
Abstract
Introduction:
Continuous glucose monitoring (CGM) use in people with type 1 diabetes (T1D) is revolutionizing management. Use of CGM in hospital is poised to transform care, however routine use is not currently recommended due to lack of accuracy validation in acute care, including in people with T1D. We aimed to determine real-world CGM accuracy in hospitalized adults with T1D.
Materials and Methods:
In this multicenter retrospective observational study, we compared CGM interstitial fluid glucose with reference blood glucose (capillary/whole-blood point-of-care [POC], blood gas [GAS]) in adults with T1D requiring multiday admissions during 2020–2023 across three health services in Australia. Patients requiring dialysis or admitted under pediatric/obstetric/palliative care/psychiatry units were excluded. CGM accuracy was assessed by comparison with time-matched (±5 min) reference glucose measures, utilizing median absolute relative difference (ARD), mean ARD (MARD), and consensus error grid (CEG) analysis.
Results:
In total, 2,199 CGM-reference glucose pairs from 214 admissions (146 patients) were assessed. Overall, mean (SD) ARD was 12.8% (13.1) and median (IQR) ARD was 9.4% (3.7–17.7). MARD for CGM-POC pairs was 12.3%; MARD for CGM-GAS pairs was 14.3%. In CEG analysis, 99.3% of glucose pairs were within zones A/B. Accuracy was lower in critical care compared with noncritical care wards (MARD 16.1% vs. 12.0%, P < 0.001).
Conclusions:
In this real-world multicenter study, CGM glucose agreed well with reference blood glucose, suggesting modern CGM devices could be safely and effectively used in hospitalized adults with T1D. Further prospective studies of CGM accuracy with newer generation devices across different scenarios will further elucidate inpatient CGM accuracy and safety.
Introduction
The prevalence of diabetes is high in many hospitals, affecting up to 30% of adults admitted to hospitals across different continents. 1 –3 Inpatients with diabetes are at high risk of adverse glycemia, which is associated with increased inpatient morbidity and mortality. 4
Appropriate glycemic management in hospital improves patient outcomes, 5,6 but is contingent upon the accuracy of glucose measures. Current inpatient glucose monitoring is predominantly performed by point-of-care (POC) capillary blood glucose (BG) measures via finger prick, with additional blood gas (GAS) and plasma glucose measures via venesection where required. These are performed, at most, only a few times per day, resulting in a limited “snapshot” of a patient’s continuous glycemic status. Depending upon local health system resources, POC BG measures are documented in the hospital’s medical records either through manual transcription onto paper charts, manual entry into electronic medical record (EMR) charts, or automated electronic entry into EMR charts via “connectivity” or networked BG meters. 7 Accuracy of glucose values and blood test times may be more limited where manual entry is required due to transcription delays or errors, whereas data fidelity is higher with automated entry.
More recently, subcutaneous continuous glucose monitoring (CGM) technology has enabled minimally invasive interstitial fluid glucose (ISFG) measures as an estimate of BG, often without the need for finger prick testing. Modern CGM devices measure ISFG every 1–5 min and can be linked to a health care provider or health service via web-based CGM software, providing both patients and clinicians with access to comprehensive real-time continuous glycemic information. In the community setting, CGM technology has greatly improved patient and glycemic outcomes. 8,9
CGM use in hospital, likewise, has the potential to improve glycemia in the acute setting and potentially reduce nursing workload. 10 –13 To this end, the American Diabetes Association’s 2024 “Standards of Care in Diabetes” include the recommendation that people using CGM should continue its use “during hospitalization if clinically appropriate.” 14 However, current regulatory approval for CGM use in hospital remains limited, with no subcutaneous CGM device with wireless transmission of data approved by the U.S. Food and Drug Administration (FDA) or obtaining a Conformité Européenne (CE) Mark for use in hospitalized people. 12 The Medtronic Sentrino device is approved for in-hospital use in Europe but requires a wired physical connection for transmission of glucose data. For all other subcutaneous CGM devices, accuracy concerns for use in hospital exist predominantly due to potential alterations in tissue perfusion with acute illness, as well as exposure to interfering medications, radiological studies, or surgical procedures (especially those requiring diathermy). 15 Establishing CGM device accuracy in hospital is crucial to ensure this technology can be safely applied to the inpatient setting.
