dose–adjusted HbA1c (IDAA1c) as there is a need of comparable data in a time when disease-modifying therapies are coming.
The aim of this retrospective study using real life data was to investigate the frequency and characteristics of the group with partial remission up to 24 months after diagnosis using the IDAA1c definition. In addition, we wanted to study whether the chosen method of insulin delivery was associated with the incidence and duration of this period as well as with the incidence of severe hypoglycemia or ketoacidosis. Finally, we wanted to compare the clinical definition for partial remission used in Sweden, that is, total insulin dose <0.5 U/kg/day and HbA1c <57 mmol/mol (7.4%), as this was the target for HbA1c during this time period 28 with the internationally accepted IDAA1c. 24
Patients and Methods
The study population consisted of (a) all children 0–17.99 years of age with newly diagnosed type 1 diabetes, as reported to the Swedish National Diabetes Register for Pediatric Diabetes (SWEDIABKIDS) and (b) the participants in the Better Diabetes Diagnosis study (BDD). The definition of type 1 diabetes was typical symptoms of diabetes and P-glucose ≥11.1 mmol/L (≥200 mg/dL) or fasting P-glucose ≥7.0 mmol/L (≥126 mg/dL). 28 The period 2007–2020 was studied: the duration of 2007–2011 was selected because the BDD study had analyzed C-peptide in the participants twice during these years, at the diagnosis of type 1 diabetes and after 1 year. As there have been large improvements in diabetes care the last decade, we decided to also include a cohort from 2012 to 2020 to explore the continued prevalence of partial remission (Fig. 1). Data extracted were date for diabetes diagnosis, sex, insulin delivery method, longitudinal data on total daily insulin dose, C-peptide, and HbA1c. We used two definitions of partial remission as follows: (a) IDAA1c: HbA1c (%) + [4 × total daily dose of insulin (U/kg/day)] ≤9 24 and (b) the definition used clinically in Sweden at the time, defined as a total insulin dose <0.5 U/kg/day and a HbA1c <57 mmol/mol (7.4%), as this was the target for HbA1c during this period 28 (abbreviated PR). Our study was approved by the Swedish Ethics Review Authority (2014/2011-31 and 2020–05894).
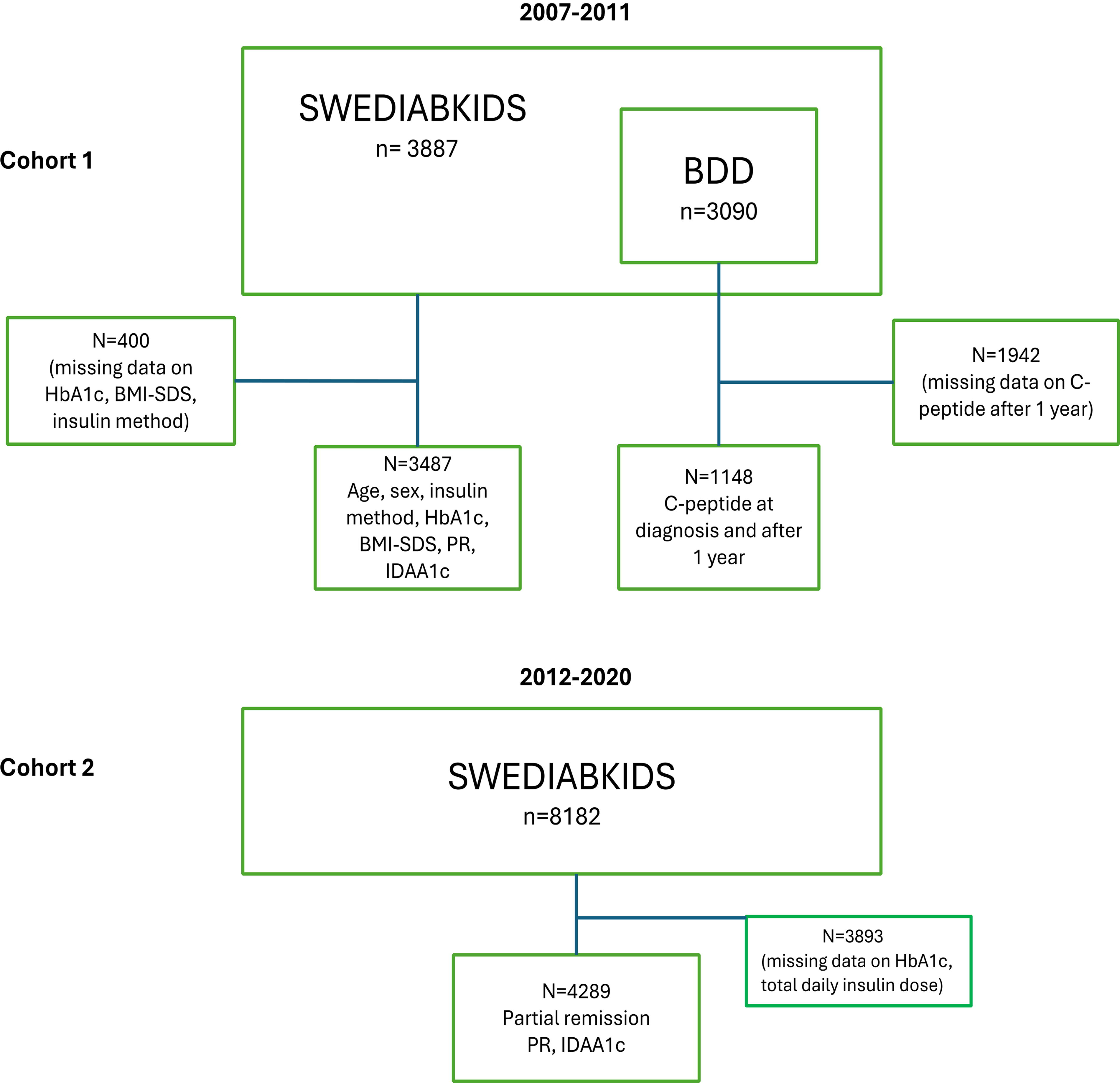
