
Abstract
Objective:
To assess the impact and feasibility of a telehealth program using continuous glucose monitoring (CGM) and a connected insulin pen cap (CIPC) in nursing homes for older adults with insulin-treated diabetes.
Research Methods:
This multicenter, prospective, sequential, single-arm study consisted of three phases: (1) baseline, blind CGM (Freestyle Libre Pro®); (2) intervention 1, CGM (Freestyle Libre2®) without alarms; and (3) intervention 2, CGM with alarms for hypo and hyperglycemia. Two telehealth visits from reference diabetes units were conducted to adjust antidiabetic treatments. Insulin treatment was tracked using the Insulclock® CIPC. The study’s primary objective was to evaluate the reduction of hypoglycemia rate.
Results:
Of 82 eligible patients at seven nursing homes, 54 completed the study (age: 87.7 ± 7.1, 68–102 years, 56% women, duration of diabetes: 18.7 years, baseline glycated hemoglobin: 6.9% [52 mmol/mol]). The mean number of hypoglycemic events was significantly reduced from baseline (4.4) to intervention 1 (2.8; P = 0.060) and intervention 2 (2.1; P = 0.023). The time below range 70 mg/dL (3.9 mmol/L) significantly decreased from 3.7% at baseline to 1.4% at intervention 2 (P = 0.036). The number of insulin injections significantly decreased from baseline to intervention 1 (1.2 to 0.99; P = 0.027). Nursing home staff expressed a positive view of the program, greater convenience, and potential to reduce hypoglycemia with the Freestyle Libre2® CGM versus the glucometer.
Conclusions:
A telehealth program using CGM and a CIPC was associated with improved glycemic profiles among institutionalized older individuals with diabetes receiving insulin and was well perceived by professionals.
Introduction
The impairment in insulin secretion that causes diabetes mellitus gradually deteriorates as people age. 1,2 The demographic landscape in Western countries is progressively shifting toward an aged population. In 2020, individuals aged 65 years and above comprised 17% of the U.S. population, with 21% being diagnosed with diabetes. 3 Projections indicate that by 2040, this age group is expected to represent 22% of the total population. As the population ages, many individuals reside in specialized facilities, where the prevalence of diabetes ranges from 20% to 34% across various studies. 4 –7
Managing diabetes in older adults is challenging due to the presence of age-related comorbidities and the need for careful treatment deintensification. 8 This population is at high risk of hypoglycemia, which can have devastating consequences, especially for individuals with frailty or cognitive impairment. 9 Furthermore, older adults are particularly vulnerable to adverse events from glucose-lowering therapies, potentially leading to severe outcomes such as cardiovascular events, falls, and increased mortality. 10
Diabetes management in long-term care (LTC) facilities is even more challenging than in hospitals because of the often limited provider and nursing resources and the predominance of older patients with significant comorbidities and compromised functional and cognitive status. 11 These patients are at high risk of hypoglycemia due to various factors, including impaired cognitive and renal function, polypharmacy, and nutritional issues. 12 Guidelines on diabetes management in LTC facilities recommend accounting for patient heterogeneity, prioritizing the minimization of hypoglycemia risk, and using simplified treatment regimens. 13
Continuous glucose monitoring (CGM) may benefit older adults and those in LTC settings since it can detect glycemic excursions, prevent hypoglycemia episodes, and guide therapeutic adjustments. 14,15 Furthermore, integrating these CGM advantages with telemedicine programs can improve glycemic outcomes and reduce patient and administrative burdens. 16 In LTC settings, this approach would allow the automatic sharing of glucose information with health care providers from nursing homes and reference hospitals. However, the feasibility and benefits of CGM in assisting health care providers from nursing homes remain unknown in this challenging population. This is particularly relevant considering that the COVID-19 pandemic has prompted health care systems to adapt their assistance and increase the use of eHealth solutions.
Keeping track of insulin treatment can be challenging, particularly for institutionalized or hospitalized patients. Manual tracking methods are burdensome for nurses and can lead to missed or inaccurate information. Insulclock®, a small, connected insulin pen cap (CIPC) that attaches to all insulin pen devices, addresses this issue by collecting and storing crucial diabetes information, including the date, time, and dose of each injection; type of insulin used; and insulin temperature. These data are accessible via Bluetooth® and smartphone technology, allowing health care providers and caregivers to easily analyze and monitor trends. 17,18 The objective of this study was to assess the impact and feasibility of implementing a telehealth program based on CGM and a CIPC among older adults with insulin-treated diabetes residing in nursing homes.