Existing studies of CGM use in hospital predominantly assess accuracy in people with type 2 diabetes (T2D). 16 –19 However, the incidence of T1D is increasing 20 and people with T1D have much greater uptake of CGM, 21 as well as higher risk of hospitalization. 22 Given FDA validation criteria for integrated CGM systems requires a comparison of identical time-matched ISFG to laboratory glucose measures to ensure there are “robust clinical data demonstrating the accuracy of the device in the intended use population,” ideally inpatient diabetes accuracy studies should include populations with T1D. 23,24
In this real-world study, we aimed to assess accuracy of in-hospital CGM compared with BG monitoring in adults with T1D using CGM who were admitted to the hospital.
Materials and Methods
Patients
We conducted the CONFIDE-1 study (CONtinuous glucose monitoring For Inpatients with DiabEtes—type 1), a multicenter retrospective observational study in which we screened all adult patients with T1D requiring multiday acute hospital admissions from July 2020 to December 2023, inclusive, across three health services in Melbourne, Australia (Eastern Health [EH], Melbourne Health [MH], Peninsula Health [PH]), comprising six major metropolitan, inner suburban, and outer suburban hospitals.
We included patients who were already using their own FreeStyle Libre® Libre 2 (Abbott Diabetes Care Inc, VIC Australia), Dexcom® G5 or G6 (DexCom Inc, CA, USA), and Medtronic Guardian™ 3 (Medtronic, MN, USA) CGM devices prior to elective or emergent acute admissions, including in critical care and noncritical care wards. Patient CGM glucose data previously linked to the health service’s corresponding web-based CGM software accounts (Libreview, Dexcom Clarity, and Medtronic Carelink websites) for clinical care purposes was downloaded for analysis.
We excluded patients with end-stage kidney disease requiring dialysis; patients admitted under pediatric, obstetric, palliative care, psychiatry, or subacute units; and patients without any CGM ISFG or BG measures recorded during their admission.
Materials
POC measures were performed using the following BG meters: Accu-Chek® Guide (Roche Diabetes Care, Rotkreuz, Switzerland) at EH, Nova StatStrip® (Nova Biomedical, MA, USA) at MH (Royal Melbourne Hospital), or FreeStyle® Optium Neo H (Abbott Diabetes Care, CA, USA) at PH; and GAS measures were performed using GEM® 5000 (Werfen, Barcelona, Spain) or ABL90/ABL800 FLEX (Radiometer, Copenhagen, Denmark). At each health service, hospital policies mandate daily glucose meter quality control checks by ward nursing staff. Glucose measures outside the device’s reportable ranges were excluded for accuracy analyses (40–400 mg/dL for Dexcom® and Medtronic Guardian™ CGM devices; 40–500 mg/dL for FreeStyle Libre® CGM devices in Australia; 10–600 mg/dL for Nova StatStrip® and Accu-Chek® Guide POC glucose meters; 20–500 mg/dL for FreeStyle® Optium Neo H POC glucose meters).
Accuracy analyses
We assessed CGM accuracy by time-matching reference BG (capillary/whole-blood POC and GAS) to the closest CGM ISFG measure within 5 min.
To perform CGM accuracy analyses, glucose data from this initial full dataset were restricted to a final accuracy analysis dataset by excluding those glucose measures with a clearly identifiable reason for potential inaccuracy (Supplementary Fig. S1), specifically: Manual EMR POC BG entries not accompanied by either a concurrent POC ketone measure or comment stating finger prick testing had been performed, given the potential for nursing staff to manually enter CGM ISFG measures into the EMR as a substitute for a POC BG measure, Patients using a CGM Reader/Receiver device rather than smartphone application, due to possible device time-stamp inaccuracies in Reader/Receiver devices that require users to manually enter date/time settings, and Patients receiving medications during their admission known to interfere with CGM device accuracy, according to manufacturer product information: ascorbic acid >500 mg/day for Libre 2; hydroxyurea or acetaminophen for G5, Guardian 3; and hydroxyurea or supratherapeutic acetaminophen for G6.
