
Abstract
The global incidence of diabetes is rising steadily and with it the number of people living with diabetic retinal disease (DRD) is increasing. Like diabetes, DRD can be treated but not cured. In response, therapies to address DRD include targeted ocular and systemic medications. This review discusses diabetes and DRD in terms of current screening recommendations, treatments, and considerations related to those therapies and future drug targets and trials on the horizon. This discourse is targeted at all members of the diabetes care team, including primary care providers, optometrists, and ophthalmologists. The dynamic landscape of diabetic retinopathy treatment is promising for the prevention and improvement of visually significant disease.
Introduction
Epidemiology
Diabetes mellitus is now a global pandemic that affects more than 1 in 10 adults worldwide. 1 In the United States, the 2017 estimated type 2 diabetes mellitus (T2DM) prevalence is 13% in those aged 45 to 64 years and about 20% for those aged ≥65 years, not including an estimated 7.3 million people that are undiagnosed. 2 Globally, diabetes is estimated to affect 415 million individuals in 2015 with an annual expenditure of $673 billion and is predicted to affect 642 million individuals by 2040. 3 These statistics are accompanied by a parallel increased incidence of vision-threatening diabetic retinal disease (DRD), affecting about 12% of persons with diabetes worldwide. 4 DRD is the leading cause of vision loss and preventable blindness for individuals aged 20–74 years in developed nations. 5 Vision loss applies to all types of diabetes, as persons with type 1 diabetes (T1DM) are at a higher risk of DRD and most individuals in this cohort will develop some degree of DRD within 15 years of diagnosis, compared with the 12% of diabetic persons experiencing DRD overall. 6 The Wisconsin Epidemiological Study of Diabetic Retinopathy demonstrated that the incidence of visual impairment in patients with T1DM decreased by 57% over 25 years, 7 largely due to better understanding of the disease and better available treatment options. The benefits of these treatment advances apply to patients with T2DM as well.
Pathophysiology of diabetic retinopathy
Diabetes mellitus causes vascular and neurological pathologies, including DRD, diabetic nephropathy, and diabetic autonomic, sensory, and motor neuropathies. 8,9 Together, these pathologies add a substantial comorbidity to diabetic patients and create leading burdens to health care systems. DRD is a progressive disease and presents in stages, affecting the physiology and architecture of the complex neurosensory retina. The retina is organized into 10 layers of cells and is highly metabolically active, relying on diverse mechanisms to facilitate vision across different environments. 10 The photoreceptor component of the retina is composed of rod and cone cells, with the highest concentration in the macula. Therefore, disease in the macula is sight-threatening and is monitored closely by ophthalmical specialists once DRD has been diagnosed. Neurovascular dysregulation in DRD is complex and multifactorial. 11
Visible anatomical changes occur in DRD that correlate to visual impairment and are evident to primary care providers through direct ophthalmoscopy and to eye specialists through dilated indirect ophthalmoscopy and imaging modalities such as optical coherence tomography (OCT). Hallmarks of DRD visible by ophthalmoscopy include cotton wool spots, microaneurysms, hemorrhages, neovascularization, and exudates of lipids and protein that accumulate through leaky vessels. DRD causes blood–retinal barrier breakdown and retinal vessel leakage, so the central retina swells, causing visual impairment from diabetic macular edema (DME). Vision-threatening DME can be objectively measured with OCT, and decisions on interventions can be tailored to the patient. Biochemical pathways associated with excess glucose, the polyol (sorbitol) pathway, nonenzymatic glycation, and oxidative stress have been associated with diabetes complications, but none of these mechanisms has been proven to be causal or modifiable in human disease. 12 –14 A recent summary lists various pathways that are associated with DRD, but none of them has yet fully explained the pathogenesis of DRD. 15
Screening recommendations
The leading cause of visual impairment in persons with DRD is DME. 16 It is best detected by trained eye specialists with a dilated fundus examination, yet despite this understanding, only 30%–40% of patients in the United States receive an advanced eye examination in the first 5 years after diagnosis. 17 Multiple studies have highlighted that 50%–75% of patients with diabetic retinopathy (DR) and/or DME are unaware that they have diabetic eye disease. 18,19 Screening for DRD remains a challenge for both physicians and patients. Cited barriers to screening include patients having no vision symptoms, misunderstanding regarding screening for well-controlled disease, and a lack of formal recommendation for a dilated examination by primary providers. 20
The American Diabetes Association (ADA) recommends dilated eye examinations by an ophthalmologist or optometrist within 5 years of T1DM diagnosis or at the time of T2DM diagnosis. 21 If there is no evidence of retinopathy and glycemic measures are within the target range, then patients may continue screening examinations every 1 or 2 years. When patients are identified with any evidence of DR, including DME, the American Academy of Ophthalmology and American Society of Retina Specialists recommend referral to an ophthalmologist experienced in treating DRD. 22 Engagement of patients and physicians to awareness of the current diabetic screening recommendations is paramount to early identification of retinopathy. 19 Treatment improves ocular and systemic disease control, as well as educational and emotional support from the primary team.