Flowchart over the two cohorts. BDD, Better Diabetes Diagnosis study group; BMI, body mass index (kg/m2); IDAA1c, insulin dose–adjusted A1c [HbA1c % + 4 × total daily dose (U/kg/day)] ≤ 9; PR, partial remission defined as insulin <0.5 U/kg/day and HbA1c <57 mmol/mol (7.4%); SDS, standard deviation score.
SWEDIABKIDS
All 43 pediatric clinics in Sweden have registered their patients since 2007 to SWEDIABKIDS, resulting in a coverage of nearly 98% for prevalent cases, 29 and the register is repeatedly validated against the Swedish Prescribed Drug Register for incident cases. 30 The Prescribed Drug Register is maintained by the National Board of Health and Welfare and covers all redeemed medical prescriptions since July 2005.30 Since 2008, SWEDIABKIDS has been web-based, and clinical data are recorded prospectively from every patient visit to the outpatient pediatric clinics, which is usually three to four times per year per patient. At each visit, anthropometrical data (weight and height), HbA1c, insulin method, total insulin dose, and incidences of severe hypoglycemia and ketoacidosis were recorded. Severe hypoglycemia was defined as blood glucose <3.9 mmol/L (70 mg/dL) together with an event involving seizure or unconsciousness, and ketoacidosis was defined as pH <7.3. Data for the present study were collected from each patient 3, 12, and 24 months after diagnosis of type 1 diabetes. As the dates for the visits were not exactly on time, we used the intervals 2–4, 11–13, and 23–25 months. We analyzed the groups with the insulin method that they had at the time of the visit, and individuals with partially missing data were only included in the analysis where data were present. We analyzed the group having missing data and saw that there were somewhat more boys (59%), more patients in the oldest age-group, and more use of multiple daily injection (MDI) as insulin method. We wanted to include ketoacidosis at diagnosis, but this was not possible as these data were not available during this time period. In 2011, data from 6861 unique patients up to 17 years of age were recorded in SWEDIABKIDS from 26,004 visits. 31 From 2007 to 2011, on average, 806 patients per year were recorded with newly diagnosed type 1 diabetes, and in 2012–2020, on average, 885 patients per year were recorded. SWEDIABKIDS was in 2018 integrated into the Swedish National Diabetes Register (NDR), with patients with diabetes >18 years of age, and is now referred to as NDR.