Research Design and Methods
Design
This multicenter, prospective, sequential, and single-arm study was conducted at seven nursing homes across Spain (Residencias de Ancianos de la Diputación de Burgos, Burgos; Residencia San Fernando, Real Sitio de San Ildefonso; Residencia Nava Asunción, Nava de la Asunción; Residencia Coca, Coca; Residencia Sanchonuño, Sanchonuño; Residencia Claros Abades, Abades; and Residencia San Lorenzo de Segovia, Segovia) and two diabetes units from their corresponding reference hospitals (Endocrinology and Nutrition Unit, Hospital General de Segovia, Segovia; and Endocrinology and Nutrition Service, Hospital Universitario de Burgos). The study was classified by the Spanish Agency for Medicines and Health Products and approved by the Research Ethics Committee (REC) of the Hospital General de Segovia (REC code: 21-036, November 4, 2021). The study was conducted following the ethical principles of the Declaration of Helsinki. All participants provided written informed consent.
The study consisted of a one-week run-in phase followed by a 10-week follow-up divided into three sequential phases: (1) baseline, blind CGM (Freestyle Libre Pro®); (2) intervention 1, CGM (Freestyle Libre2®) without alarms; and (3) intervention 2, CGM with alarms for hypo and hyperglycemia. During the baseline period, participants wore the Freestyle Libre Pro sensor, and during the two intervention phases, they used the Freestyle Libre 2 sensor without and with active alarms, respectively. All participants wore the CGM sensor for 2 weeks during each period, and the time between visits allowed a window of up to 2 weeks to accommodate the center’s availability for visits. Two telehealth visits were scheduled after the Freestyle Libre Pro and the first Freestyle Libre 2 (without alarms). At visit 0 (week 1), participants were screened for eligibility, and demographic and clinical data were collected. At visit 1 (week 0, baseline), inclusion and exclusion criteria were reviewed, and the Freestyle Libre Pro sensor was placed and activated. Nursing home staff (physicians and nurses) were trained in the use of Insulclock device and app. At visit 2 (week 2), Freestyle Libre Pro sensors were collected, after which nursing home staff managed subsequent CGM sensors. The first telehealth consultation (visit 3, weeks 2–4) used data from the Freestyle Libre Pro sensor to adjust antidiabetic treatments. A first Freestyle Libre 2 CGM sensor was applied at the nursing homes with the alarm settings inactive. At visit 4 (weeks 4–5), the second telehealth consultation considered therapy changes after analyzing data from the first Freestyle Libre 2 sensor through the Libreview® platform. At visit 5 (week 6), a new Freestyle Libre 2 sensor was applied at nursing homes with alarms activated to detect hypoglycemia at 70 mg/dL (3.9 mmol/L) and hyperglycemia at 250 mg/dL (13.9 mmol/L). At visit 6 (week 8), CGM and clinical data were collected. The final visit (visit 7, week 10) assessed nursing home staff opinions regarding the feasibility and satisfaction with the devices used and the entire telehealth program using qualitative surveys. The subject’s satisfaction with the diabetes treatment intervention was measured using the Diabetes Treatment Satisfaction Questionnaire change version (DTSQc). 19 Blood glucose monitoring and insulin dosing were based on the standard practice of each nursing home.
Population
Participants aged over 65 years, diagnosed with diabetes mellitus, institutionalized in nursing homes, willing to use the CGM, and who provided written informed consent were included. Exclusion criteria comprised a history or current alcohol or drug abuse within the previous years, an acute infection, or any medical condition that, according to the investigator, could interfere with study procedures.
Outcomes
This study assessed the impact and feasibility of implementing a telehealth program based on CGM and the Insulclock CIPC in nursing homes. The primary objective of the study was to evaluate the effect of the telehealth program on the rate of hypoglycemia. Hypoglycemia was evaluated by collecting the mean number of hypoglycemic events and the proportion of time below range (TBR) at 70 and 54 mg/dL (3.9 mmol/L and 3.0 mmol/L). Hypoglycemic events were defined as glucose levels below 70 mg/dL (3.9 mmol/L) lasting more than 15 min based on 14 days of CGM data.