Classification of DR
The Diabetic Retinopathy Study (DRS) provided the basis for the DR classification system known as the Early Treatment of Diabetic Retinopathy Study (ETDRS) criteria (Fig. 1). 24 In this classification system, 7 photographs per eye were used to identify DR lesions and give a severity score. 24 The ETDRS DR severity scale describes 12 DR levels based on characteristics observed in color fundus photographs. Assignment of a patient’s DR severity and clinically significant macular edema determines subsequent examination frequency, need for subspecialist referral, and treatments. Therapeutics are targeted at changing the clinical course for patients with moderately severe/severe nonproliferative DR (NPDR) before it progresses to proliferative disease.

Schematic of Diabetic Retinopathy Severity Scale (DRSS) from ETDRS = Early Treatment of Diabetic Retinopathy Study; NPDR = nonproliferative diabetic retinopathy; PDR = proliferative diabetic retinopathy; PRP = panretinal photocoagulation. Source: Arcadu et al. 23 Courtesy of Creative Commons Open Access License.
Proliferative DR (PDR) exists when retinal and/or iris neovascularization develops with the risk of vitreous hemorrhage, fibrovascular tissue proliferation, and retinal detachment. Severe NPDR is defined as the state without signs of neovascularization but has the following: (1) severe intraretinal hemorrhages and microaneurysms throughout the retina, (2) venous beading in ≥2 quadrants, or (3) moderate intraretinal microvascular abnormalities in ≥1 quadrant. 22 DME can occur at any stage of DR, but is more common in those eyes with greater DR severity. 25 To simplify, DR is classically categorized into either NPDR or PDR, with or without DME. ETDRS-guided conventional management has been to essentially observe NPDR without DME and to treat DME and PDR. 26
Recently, artificial intelligence (AI) has offered efficiency in diagnosing and treating DR. In 2018, the software program Idx-DR received FDA approval for analysis of retinal images taken with a nonmydriatic retinal camera for DR screening (FDA.gov). Since then, many AI software programs using deep learning algorithms have emerged, including EyeArt, Retmarker, Google, and the Singapore Eye Lesion Analyser. 27
In this dynamic environment of advancements in screening techniques, DR identification follows an explosion of systemic and ocular pharmacotherapy and surgical treatment options. We divide the discussion into ocular pharmacologic and surgical therapies and systemic approaches. This review covers the current and prospective management options that are rapidly changing in the landscape of caring for patients with vision-threatening DRD. The 50-year-old classification of DR is not quantitative and does not account for responses to laser therapy or drug therapy. These limitations have resulted in calls for a revised classification scheme that accounts for visual function and the status of the neurosensory retina. 28,29 This work is a major focus of the Mary Tyler Moore Vision Initiative (marytylermoore.org).
Ocular Treatments of DR
Ocular pharmacologic treatments of DR
Antagonism of vascular endothelial growth factor (VEGF) action has become the mainstay of the ocular management of DRD. VEGF induces endothelial cell leakage and proliferation, and its upregulation is key to the progression of DR through proliferation of new vessels and promotion of vascular permeability. 30,31 As DRD progresses, areas of ischemia, inflammation, and metabolic mismatch promote neovascularization mediated through upregulation of VEGF, and neovascularization and vascular leakage ensue. 32 Thus, targeted intraocular VEGF inhibition has become a major advancement for treatment of DR. 33
The ETDRS is the basis for observing mild-to-moderate NPDR without DME, as well as severe NPDR. 24 This study was published 2 years before the Diabetes Control and Complications Trial that established the importance of intensive metabolic control. 34 However, the treatment algorithms for vision-threatening PDR and/or DME have become more straightforward as data from studies became more robust. The pathogenesis of PDR and DME is complex and multifactorial. Treatment options for DR can be divided into those addressing PDR and those addressing DME. PDR is associated with retinal ischemia and a pro-angiogenic environment, of which VEGF is a major player. 35 DME is thought to be secondary to accumulation of intraretinal fluid from disruption of the blood–retinal barrier secondary to factors affected by hypoxia, VEGF, protein kinase C activation, and histamine. 36 In 1994, elevated VEGF levels in the ocular fluid of DR patients led to the initial Food and Drug Administration (FDA) approval of the anti-VEGF drug, pegaptanib, for treating neovascular age-related macular degeneration. 37 This step was quickly followed by the development and use of other anti-VEGF agents, notably bevacizumab, ranibizumab, and aflibercept, to treat DME 38 and PDR. 33,39
Before the development of pharmacotherapy options such as anti-VEGF agents and corticosteroids, retinal laser photocoagulation was the mainstay of care for DME patients. 40 The ETDRS showed that focal laser treatment reduced the rate of moderate vision loss by at least 50% in eyes with clinically significant DME compared with no treatment. 24 Traditional focal laser photocoagulation was not ideal for treatment in the macula because it created small laser burns and their enlargement over time. 41 These concerns led to the development of the “subthreshold lasers” where photocoagulation is achieved with shorter pulses using a low power to minimize collateral thermal damage. However, few clinicians have adopted subthreshold laser treatment of the macula.