BDD
BDD is a prospective national study that started in 2005 in Sweden to classify the type of diabetes in all newly diagnosed children and adolescents 0–17 years of age. This ongoing study recruits patients from all of the 43 pediatric clinics in Sweden. Blood samples are collected and analyzed for auto-antibodies, Human Leukocyte Antigen (HLA) genotype, and levels of C-peptide at diagnosis. In 2006, ∼75% of all children and adolescents with newly diagnosed diabetes in Sweden were registered in the study, and at present, the coverage is over 95%. 32 Between 2005 and 2010, C-peptide was analyzed in the BDD study at diabetes diagnosis and after 1 year. 32 In the present study, 1148 patients were included from the BDD study (during 2007–2010) having C-peptide values registered at diagnosis of type 1 diabetes and after 1 year. Missing data on C-peptide were 63%, mainly because of missing data at the 1-year follow-up with no further analyses performed on those patients (Fig. 1). Since 2011, analyses of HLA profile, auto-antibodies (GADA, IA-2A, IAA, ZnT8A), and C-peptide levels are part of clinical routine in Sweden for all pediatric patients with a diagnosis of diabetes. However, no systematic follow-up of C-peptide is available.
Biochemical analysis
Serum C-peptide was measured from random nonfasting blood samples collected at diagnosis before the first insulin dose was administered and at a nonfasting random sample 1 year later. The samples were analyzed at the Department of Pediatrics, Linköping University, Sweden, with a time-resolved fluoroimmunoassay (AutoDELFIATM C-peptide kit, Wallac, Turku, Finland), with a detection level of 0.03 nmol/L. Each assay was validated by inclusion by a C-peptide control module, containing a high-, medium-, and a low-level control (Immulite, DPC, UK). A 1224 MultiCalc© program (Wallac) was used to calculate the levels of C-peptide. 33 At the different hospitals participating in SWEDIABKIDS, analyses in HbA1c are performed according to different laboratory methods. These are quality assured through Equalis (External Quality Assurance in Laboratory Medicine in Sweden), 34 which makes it possible to compare HbA1c values across different clinics. HbA1c is presented as International Federation of Clinical Chemistry and Laboratory Medicine (IFCC) units (mmol/mol) and National Glycohemoglobin Standardization Program (NGSP) units (%). 35 The conversion of HbA1c from IFCC (mmol/mol) to NGSP (%) was done using the tool provided by the National Glycohemoglobin Standardization Program. 36
Statistical analyses
The annual data were stratified according to the insulin delivery method, continuous subcutaneous insulin infusion (CSII) versus MDI, sex, partial remission status (IDAA1c ≤9 vs. IDAA1c >9) or according to the Swedish, clinical remission definition, age at diagnosis group (0–6, 7–12, 13–17 years old), and duration group (0–3, 3–12, 12–24 months after diabetes diagnosis). We stratified the groups being in partial remission at 3 months, after 1 year, and still in partial remission after 2 years. The age-groups were based on major clinical differences in developmental psychology, ability to self-care, bodily maturation, and hormonal impact on the glucose metabolic control. All statistical analyses were performed using SPSS version 27 (IBM Inc., Armonk, NY, USA). For normally distributed data, differences between groups were tested with independent two-sample t-tests. A nonparametric Mann–Whitney U test was used to compare the skewed data on C-peptide between groups. The interquartile range (IQR) was calculated by subtracting the 75th and 25th percentile of the median. To account for the repeated measurements, a generalized linear mixed regression model was performed, where the outcome was being in remission at each time point and independent variables/factors were insulin delivery method, sex, age at diagnosis, and duration of diabetes, and individuals were treated as a random factor. Statistical significance was defined as P < 0.05 (two-sided).