Secondary objectives were to assess (1) the effect of the telehealth program on glycemic control and (2) the feasibility of implementing the telehealth program. Glycemic control was evaluated by retrieving the following CGM metrics: time in range (TIR) 70–180 mg/dL (3.9–10.0 mmol/L), time above range (TAR) 180 and 250 mg/dL (10.0 and 13.9 mmol/L), glucose management indicator (GMI), coefficient of variation, mean amplitude of glycemic excursions, low blood glucose index (LBGI), and high blood glucose index. 20 Data on glycemic control were also expressed as the proportion of time spent in the different glucose ranges (<54 mg/dL, 54 − 70 mg/dL, 70 − 180 mg/dL, 180 − 250 mg/dL, and >250 mg/dL) and the ambulatory glucose profile (AGP). 21 Data completeness was assessed by the mean duration of CGM use.
The feasibility of implementing a telehealth program in nursing homes was evaluated by collecting nursing home staff’s experiences and satisfaction via two purpose-made questionnaires. The first questionnaire administered to nursing home staff to evaluate satisfaction with the devices used (Insulclock CIPC and Freestyle Libre 2 CGM system) comprised 15 items that could be scored from 0 to 5 (Supplementary Table S1). The second questionnaire, intended to evaluate satisfaction with the entire telehealth program, was also given to nursing home staff. This second questionnaire comprised 10 items, 8 of which could be scored from 0 to 3 or to 4 and 2 of them with Yes/No options (Supplementary Table S2). Additionally, subjects’ satisfaction with the diabetes treatment intervention was measured using the DTSQc. 19
Life expectancy was calculated with the Life Expectancy Estimator for Older Adults with Diabetes (LEAD), a risk-scoring tool based on 11 clinical variables (an interaction between age and heart failure, sex, dementia, metastatic cancer, peripheral vascular disease, body mass index, serum creatinine, albuminuria, home oxygen use, wheelchair use, and current smoking). 22
Devices
The Freestyle Libre 2 (Abbott Diabetes Care) automatically records glucose concentration every 15 min and stores the data in an 8-h log. This CGM system provides continuous access to glucose levels and includes real-time glucose alarms for detecting hypo and hyperglycemia. Glucose data can be uploaded and automatically shared with health care providers within the institution. Additionally, reference diabetologists can access this information using the dedicated software platform (Libreview). Each sensor is valid for 14 days. The FreeStyle Libre Pro is the blinded version for professional use, which automatically records glucose data every 15 min for 14 days and stores the data into the sensor. Glucose data are only available by downloading the memory from the sensor with a specific reader.
Insulclock (Insulcloud S.L.) is a plug-in cap for insulin pens that records the dose and time of insulin injections, tracks insulin temperature changes, detects injection duration, and identifies the specific insulin pen used. 17 For the purposes of the study, we used the Insulclock 360, an application designed for health care providers to monitor multiple institutionalized users. The app synchronizes with devices to automatically log data from insulin treatment and CGM glucose profiles. Each center was provided with a tablet equipped with the app to allow health care providers access to participants’ data.
Telehealth program
Two telehealth visits were conducted by telephone to review glucose data and adjust antidiabetic treatments. The telehealth visit was conducted between the study endocrinologist at the reference unit and the primary care clinician at the nursing home. At each virtual visit, the endocrinologist sent glucose data records and adjustment suggestions (dosing, insulin, and non-insulin treatment changes) to the primary care clinician at the nursing home. Between these visits, the nursing home followed its routine blood glucose monitoring and insulin dosing practices based on the patient's needs and the health care provider’s clinical judgment. The primary care clinician documented in the patient data log any changes performed based on these suggestions.
Statistical analyses
Due to the nature of the study, a formal sample size calculation was not required. In a previous pilot experience at the Trescasas nursing home, around 20% (125 patients) of institutionalized patients were diagnosed with diabetes. Based on this previous experience and, assuming a 30% refusal or unavailability rate, a sample size of 80 patients was estimated.
Statistical analyses were performed using the SAS software (SAS Institute) for Windows, version 9.4. The level of statistical significance was set at p < 0.05. Continuous variables were described by mean, standard deviation, median, and interquartile range (IQR) and categorical variables by numbers and percentages. Comparisons between two independent groups for continuous variables were performed with the Mann–Whitney hypothesis test or the Student’s t-test and with the Chi-square test or Fischer’s exact test for categorical variables.