Corticosteroids reduce intraocular VEGF so intravitreally injected triamcinolone for the treatment of DME was a focus of study in the Diabetic Retinopathy Clinical Research Network. 42 It was found to be less effective than laser photocoagulation for DME as a primary therapy, but beneficial for those eyes that are refractory to laser treatment. 42 Sustained-release dexamethasone and fluocinolone acetonide intraocular implants for persistent DME have been developed, 43 but they are generally used as secondary agents because they can cause cataracts and glaucoma. 44
The focus of DME treatment until recently has been focused on inhibition of VEGF-A through FDA-approved and off-label use of intravitreal injections of ranibizumab, aflibercept, and bevacizumab. 45 Comparison of the three first-generation intravitreal anti-VEGF drugs showed aflibercept to be more effective at improving vision in eyes presenting with worse initial visual acuity. 46 The visual outcomes for the three agents were similar for eyes with good (20/40 or better) baseline visual acuity.
Bevacizumab is a full-size, humanized, recombinant monoclonal immunoglobulin G antibody that binds all VEGF isoforms. Its use as an intravitreal anti-VEGF agent is considered off-label, as its FDA approval is for the systemic treatment of metastatic colorectal cancer. However, its use in treating DME is widely accepted due to its low cost, safety, and positive clinical effects in case studies and retrospective studies. 47 Ranibizumab is a humanized monoclonal antibody fragment that targets VEGF-A. The FDA approval of intravitreal ranibizumab for treatment of DME in 2012 was supported by the RISE and RIDE studies. 48 Patients improved in visual acuity by 11.7 and 12.0 letters (2 lines on the ETDRS chart) in the ranibizumab 0.3 and 0.5 mg groups, respectively, at 2 years, equivalent to 2.5 letters in the sham group. Aflibercept consists of two VEGF receptors fused to a humanized monoclonal antibody backbone that targets VEGF-A, VEGF-B, and placental growth factor. It was FDA approved for an intravitreal treatment of DME in 2015 in its original 2 mg dose. Two important trials (VIVID and VISTA) compared 2 mg aflibercept every 4 weeks and every 8 weeks after loading with macular laser photocoagulation. Visual outcomes were greater with aflibercept 2 mg than with laser treatment. 49
The randomized trials associated with these first-generation anti-VEGF drugs (bevacizumab, ranibizumab, and aflibercept) showed significantly improved vision after 1 year, 50,51 but real-life use did not match the visual outcomes achieved in clinical trials. It was apparent that achieving maximum benefits of intravitreal anti-VEGF therapy required adherence to an aggressive treatment schedule, and reduced anti-VEGF treatment showed diminishing long-term visual acuity benefits. 52 This information birthed the next generation of anti-VEGF agents designed for greater treatment durability. Brolucizumab is a single-chain antibody fragment that targets all three VEGF-A isoforms (110, 121, and 165 kDa) that received FDA approval in 2022 for intravitreal treatment of DME. Its use has been limited by concerns for a 3% intraocular inflammation rate, including vasculitis in the pivotal clinical trials compared with the 1% in the control aflibercept group (brolucizumab package insert 2022). Real-world studies report an incidence of intraocular inflammation after use of the drug ranging from 0% to 19%. 53 Faricimab is a bispecific antibody targeting both VEGF-A and angiopoietin-2 that received FDA approval in 2022 as an intravitreal injection for DME. Dual inhibition of angiopoietin-2 (Ang-2) and VEGF-A is intended to provide a synergistic effect to enhance vascular stability and reduce vascular leakage. 54 FDA approval for treatment of DME was supported by YOSEMITE and RHINE trials, in which patients were randomized to receive one of two 6 mg faricimab regimens (fixed 8-week dosing or treat-and-extend protocol) or standard fixed-dose 2 mg aflibercept. Faricimab was well-tolerated with a similar safety profile to aflibercept and found to be noninferior to 2 mg aflibercept. 55
Aflibercept 8 mg received FDA approval in 2023 as the first and only treatment approved for DME for dosing at 8-week intervals and up to 16-week intervals after 3 initial monthly doses. The PHOTON trial randomly assigned patients with DME to standard 2 mg aflibercept or to 8 mg every 12 or 16 weeks after loading. The trial showed noninferiority with the higher 8 mg dose and extended treatment schedule and with maintenance of visual acuity improvements and a similar safety profile compared with the 2 mg dose. 56 Thus, patients require less frequent treatment than with the 2 mg dose.