Results
Baseline data are presented in Table 1. In total, data from 3887 patients (56% boys) from 0 to 17 years of age were available. Girls were younger (mean age 9.2 years) at diagnosis of diabetes than boys (mean age 10.1 years). There were more patients with partial remission using the IDAA1c definition compared with the Swedish clinical definition, that is, 48% versus 36% at 3 months, 33% versus 14% at 12 months, and 26% versus 5% at 24 months. The relative proportion of patients in partial remission according to the IDAA1c definition at 3 months increased from 45% in 2007 to 51% in 2011. To investigate if this increase continued, we analyzed the years from 2012 to 2020, which showed that there was an increase in the frequency of partial remission between 2007–2011 and 2012–2020 of ∼5% (Fig. 2).
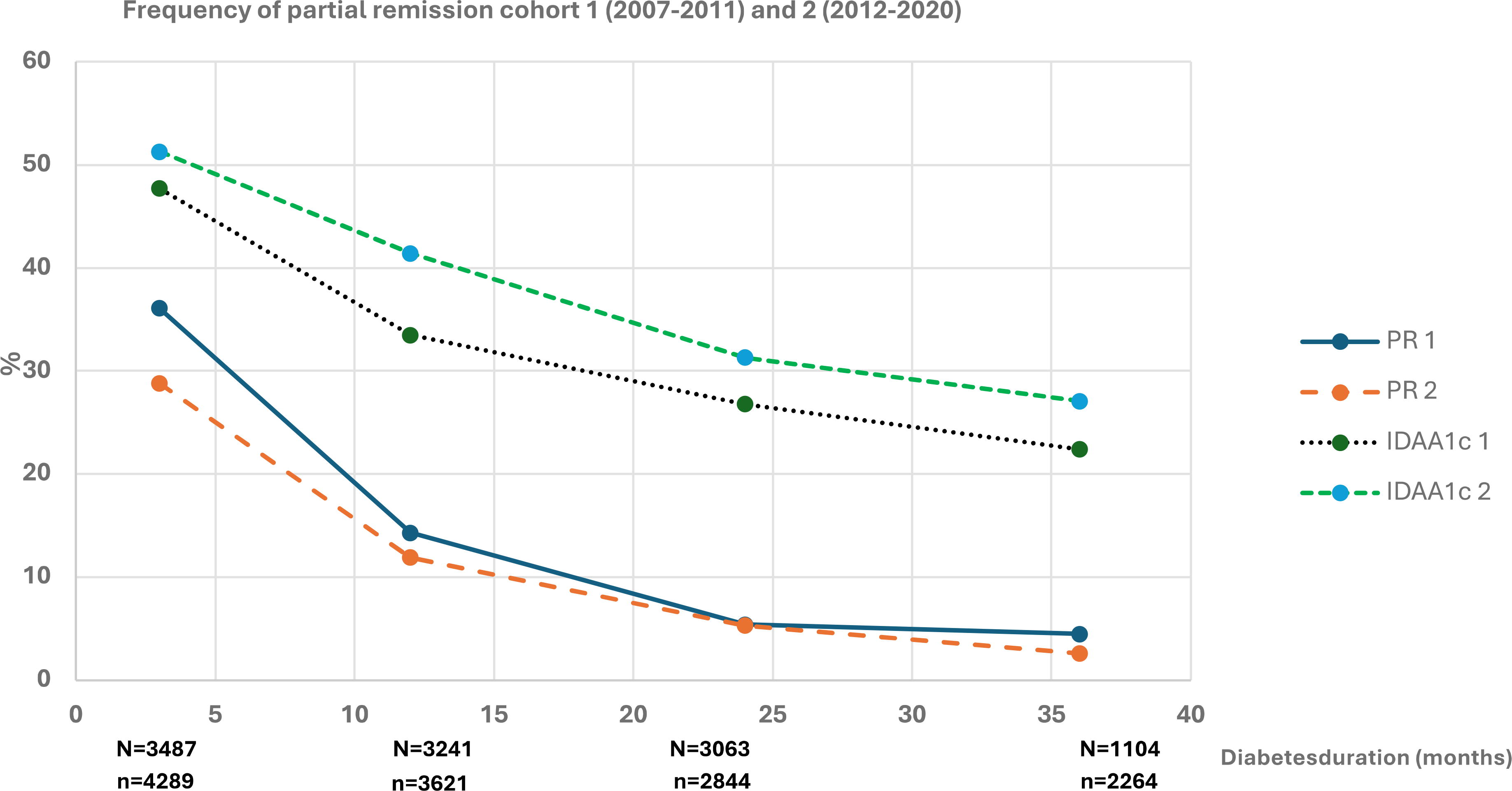
PR frequency at 3, 12, 24, and 36 months during the years 2007–2011 (PR 1 [solid blue] and IDAA1c 1 [dotted dark green]) and 2012–2020 (PR 2 [dashed orange] and IDAAC1 2 [dashed light green]) with remission defined as PR = total insulin dose <0.5 U/kg/day + HbA1c <57 mmol/mol (7.4%) and IDAA1c = HbA1c (%) + [4 × total daily dose (U/kg/day)] ≤9; N = the number of individuals having available data on HbA1c and total daily insulin dose (U/kg/day) at each time point in cohort 1 (2007–2011); n = the number of individuals having available data on HbA1c and total daily insulin dose (U/kg/day) at each time point in cohort 2 (2012–2020).