Additionally, raw CGM data from 14 consecutive days for each study phase were analyzed using the glucodensity function. 23 This analysis provides a detailed understanding of glucose levels by considering the proportion of time spent at each glucose concentration rather than within coarsely defined ranges. The analysis compared the evolution of mean and variability quantiles of individual glucodensities throughout the study phases.
Results
Study population
A total of 82 patients were screened, and we were able to obtain evaluable data for analysis from 54 subjects. The remaining 28 were not analyzed because of clinical or technical reasons or had missing data (Supplementary Fig. S1). Only cases with ≥70% of data during the collection period were included in the final analysis. 24 All patients had type 2 diabetes except for three: two with diabetes secondary to partial pancreatectomy and one with type 1 diabetes. Mean age in the overall population was 87.7 (range, 68 to 102) years and 56% were women. The median (IQR) LEAD risk score was 9 (7−10), corresponding to a median life expectancy of 2.8 years, and 26.5% of the population had a predicted median life expectancy of 2.2 years (score >10). At baseline, mean glycated hemoglobin (HbA1C) was 6.9%. No patient developed diabetic ketoacidosis or severe hypoglycemia during the study. The mean number of days with CGM data was 14.1 at baseline and 14.0 at interventions 1 and 2.
Demographic and clinical characteristics of study participants are shown in Table 1.
Clinical and Demographic Characteristics of Study Participants
Data are expressed as N (%), mean ± standard deviation (SD), or median (IQR).
Patients could have more than one comorbidity.
BMI, body mass index; HbA1C, glycated hemoglobin; IQR, interquartile range; LEAD, Life Expectancy Estimator for Older Adults with Diabetes.
Hypoglycemia
The mean number of hypoglycemic events was significantly reduced from baseline (4.4) to intervention 1 (2.8; P = 0.060) and intervention 2 (2.1; P = 0.023). A nonsignificant decrease in TBR 54 mg/dL (3.0 mmol/L) was observed from 0.3% at baseline to 0.2% at intervention 1 and 0.1% at intervention 2. The TBR 70 mg/dL (3.9 mmol/L) significantly decreased from 3.7% at baseline to 1.4% at intervention 2 (P = 0.036).
Glycemic control
Mean glucose levels increased from 157.6 mg/dL (8.6 mmol/L) at baseline to 160.3 mg/dL (9.0 mmol/L) at intervention 1 and 168.5 mg/dL (9.3 mmol/L) at intervention 2, with no significant differences observed in either phase. The TIR 70 − 180 mg/dL (3.9–10.0 mmol/L) was nonsignificantly reduced from baseline (66.9%) to intervention 1 (66.6%) and intervention 2 (63.0%). No significant differences in TAR 180 mg/dL (10 mmol/L) were observed from baseline (29.4%) to intervention 1 (31.4%) and intervention 2 (35.6%). Similarly, the TAR 250 mg/dL (13.9 mmol/L) increased from 9.2% at baseline to 9.8% at intervention 1 and 11.8% at intervention 2, with no significant differences from baseline to either intervention phase. Glycemic control variables throughout the three study periods are shown in Supplementary Table S3.
When analyzing the percentage of time spent within each glucose range at the study periods, we noted an increase in the time spent above 180 mg/dL, attributed to a decrease in TIR or in time below 70 mg/dL. Notably, the proportion of time within the 54−70 mg/dL range decreased from 3.4% to 1.3%, while an increase from 20.2% to 23.9% was observed in the time spent within the 180−250 mg/dL range. The proportion of time within the target range decreased from 66.9% at baseline to 62.9% at intervention 2 (Fig. 1).