Since 2022, many biosimilars have entered the competition for intravitreal treatment options. Two ranibizumab biosimilars, ranibizumab-eqrn and ranibizumab-nuna, have received FDA approval and interchangeable status in 2022 and 2023, respectively, allowing for lower cost delivery of an agent without clinically meaningful difference in safety and effectiveness compared with ranibizumab. 57 Other biosimilars for aflibercept are in development.
In addition to its use for treatment of DME, anti-VEGF agents are a frequent treatment for PDR, as it significantly reduces the area of leakage and improves visual acuity. 58 Intravitreal ranibizumab 0.5 mg is noninferior to panretinal photocoagulation (PRP) for PDR. 59 Aflibercept was also noninferior to PRP in the CLARIFY trial and showed greater improvement in retinopathy compared with PRP. 60 Intravitreal anti-VEGF therapy is especially useful in cases of PDR complicated by vitreous hemorrhage that obscures the patient’s view and limits the ability to apply PRP. 33 These anti-VEGF effects seem advantageous, but the long-term results and duration of adherence to anti-VEGF in eyes with NPDR are not yet defined. 61 The improvement of vascular lesions in treated eyes 62 does not improve vascular reperfusion as determined by fluorescein angiography 63 nor visual acuity benefit with early intravitreal aflibercept for moderately severe or severe NPDR. 64 In fact, after 2 years of ranibizumab therapy, eyes with PDR developed peripheral visual field loss at nearly the same rate as eyes treated with PRP. 59,65 It is also not clear whether improvement in Diabetic Retinopathy Severity Scale (DRSS) is a true disease modification. 61 Ocular therapy for NPDR without DME is still being refined 61 ; the treatment of DRD still relies on concurrent systemic control of diabetes.
Surgical/procedural ocular treatments of DR
The DRS established in 1978 shows that there is significant reduction in severe vision loss due to PDR treated with PRP compared with untreated controls. 26 Retinal laser treatment produces photothermal effects with coagulative necrosis through absorption of the light in the retinal pigment epithelium and the choroid. 66 The mitigation of vision loss from retinal ischemia and proliferative disease is not without cost, because PRP causes discomfort during the laser treatment, permanent decreases in night, peripheral, and color vision, and occasional exacerbation of DME. 67 However, PRP remains a standard of care for treatment of PDR when indicated. 22
Surgical management for DR is focused on advanced disease stages. Vitreous hemorrhage is the most common complication of PDR that decreases visual acuity. 68 Nonclearing vitreous hemorrhages are generally removed by vitrectomy after 1–6 months for T1DM patients, but can be observed for longer in T2DM patients, depending on the presence of adequate PRP treatment and patients’ impairment. Other indications for pars plana vitrectomy include severe fibrovascular proliferation, macular-threatening tractional retinal detachment, ghost-cell glaucoma, premacular hemorrhages, and macular edema with tractional components. Updated vitrectomy instrumentation such as high cutting rates and 25- or 27-gauge instruments allow for precise removal of fibrovascular membranes and the repair of tractional retinal detachments. 69 New imaging technologies such as intraoperative OCT afford live cross-sectional microarchitectural views of the macula to identify tissue planes and assist with membrane peeling maneuvers. 70
Other devices and procedures are aimed at improving efficiency in the delivery of pharmacologic agents. Surgical implantation of long-term medication devices is aimed at decreasing the treatment burden of monthly intravitreal injections. A port delivery system (PDS) for ranibizumab continuously delivers anti-VEGF into the vitreous after surgical implantation with in-office refills. The PAGODA trial compared 634 patients with center-involving DME who were randomized to PDS group or intravitreal ranibizumab 0.5 mg monthly injections after receiving loading doses. 71 The trial showed PDS to be noninferior to monthly ranibizumab injections. The sponsor issued a voluntary recall in 2022 for septum dislodgement issues (Genentech voluntary recall 2022). The PAVILION trial, in which patients with moderately severe to severe NPDR without center involving DME were assigned to PDS or standard of care, showed stable visual acuity through 1 year. 71
Systemic Treatments of DR
Systemic pharmacologic treatments of DR
In patients with T1DM, control of systemic blood pressure can have a profound impact on DR. 72 Conversely, the ACCORD trial in T2DM patients demonstrated that intensive blood pressure regulation did not significantly impact DR progression, whereas intensive control of glycemia and cholesterol levels did, thus highlighting differences in the type of diabetes in DR and the impacts of systemic medications on the disease. 72,73 Hence, physicians and ophthalmologists must work together to help prevent visual impairment and blindness in persons with diabetes.