Baseline Data from 2007 to 2011 for New-Onset Type 1 Diabetes in Children 0–17 Years of Age Stratified for Sex and Prevalence of Partial Remission at 3, 12, and 24 Months Duration
Values presented are numbers, percentages, means with SDs.
BMI, body mass index (kg/m2); IDAA1c, insulin dose–adjusted A1c [HbA1c % + 4 × total daily dose (U/kg/day)] ≤ 9; PR, partial remission defined as insulin <0.5 U/kg/day and HbA1c <57 mmol/mol (7.4%); SD, standard deviation; SDS, standard deviation score.
Sex and age
More boys than girls were in partial remission throughout the follow-up period until 24 months after diabetes onset (Table 2). There were fewer children in the youngest age-group (0–6 years) in partial remission at 3 and 12 months but not at 24 months compared with the older age-groups (Table 2).
Prevalence of Partial Remission Stratified for Sex, Age Groups, Insulin Method, and Severe Events for Duration Groups of 3, 12, and 24 Months
Data do not always sum up to population totals because of partially missing data.
P-values are difference between groups within each definition of partial remission.
Hypoglycemia: P-glucose <4 mmol/L and unconsciousness or seizures.
CSII, continuous subcutaneous insulin infusion; MDI, multiple daily injections; NS, nonsignificant.
Insulin delivery method
Patients who were treated with CSII remained to a larger extent in partial remission compared with those treated with MDI, 37% versus 33% at 12 months, and 31% versus 27% at 24 months, respectively (Table 2). There were significantly less incidents with hypoglycemia and ketoacidosis among children with partial remission at 12 and 24 months (P < 0.05; Table 2).
C-peptide
Serum C-peptide at diagnosis was higher in the group that later entered partial remission as well as after 1 year, and mean HbA1c was lower (Table 3). The C-peptide values correspond to the different duration groups (0–3, 3–12, and 12–24 months after diabetes diagnosis) being in partial remission.
Median C-Peptide Levels and Mean HbA1c at 3, 12, and 24 Months of Duration of Type 1 Diabetes Stratified by Definition of Partial Remission
Median (interquartile range).
Mean ± standard deviation.
However, there was no distinct level of C-peptide at diagnosis that could predict later partial remission due to a large overlap.
Regression analysis
Factors associated with partial remission were further analyzed with logistic regression, with each time point (3, 12, and 24 months after diabetes onset) modeled separately (Table 4). Partial remission was associated with CSII throughout follow-up. There was somewhat increased likelihood of partial remission in boys compared with girls: 20% at 3 months (odds ratio [OR]: 1.20, 95% CI: 1.00, 1.43), 23% at 12 months (OR: 1.23, 95% CI: 1.04, 1.46), and 25% at 24 months (OR: 1.25, 95% CI: 1.05, 1.50). The longitudinal analysis was a nominal regression with partial remission at 3 months and still in partial remission at 12 and 24 months as the dependent variable, and age at onset, sex, insulin delivery method, and diabetes duration as the independent variables suggested that the insulin delivery method at 3 months may be associated with reaching partial remission, although the analyses did not reach statistical significance (data not shown). However, subgroup analysis for the group being in partial remission having data from 3, 12, and 24 months indicated that insulin pump treatment at 3 months increased the probability of reaching partial remission and maintaining it for 24 months (OR: 3.26, 95% CI: 1.10, 9.69).