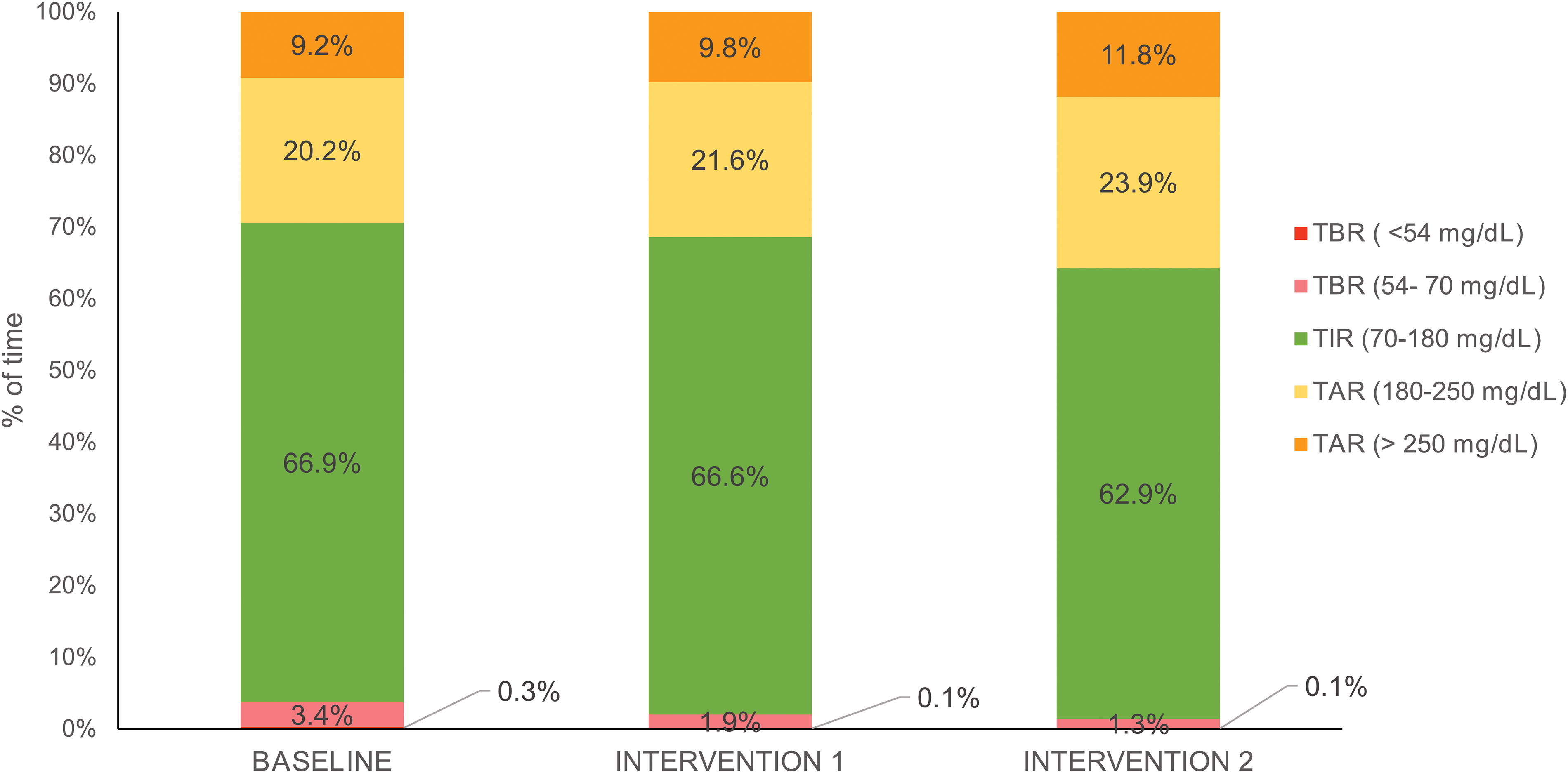
Time within glucose ranges at each study period. The stacked bar graphs show the proportion of time spent at each glucose range (<54 mg/dL, 54−70 mg/dL, 70−180 mg/dL, 180−250 mg/dL, and >250 mg/dL) at each study period. TAR, time above range; TBR, time below range; TIR, time in range.
Figure 2 shows the AGP for the overall study population at baseline and at interventions 1 and 2. At baseline, a pattern of sustained diurnal hyperglycemia with a nocturnal decline was observed, along with a hypoglycemia rate exceeding the recommended limit. Following interventions 1 and 2, the AGP mainly exhibited a flatter nocturnal profile consistent with the observed reduction in hypoglycemia risk.

Ambulatory glucose profile at each study period. The dark line represents the 50th percentile (median), and the lighter outer band represents the 25th to 75th percentile (interquartile range [IQR]) across a 24-h period.
CGM alarms feasibility and impact
Five out of seven nursing homes accepted using alarms at intervention 2. Twenty-five (46%) of the evaluable participants used the alarms. CGM metrics with statistically significant changes from intervention 1 (no alarms) to intervention 2 (alarms) were GMI and LBGI.
Glucodensity analysis
Over the three periods, the glucodensity function confirmed a reduction in hypoglycemia values and a shift toward higher glycemia ranges (Fig. 3). Supplementary Figure S2 illustrates variance quantile function values for glucodensities, highlighting a reduction of glucose variability in the hypoglycemia range, mainly following the first telehealth intervention. Supplementary Figure S3 reveals distinct profiles within the studied population and highlights the impact of the intervention on individual cases.