In 2024, ADA focused its recommendations on implementing strategies to help persons with diabetes achieve glycemic, blood pressure, and lipid goals to reduce the risk for or slow the progression of DR. 21 Glycemic and blood pressure control are well-defined modifiable risk factors for DR. 74 Every 1% decrease in glycated hemoglobin level is associated with a 40% reduced risk of DR, and every 10 mm Hg decrease in systolic blood pressure is associated with a 35% reduced risk. 74 Meta-analysis of renin–angiotensin system inhibitors showed that angiotensin converting enzyme (ACE) and angiotensin receptor blocker (ARB) inhibitors reduce the risk of DRD and may exert the most beneficial effect on DR of all the widely used antihypertensive drug classes. 75 Although these benefits are well-established and common knowledge among patients and clinicians alike, multiple studies show that only 20%–30% of diabetic patients are able to meet glycemic and blood pressure targets. 18 There are distinct beneficial effects of reducing blood pressure to prevent DR, 74 but a 2023 Cochrane Review concluded that there was a paucity of evidence to support reduction of blood pressure to prevent DR. 76 However, hypertension is a well-known modifiable risk factor to reduce DR progression, as well as cardiovascular and renal disease. 77
Dyslipidemia is a risk factor for DR progression, and treatment with statins has been associated with reduced vision loss. 78 Fenofibrate inhibits DR progression, but its effects may be less related to lipid production than from its anti-inflammatory and antioxidant properties. 78 Two large clinical trial subgroup analyses suggest that systemic fenofibrate reduces DR progression. 79 The FIELD trial first demonstrated that fenofibrate inhibition of peroxisome proliferator-activated receptor (PPAR)-α used to treat the metabolic effects of cholesterol metabolism in diabetic patients had a significant impact on the progression of DR. 80 The exact mechanism by which PPAR-α inhibition slows DR is not known, but there is evidence of PPAR-α downregulation in animal models of DR and that activation through systemic drugs and through local microRNA modulation is protective. 81,82
A multicenter cohort study showed fenofibrates to be associated with a decreased risk of visually threatening DR and PDR. 77 Nevertheless, fenofibrate is rarely prescribed for DRD in the United States, so the DRCR Retina Network is enrolling patients who are randomly assigned to once daily fenofibrate or placebo with a primary outcome of worsening DR at 4 years, estimated to be completed in mid 2027.
Mainstays of systemic pharmacologic treatment of diabetes include insulin, metformin, thiazolidinediones (TZDs), and sulfonylurea (SU) derivatives. Metformin decreases progression of DR, 83 at least partly through inhibition of angiogenesis and retinal inflammation. 84 TZDs are agonists of PPARγ that are found in multiple cells. The ACCORD-Eye study concluded that TZDs improved visual acuity and were not associated with an increased risk of DME. 85 SU derivatives, such as gliclazide, glipizide, glibenclamide, and glimepiride, are still used due to their low cost. The SU derivatives act through sulfonylurea receptor 1 (SUR1) and sulfonylurea receptor 2 (SUR2) receptors on beta cells and other tissues, including the retina, regulating the flow of K+ ions, and secondarily Ca++ ions, through ATP-dependent channels. 86 Retrospective analysis of the groups of antihyperglycemic drugs did not show significant correlations with DR, 87 although persons treated with SU derivatives had a statistically higher risk of DR compared with placebo. 86