Odds Ratios for Partial Remission at 3, 12, and 24 Months After Onset of Type 1 Diabetes in Children 0–17 Years of Age
Each definition modeled separately.
aOR, adjusted odds ratio; CI, confidence interval; cOR, crude odds ratio; OR, odds ratio.
Discussion
In the present study of 3887 Swedish children and adolescents with newly diagnosed type 1 diabetes from 2007 to 2011, we found that young age at diagnosis, female sex, lower levels of C-peptide at diagnosis, and insulin administered through MDI were associated with lower frequency of partial remission. In our study, we defined partial remission as IDAA1c and compared it with the definition used in Sweden (PR, total insulin dose <0.5 U/kg/day and HbA1c <57 mmol/mol [7.4%] at the time when our patients were diagnosed), which is not based on the degree of residual beta cell function. As CSII treatment is associated with lower insulin dose/kg/day compared with MDI treatment and the Swedish clinical definition of partial remission is based on total insulin dose, this could affect the results. There are limitations using HbA1c or IDAA1c to define partial remission as it can be difficult for patients having a very high HbA1c at diagnosis of type 1 diabetes to reach HbA1c <57 mmol/mol (<7.4%) 3 months after diagnosis even though they are in partial remission with a very low total insulin dose. The finding that boys more often than girls enter partial remission was previously reported by Örtqvist et al. 21 and that boys have a longer duration of partial remission compared with girls by Bober et al. 19 In the present study, this gender difference remains over time, and at 24 months, there were still more boys in partial remission than girls. We found that girls were approximately a year younger at the onset of diabetes compared with boys (mean age 9.2 vs. 10.1 years). This could be due to the relative insulin resistance, which is more pronounced in prepubertal girls than in boys. 37 However, in the logistic regression model, younger age at onset in girls could not explain the gender difference in partial remission rate. Recent studies have highlighted a number of sex-related differences both at diagnosis and during treatment of type 1 diabetes that may explain the lower chance of remission seen in girls in this study. Apart from the effects from sex hormones, for example, estrogens on insulin resistance even in late prepubertal girls and throughout adolescence producing higher HbA1c at diagnosis as well as during treatment, differences in the distribution of body fat, growth hormone profiles, treatment biases, coping mechanisms, and health-related quality of life may all affect glycemic control and lower the chance to reach remission in girls compared with boys. 38
Young age (0–6 years of age at diagnosis) was associated with lower frequency of partial remission during follow-up, which is consistent with the findings in previous studies. 21,39 Grönberg et al. demonstrated that younger age at diagnosis predicted lower C-peptide levels, which could be explained by a more aggressive form of the disease or an overall lower beta cell mass in younger children. 16
The frequency of partial remission at 3 months increased during the study period, from 2007 to 2011, and during this time, CSII treatment increased from 32% to 42%. 31 We could identify a further increase in the frequency of partial remission during the period 2012–2020, and there have been large improvements in diabetes care during the last decade with advancements in technology, continuous glucose monitoring (CGM), carbohydrate counting, and support from the diabetes teams, which have led to a general decrease in HbA1c. 29 As data on CGM usage were not registered during this time period (2007–2011), we were not able to include these in the analysis. Recently a new therapy with monoclonal anti-CD3 antibodies (teplizumab) has been authorized by the Federal Drug Administration in the United States for the treatment of individuals with multiple autoantibodies and type 1 diabetes in stage 2, as studies have shown that teplizumab treatment may preserve residual beta cell function for several years. 10
Total daily insulin dose (U/kg/day) in association with metabolic control indirectly reflects the endogenous insulin production, whereas C-peptide is a direct measure of endogenous insulin production. The Diabetes Control and Complications Trial study showed that intensive insulin therapy (MDI or insulin pump) reduced the risk of C-peptide loss by more than 50%, suggesting that metabolic control is associated with the maintenance of beta cell function. 40 C-peptide levels >0.2 nmol/L at diagnosis and during the first year reduced the incidence of microvascular complications (retinopathy) and severe hypoglycemia. 15,16 In the present study, mean C-peptide levels were above this threshold during the first 2 years after diagnosis. However, 40% were below <0.2 nmol/L, which may increase the risk of long-term complications. There seemed to be less incidents of severe hypoglycemia and ketoacidosis in the partial remission group compared with the group without partial remission, which indicates a more stable glucose control, but these events were rare in both groups, making it difficult to draw firm conclusions.