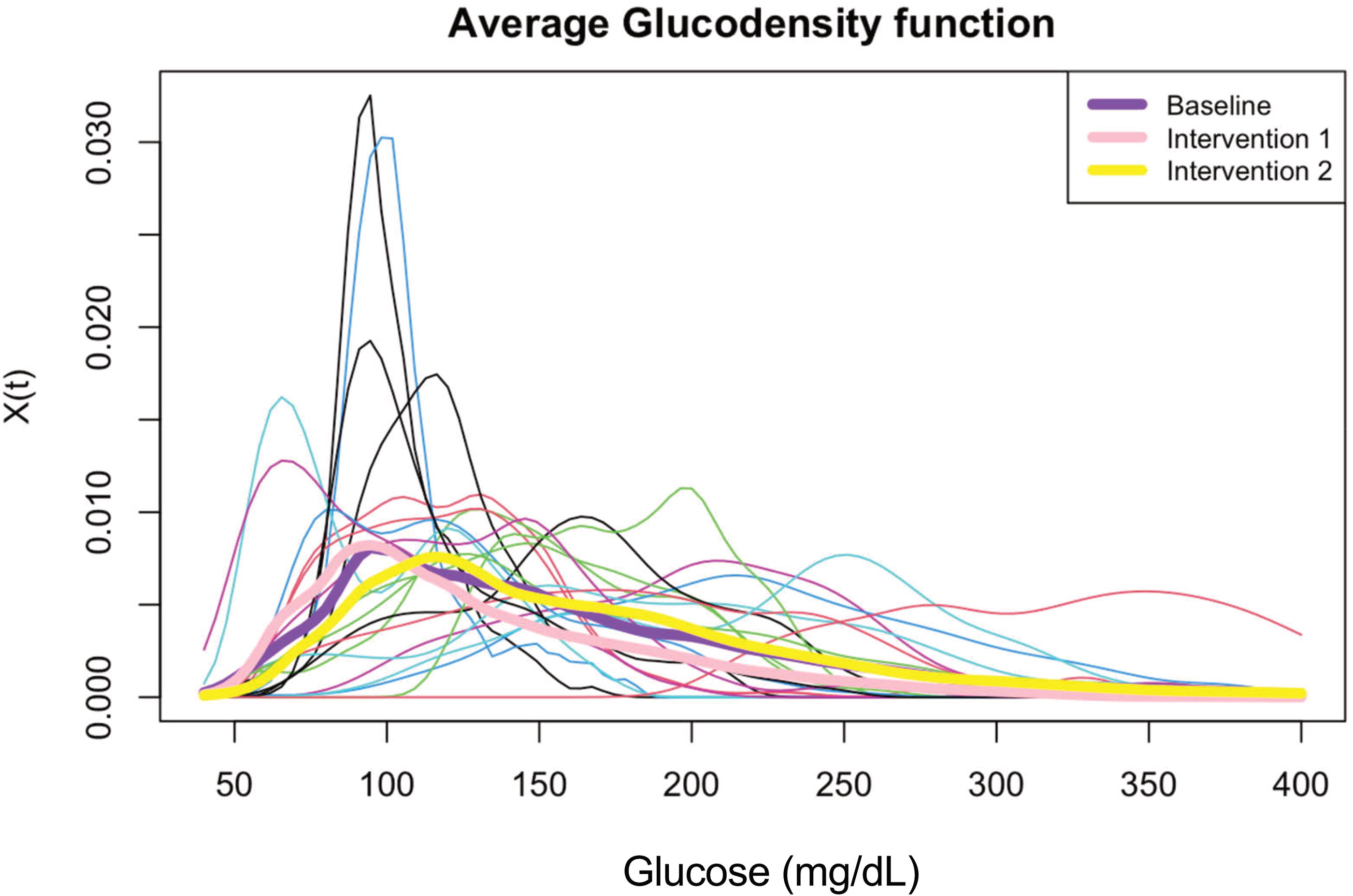
Individual and average glucodensity function at each study period.