Newer antihyperglycemic drugs have entered the therapeutic armamentarium. Dipeptidyl peptidase-4 inhibitors, including sitagliptin, saxagliptin, and linagliptin, have shown an overall acceptable safety profile in use with patients with DR, although results are mixed regarding risk of ocular events. 86 Sodium-dependent glucose transporter (SGLT) inhibitors have become standard of care, in addition to glucagon-like peptide-1 (GLP-1), in treating diabetic patients with cardiovascular disease. 88 SGLTs and facilitative glucose transporters regulate cellular uptake of glucose molecules, including in the retina. 89 The flozin class of SGLT-2 inhibitors reduces sodium-dependent glucose uptake and removes excess glucose from the microcirculation by acting on renal tubules. Post hoc analysis of the EMPA-REG OUTCOME study showed that taking empagliflozin was not associated with an increased risk of DR compared with placebo. 90 A meta-analysis including over 100,000 T2DM patients has supported flozins to be the safest form of therapy in terms of risk of DR development. 87
There was recent interest in the possible association between the use of GLP-1 analog, semaglutide, and DRD. 91 Semaglutide received FDA approval for a long-term weight management therapy and to improve glycemic control for patients with T2DM. The SUSTAIN 6 trial noted significantly increased development of DR in semaglutide users compared with placebo. 91 However, meta-analysis of randomized controlled trials failed to find a causative association between semaglutide and increased DR risk. 92 Patients ≥60 years or who had diabetes for ≥10 years were at increased risk for DR, which was thought to be related more from the magnitude and speed of glucose reduction rather than from semaglutide per se. The unclear role of GLP-1 inhibitors on DR progression spawned the FOCUS clinical trial discussed below. Comparison of systemic diabetic medications in retrospective observational database study demonstrates that of all glucose lowering medications discussed, the SGLT inhibitors were associated with the lowest risk of sight-threatening DR (Fig. 2). 93
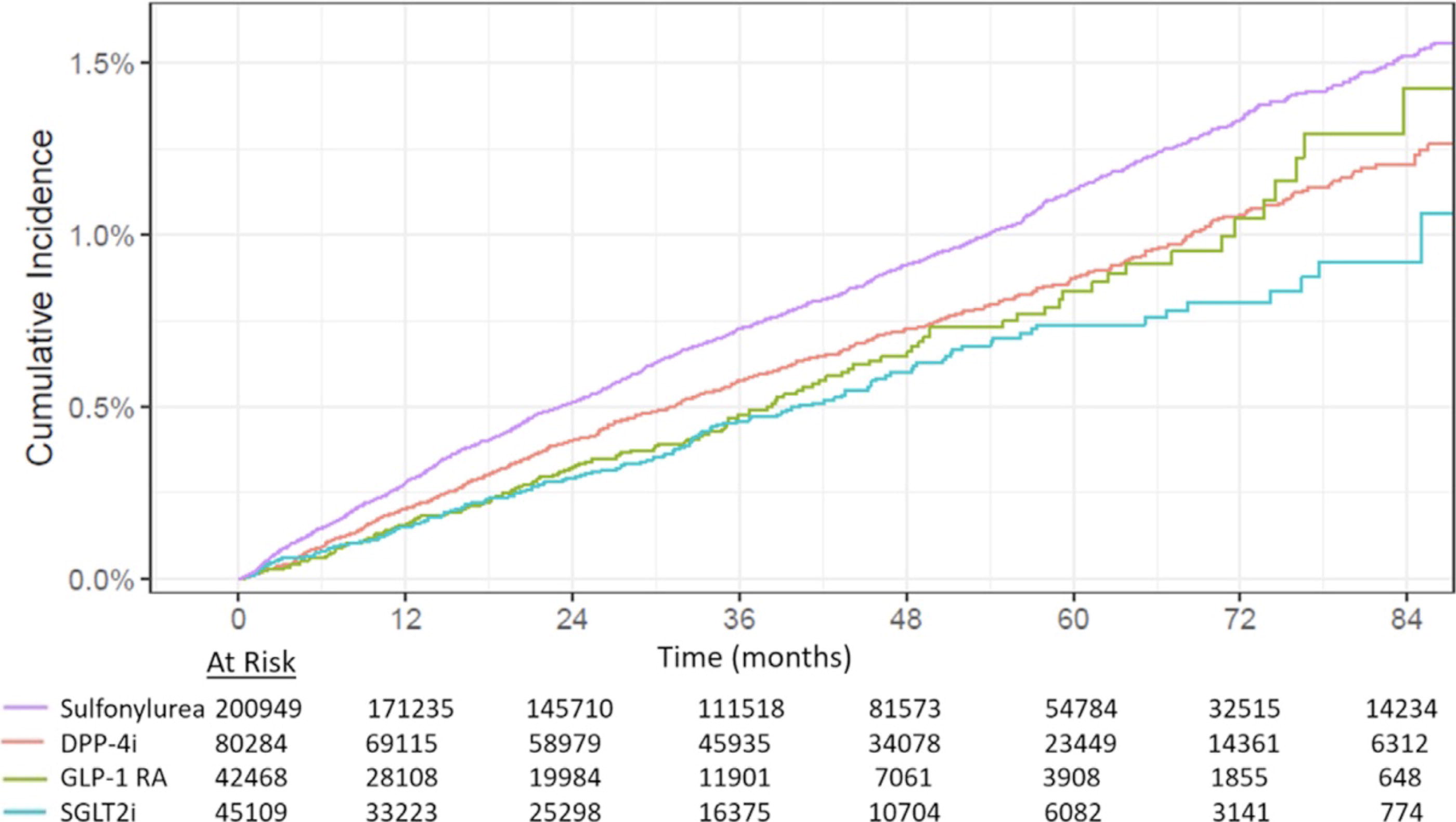
Incidence of treatment for diabetic retinopathy with systemic diabetic medications from Barkmeier et al., 2024. 93
Surgical/procedural systemic treatments of DR
Pancreatic islet transplantation is a definitive surgical approach for treatment of T1DM. One study showed that 18.8% of patients had progression of DR within 12 months, and 20.5% after 4.2 years, 94 so careful fundus monitoring in the perioperative period and the years following surgery is important. 94
Bariatric (metabolic) surgery includes gastric banding, sleeve gastrectomy, and Roux-en-Y gastric bypass techniques. Rapid correction of blood glucose levels and postoperative postprandial hypoglycemia in diabetic patients may contribute to worsening DR, 95 although the exact mechanisms are still not clear. One study showed that 19% of bariatric surgery patients developed new DR and concluded that DR progression was highest in young men with preoperative DR and poor metabolic control and that bariatric surgery does not prevent DR. 96 Another study indicated that bariatric surgery can improve diabetic peripheral neuropathy and DR. 97
Noninvasive treatments with lifestyle changes also remain a fundamental element in treating diabetes. Post hoc analysis of the DCCT study showed a significantly higher risk of DR progression with a high-calorie diet rich in fatty acids and smoking. 98 Meta-analysis of 22 studies showed association with regular physical activity and a statistically significant lower risk of occurrence and progression of DR. 99 Obstructive sleep apnea is very common in T2DM 100 and is associated with sight-threatening DR and an independent predictor for the progression to pre-proliferative DR and PDR. 101 Several clinical trials have examined the relationship of obstructive sleep apnea (OSA) with DR, and use of continuous positive airway pressure (CPAP) reduces the progression of DR. 102
Emerging Treatments for DRD
Trials in ocular therapy for DR