Patients with CSII treatment remained in partial remission to a larger extent at 12 and 24 months compared with the MDI group, which was confirmed by the logistic regression analysis. Our results contradict the finding of Boughton et al. where intensive glucose control in youth 10–17 years of age with new-onset type 1 diabetes with advanced hybrid closed-loop therapy for 24 months did not appear to prevent the decline in residual C-peptide secretion. 41 Another study by Enander et al. showed that residual beta cell function at 2 years seemed to be independent of initial insulin regimens but related to HbA1c and C-peptide at onset. 42
As the C-peptide level at diagnosis of type 1 diabetes was determined before administration of insulin, one can assume that the blood glucose level was very high. A weakness of this study is that we do not have any valid blood glucose values when C-peptide was analyzed a year after diagnosis of type 1 diabetes as this blood sample was taken nonfasting and at a randomly chosen time and not after a mixed-meal tolerance test. Another weakness is that we do not know the reason for starting CSII treatment. During this period, it was mainly young children who received CSII treatment or patients with difficulties achieving a good metabolic control with MDI treatment. There were more girls than boys having CSII treatment, which could be because of health care practitioners providing them with insulin pumps in an attempt to improve their metabolic control. There were a larger proportion nonremitters in the group with young children, and they could have had good glucose control with CSII but a poor beta cell function. During this period, the frequency of CSII usage increased, and there was a difference between different participating centers, which could be a bias in the analysis and is a weakness of the study. The costs for insulin pumps in Sweden are covered by the national health care system, and the patients and their families do not have any costs for either insulin or the technology. There is no standardized curriculum in Sweden for how to start CSII treatment in a patient, so this procedure varies between different pediatric clinics. Another weakness of the study is that the registration of the total daily insulin dose was based on recall at the time of the visit to the pediatric clinic as the use of internet-based systems to download data from insulin pumps was not yet in practice. A potential bias could be the usage of CGM, which was not registered in the NDR during the time period 2007–2011. A strength of this study is the number of patients and the coverage of the registers SWEDIABKIDS and BDD, which improve the external validity. To conclude, we found that insulin through MDI, longer duration, and female sex were associated with lower frequency of partial remission. Use of CSII seems to contribute to longer partial remission among Swedish children with type 1 diabetes.
Footnotes
Acknowledgment
The authors would like to thank Ulf Söderström for the contribution to the design of the study.
Authors’ Contributions
A.-L.F. contributed to the design of the study, collected and analyzed the data, wrote the first draft of the article, and reviewed end edited the article. She is further the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. M.B. assisted with the statistical analysis and reviewed and edited the article. A.C. and G.F. contributed to the discussion and reviewed and edited the article. M.L. contributed to the design of the study, collected and analyzed the data, contributed to the discussion, and reviewed and edited the article. J.L. contributed to the discussion, and reviewed and edited the article. U.S., S.S., and T.L. contributed to the design of the study, collected and analyzed the data, contributed to the discussion, and reviewed and edited the article.
Author Disclosure Statement
None of the authors has any conflict of interest.
Funding Information
Financial support was provided by the Department of Research and Development Region Jämtland-Härjedalen, Thuringstiftelsen, Svenska Diabetesstiftelsen, Oskarfonden, Visare Norr, and Kvinnliga Föreningen Gamla Östersund.