Insulin regimen
The median number of insulin injections per day was 1.2 at baseline, 0.99 at intervention 1, and 1.0 at intervention 2, and differences from baseline to intervention 1 were significant (P = 0.027). Rapid insulin injections increased from 1.9 at baseline to 2.8 at intervention 1 and 2.9 at intervention 2. A statistically significant increase in rapid insulin doses was observed from interventions 1 to 2 (increase: 0.4; P = 0.050).
Basal insulin doses (median IU per day) decreased from 15.0 at baseline to 14.0 at intervention 2 (P < 0.01), whereas rapid insulin doses (median IU per day) from 9.8 at baseline to 6.9 at intervention 2 (P = 0.2).
Participants’ experience
The overall experience of the participants with the telehealth program was positive. Based on DTSQ results, participants reported moderate frequency of perceived hyperglycemia (mean: 2.9) and hypoglycemia (mean: 2.0). Satisfaction with how the treatment fitted into their lives (mean: 5.2), knowledge about their diabetes (mean: 4.3), willingness to recommend the treatment (mean: 5.6), and satisfaction with continuing the current treatment (mean: 5.6) showed generally positive ratings.
Nursing home staff experience
In the purpose-made questionnaire to evaluate satisfaction with the devices used (Insulclock CIPC and Freestyle Libre 2 CGM), nursing home staff reported high satisfaction with the CGM device, with a mean score of 3.1 out of 4 (1 = no satisfaction). The items related to the interference of the device with daily professional activity (mean: 3.0; 1 = not bother at all), ease of loading current insulin doses (mean: 2.4; 1 = very easy), and burden associated with insulin treatment management (mean: 2.9; 1 = not bothersome at all) were positively perceived. The device’s comfortability compared to the glucometer received the highest score (mean: 4.5; 1 = not comfortable at all). Regarding the potential reduction of hypoglycemic events, the mean score was 3.7, with 1 representing no reduction. Nursing home staff expressed an overall improvement in the insulin injection technique with the CIPC Insulclock, with a mean score of 3.6 (1 = no improvement). Nursing home staff considered that the combined use of Insulclock and CGM enhanced diabetes patient care, with a score of 3.9 (1 = no improvement).
A total of five health care providers from nursing homes completed the questionnaire to evaluate satisfaction with the entire telehealth program. The telehealth program was rated at 1.2 out of 4, with 1 considered excellent. Health care professionals considered the telehealth program better than traditional consultations, with a mean score of 1 (1 = better). The mean score for comfort with the telehealth program was 1.4 (1 = very comfortable). Health care professionals believed the telehealth program would improve the health of patients with diabetes, with a mean score of 1 (1 = it would improve).
Regarding the technical difficulties with the telehealth program, the mean score was 1.8 (1 = never), indicating infrequent issues. The potential negative impact on work organization was rated at 1.2 (1 = never), suggesting minimal disruption. Health care providers showed a strong willingness to continue with the telehealth program, with a mean score of 1 (1 = yes, without a doubt). The number of contacts through the telehealth program was rated at 2.8 (1 = insufficient).
Conclusions
The available scientific evidence highlights that institutionalized elderly individuals with diabetes are often overtreated. 25 The overtreatment persists even among those individuals with several comorbidities and frequently includes risky treatments such as insulin and sulfonylureas. A longitudinal study involving 21,531 older adults with type 2 diabetes showed that insulin use was most prevalent among older adults with poor health, while healthier patients were more likely to discontinue insulin after age 75 years. 2 Our findings corroborate this concerning trend: a population with an average age of 87 years, treated with insulin and with a life expectancy of less than three years had a baseline HbA1C of 6.9%, indicating a high risk of hypoglycemia. It is imperative that current practice aligns better with guidelines that recommend reducing treatment intensity as health status declines. 13
The described scenario calls for alternative care models to support health care professionals in managing this complex population. In this context, telehealth programs based on diabetes technology are promising for older adults. 16 Our pioneering Trescasas study suggests that these programs are effective in deintensifying treatments and well-received by nursing home professionals. Despite its short duration, our study showed a significant reduction in the doses and number of basal insulin injections (the most frequent insulin treatment in this population), accompanied by a reduction in hypoglycemia risk.