Multiple ongoing trials utilize different techniques to modulate the VEGF pathway or target different mechanisms of action and pathways altogether. Several ongoing studies involve gene therapy, including intraocular injection of a drug, 4D-150 (Table 1). A transgene expresses aflibercept and a VEGF-C inhibitory ribonucleic acid interference (RNAi), which incorporate into recipient cell DNA and express the desired proteins. Such technology has a favorable safety profile in Phase 1 trials in persons with age-related macular degeneration. This strategy could potentially reduce the number of intraocular injections needed to prevent disease progression by forcing one’s own cells to produce a desired therapy protein. 103 The trial for 4D-150 is recruiting participants in phase 2 studies, and data from a trial of anti-VEGF gene therapy using 4D-150 to treat macular degeneration have interim results up to 48 weeks follow-up demonstrating an 89% reduction in the annualized anti-VEGF injection rate. Other approaches include combining anti-VEGF medications with novel drug targets. For example, intravitreal injections of the biological RC28-E use a chimeric decoy receptor trap fusion protein to block both VEGF and fibroblast growth factor (FGF) 2, the latter of which is proangiogenic and may contribute to the development of resistance to anti-VEGF medications. Phase 2 testing is ongoing with evaluation to 48 weeks of treatment. 103,104
Mechanisms of Trials in Ocular Treatment of Diabetic Retinopathy
VEGF, vascular endothelial growth factor; ETDRS, Early Treatment of Diabetic Retinopathy Study.
Beyond VEGF antagonism, another emerging approach is the utilization of corticosteroid preparations that target inflammatory pathways of DR. OCS-1 is a high-concentration dexamethasone topical ophthalmical suspension designed to penetrate the anterior and posterior segments. 105 The DIAMOND trial is a phase 3 double-masked, randomized multicenter study in which 148 patients were randomized to receive OCS-01 or vehicle 6×/day. The study met its primary end point of significant improvement in visual acuity, in retinal thickness, and was well-tolerated in 52 weeks of study. Increased intraocular pressure occurred in 14% of OCS-01-treated eyes, but no evidence of cataract formation. 103
Other pathways are emerging as targets for DR, including the Bcl-xL senolytic pathway. Cellular senescence is characterized by increased expression of the antiapoptotic protein, Bcl-xL, 106 and inhibition of Bcl-xL with UBX1325 is thought to remove senescent cells, leading to enhanced retinal function via improved blood–retinal barrier function and reduction of inflammatory factors. 107 The BEHOLD 2a proof-of-concept trial enrolled 65 DME patients randomized to intravitreal injections of UBX1325 or sham. Results presented as a meeting abstract 107 revealed that clinically significant improvement in best-corrected visual acuity (BCVA) was met at 24 weeks; treatment was well-tolerated without significant treatment-related adverse events.
The kallikrein–kinin system was identified as a VEGF-independent DME mediator nearly 10 years ago with an 11-fold increase in vitreous plasma kallikrein levels in DME patients. 108 A potent inhibitor of plasma kallikrein, THR-149, was shown in phase 1 and 1 b studies to be safe and well-tolerated as an intravitreal injection and demonstrated improvement in visual acuity from baseline. 109 The phase 2 KALAHARI study with 20 enrolled DME patients with prior suboptimal anti-VEGF response 110 found treatments to be safe and well-tolerated without need for rescue medications at month 3, although was stopped due to inefficacy in 2023. A phase 3 study of RZ402 (Rezolute, Inc; NCT05712720) is now in progress.
Alternative intraocular medications to target interleukin-6 signaling, semaphorin-3A, endothelin receptor, and others are being studied to uncover new ways of preventing the damaging progression of neovascularization and inflammation in DR.
Dr. Stephen Kim at Vanderbilt University is evaluating the role of prostaglandin E2 and other inflammatory cytokines in persons with NPDR via measurement of aqueous humor PGE2 concentrations with or without topical ketorolac therapy (NCT0450556).