Improving safety and quality of life is the primary objective to achieve among the population of our study. However, the phenomenon of overbasalization, recently described by the American Diabetes Association, 26 is frequently observed in this population. The baseline AGP profile of our sample clearly illustrates this issue. During the telehealth program, we observed improvements in hypoglycemic profiles and CGM metrics within a few weeks, together with a reduction in the basal insulin component and an increase in prandial antidiabetic therapy, particularly the rapid insulin used. This important result warrants discussion. The progressive insulin deficiency associated with age cannot always be managed with long-acting insulin alone. Although many clinical guidelines advocate avoiding or reducing complex insulin regimens in elderly patients, 10 this is not always feasible, and the use of rapid insulin is necessary in some cases. Accurate monitoring using appropriate technology and collaboration with experienced diabetes units can be beneficial in these cases. However, data on postprandial hyperglycemia in our study, mainly the TAR 180 mg/dL, suggests that there is room for improvement in achieving this objective.
CGM has become widespread not only for self-managing diabetes therapy but is also a valuable tool for telehealth. 27 The new CIPCs offer an opportunity to integrate glucose level information with insulin therapy accurately and automatically. 28 To our knowledge, our study is the first to use this technology in institutionalized patients. Importantly, nursing home staff who participated in the study reported that the combined use of these technologies is preferred over traditional methods.
Notably, this study was conducted in Castilla y León, a region exemplifying geographical dispersion due to its extensive rural areas. The need to standardize and validate digital health solutions in such dispersed populations is paramount. Addressing future aging needs within the European Union poses a significant health care challenge, particularly in regions like Castilla y León, where the dispersed demographic adds complexity to providing effective care. 29
Several limitations of the study should be recognized. The number of recruited and evaluated participants was limited. It is important to highlight that the target population has inherent challenges in collaborating with prolonged research studies or those requiring the use of technology, which limited the completion of all study procedures in a significant proportion of the initially eligible individuals. Particularly, cognitive impairment impacted the ability to complete study procedures and follow-up. Likewise, the short duration of the study may have limited the implementation of necessary pharmacological changes to improve prandial control. Furthermore, due to the unavailability of specific surveys, purpose-made questionnaires were administered to evaluate the feasibility and satisfaction with the telehealth program. All the participants were Caucasians. Finally, the study design involved a single arm without a control group. Despite these limitations, the study has notable strengths. It pioneers the use of a novel methodology consisting of a CGM and a CIPC in a challenging target population.
In conclusion, a telehealth program based on CGM and a CIPC is associated with improved glycemic profiles in the challenging population of institutionalized older people with diabetes treated with insulin and is well perceived by nursing home staff.
Footnotes
Acknowledgments
The authors thank the valuable support of Laura García Grande (Residencia San Fernando, Real Sitio de San Ildefonso, Spain), Jessika Olivera Cabrera (Residencia San Fernando, Real Sitio de San Ildefonso, Spain), Virginia Alonso-Díaz (Residencias Nava Asunción-Coca-Sanchonuño, Nava de la Asunción, Spain), and Nadia Caballero-Gómez (Residencias Nava Asunción-Coca-Sanchonuño, Nava de la Asunción, Spain). The authors acknowledge the editorial assistance of Carla Granados from Trialance SCCL. Fernando Gómez-Peralta is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Authors’ Contributions
F.G.-P. designed and supervised the study, researched data, analyzed data, and wrote the manuscript. C.A. researched data, analyzed data, and reviewed the manuscript. M.M. analyzed data and reviewed the manuscript. E.S., A.D.S., A.S.F., L.V.-V., M.G.-G., A.F.-L., C.L.M., B.C., and G.B. researched data and reviewed the manuscript. All authors approved the final version of the manuscript.
Data Availability
The datasets generated during and/or analyzed in the current study are available from the corresponding author upon reasonable request.
Author Disclosure Statement
F.G.-P. has taken part in advisory panels for Insulcloud S.L., Sanofi, and Novo Nordisk; has received research support from Sanofi, Novo Nordisk, Boehringer Ingelheim Pharmaceuticals, and Lilly; and has acted as a speaker for Sanofi, Novo Nordisk, Boehringer Ingelheim Pharmaceuticals, AstraZeneca Pharmaceuticals LP, Bristol-Myers Squibb Co., and Lilly. C.A. has received research support from Sanofi, Novo Nordisk, Boehringer Ingelheim Pharmaceuticals, and Lilly and has acted as a speaker for Sanofi, Novo Nordisk, Boehringer Ingelheim Pharmaceuticals, AstraZeneca Pharmaceuticals LP, and Bristol-Myers Squibb Co. The remaining authors have no conflict of interest to disclose.
Funding Information
The Trescasas study is an investigator-initiated study (code: ADC IIS-20-55) funded by
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.