Boehringer Ingelheim tested the effects of an antibody against semaphorin-3A, an axonal guidance protein, in a phase 1/2 trial in patients with diabetic macular ischemia (as opposed to edema). In macular edema, the retina is thicker than normal, whereas in these eyes the macula is thinner than normal, and the blood vessels are not perfused with fluorescein dye or appear nonperfused by OCT angiography. 111 No treatment has been proven effective for this condition, in large part because it is poorly understood and represents a late stage of DRD. The trial did not show benefits after intravitreal injections at 12–40-week follow-up (NCT04424290).
Trials in systemic therapy for DR
Many clinical trials aim to control systemic diabetes and metabolic syndrome, and several of them may contribute to limiting DRD. Systemic efforts to minimize VEGF dysregulation in complex diabetes are under investigation. Through an indirect mechanism, inhibition of a transcription factor (REF-1) reduces VEGF expression. 112 The experimental APX3330 redox factor-1 inhibitor is an orally administered inhibitor of transcription factor regulator redox factor-1 associated with inflammation and VEGF production (Table 2). 113 However, the phase 2 ZETA-1 trial failed its primary efficacy end point of DR severity improvement at 24 weeks (NCT04692688), but fewer APX3330-treated patients had retinopathy worsening compared with placebo. In diabetic mice, oral administration of CU06-1004 reduced vascular leakage by maintaining endothelial cell junctions and through nuclear factor-κB inhibition reduced Intercellular adhesion molecule 1 (ICAM-1) and vascular cell adhesion molecule 1 (VCAM-1), opposing the effects of VEGF. 114 Safety trials of oral CU06-1004 have been completed, and study results are pending (Table 2).
Mechanisms of Trials in Systemic Treatment of Diabetic Retinopathy
NFκB, nuclear factor-κB; GLP-1, glucagon-like peptide-1; PPAR, peroxisome proliferator-activated receptor.
While not currently a mainstay of treatment of DR, the results of fenofibrate therapy from the ACCORD trial and other studies hold promise for systemic level of disease management. 73 Large-scale trials are investigating the clinical utility of fenofibrates. The LENS trial is a streamlined randomized double-masked phase 4 placebo-controlled trial based in Scotland that investigated fenofibrate in early DR disease management over 4 years. 115 A total of 1151 participants with nonreferable DR or maculopathy were included, and the study has recently completed with results demonstrating a 27% lower risk of diabetic eye disease compared with placebo and lower DME rates in the treatment group. 116 Phase 3 trials of fenofibrate in both T1DM and T2DM are underway in the United States (NCT04661358) with a 4-year follow-up and in persons with T1DM in Australia with a 1-year follow-up (NCT01320345).
Clinical trials in the systemic treatment of DR include novel considerations of medications already in use for other indications. Because of the expanding use of semaglutides in the treatment of T2DM and the conflicting data presented on the impact of these medications on DR, direct trials have been established to assess the impact of GLP-1 receptor inhibitors on DR. The ongoing FOCUS trial (NCT03811561) is examining the long-term effects of semaglutide on DR in 1500 patients over 5 years and is predicted to be completed in 2027. The CANBERRA trial (NCT04265261) investigated the impact of oral RG7774, a synthetic agonist of the cannabinoid receptor 2, on DR severity from baseline over 36 months. Animal models of DR demonstrated improved retinal vascular permeability, leukocyte adhesion, and ocular inflammation with RG7774 oral administration, 117 and clinical trial results showed some promise, but the manufacturer decided to abandon the drug. Other pathways being investigated include Rho-associated, coiled-coil-containing protein kinase (Rho kinase) inhibitors, connexin channel inhibitors, and dopamine pathway modulators that hold great potential for the systemic management of DR.
Conclusions
Diabetes holds the status of a global pandemic with increasing prevalence. Advances in treatments for diabetes and retinopathy provide a promising outlook for mitigating sight-threatening effects. Early identification of DR through frequent dilated retinal examinations as per guidelines is essential for prompt referral to the ophthalmologist and retinal specialist. Systemic management is equally essential for the management of NPDR and for the prevention of progression to DME and PDR with the primary care physician playing a pivotal role in the fight against vision loss in diabetic patients. Treatment advances have demonstrated powerful improvements in the care of DR, whereas trials in novel mechanisms and progress in standards of care hold promise for the future. Awareness of current guidelines, treatment protocols, and new therapeutics by both generalists and specialists is essential for preserving sight in the diabetic population.
Authors’ Contributions
Author R.B., wrote manuscript, D.B., assisted with manuscript writing, T.G., conceived manuscript and edited.
Author Disclosure Statement
The authors have no conflict of interest to declare.
Footnotes
Funding Information
Supported by the Mary Tyler Moore Vision Initiative, Breakthrough T1D, and the Taubman Medical Research Institute (TWG).