For a given time-matched glucose pair, absolute relative difference (ARD) was calculated as the absolute difference between the CGM ISFG and the synchronous reference BG, divided by reference BG. Population-level, or aggregate, mean ARD (MARD) and median ARD results were calculated using ARD results from all time-matched glucose pairs in the study cohort. Absolute differences between time-matched glucose pairs were also calculated and summarized as mean absolute difference (MAD) and median absolute difference. Patient-level MARD was calculated as the mean of all patient MARD results as determined from all time-matched glucose pairs for each individual patient; patient-level median ARD results were similarly calculated.
Subgroup accuracy analyses were reported according to reference BG source, CGM device model, glucose stratum, and ward acuity.
CGM accuracy was also assessed according to %15/15, %20/20, and %30/30 metrics, which are reported as percentage of glucose pairs within ±15/20/30 mg/dL when reference BG is ≤100 mg/dL, or within ±15/20/30% when reference BG is >100 mg/dL, respectively.
To assess CGM sensor lag, a time series offset analysis was undertaken. 25,26 CGM ISFG measures were linearly interpolated between existing CGM glucose measures, in 1-min intervals; and automated POC BG measures were offset in 1-min increments (within a −10 to +10 min window) to obtain 21 time-offset results from each POC test. Interpolated CGM glucose measures were then time-matched (within the same minute) with the offset POC BG measures, and MARD calculated for each offset increment. The offset time associated with the lowest MARD was used as an estimate of CGM sensor lag time.
Statistical analysis
For baseline and outcome data, continuous variables were reported as mean and standard deviation (SD) for normally distributed parameters; median and interquartile range (IQR) for nonparametric parameters; and number and percentage for dichotomous variables.
Wilcoxon rank sum test was performed for unpaired two-group comparisons of nonparametric variables. No adjustment for multiple comparisons was performed, and reported results should be considered hypothesis generating.
Additional accuracy assessments performed included Consensus (Parkes) error grid (CEG) 27 and Surveillance error grid (SEG) 28 (accessed via the Diabetes Technology Society website at https://www.diabetestechnology.org/seg) analyses, as well as Reduced Major Axis regression (where a 95% confidence interval [CI] of the regression slope that includes 1 indicates that there is no significant proportional bias, whereas a 95% CI of the intercept that includes 0 indicates that there is no significant fixed bias). 29
Statistical analysis was performed using R version 4.4.1 (R Foundation for Statistical Computing, Vienna, Austria). Additional analyses for Reduced Major Axis regression analyses were performed using R package “lmodel2,” and Consensus Error Grid analyses were performed using R package “ega.”
Ethics approval
Ethics approval for this study was obtained from each health service’s Office for Research prior to study commencement (EH: QA23-105–102749; MH: QA2023122; PH: SA/103943/PH-2023). Individual patient consent for this analysis was not considered to be required by the relevant human research ethics committees as data was only aggregated in a deidentified format, patients had previously provided explicit consent for their health services to access this data, and this analysis would be reasonable usage of the data for quality assessment and improvement purposes.
Results
We examined a total of 4095 admissions from 1975 adult patients with T1D requiring multiday acute hospital admissions across three health services between July 2020 and December 2023 who were admitted under medical and surgical units.
Of these, 328 admissions (216 patients or 11%) had at least one time-matched CGM-reference BG pair available during their admission, with the full dataset comprising a total of 6951 CGM-reference BG pairs comprising 6348 CGM-POC and 603 CGM-GAS glucose pairs. Of Dexcom CGM users, 4% (2/52) used a Dexcom “Receiver” device, while 96% used the Dexcom phone app (“Dexcom G5” or “Dexcom G6”) to receive glucose data. Of Libre CGM users, 22% (32/146) used an intermittently scanned Libre “Reader” device, while 78% used the Libre phone app (“LibreLink”) to receive glucose data.
After excluding glucose measures with a clear reason (based on the clinical scenario) for any potential inaccuracy (Fig. 1), the accuracy analysis dataset consisted of 214 admissions (146 patients) with 2199 CGM-reference BG pairs (1708 CGM-POC and 491 CGM-GAS glucose pairs). The mean (SD) study population glucose was 211 mg/dL (SD 100). Each patient contributed a median (IQR) of 5 (2–14) time-matched glucose pairs over their admission (median 2.9 day stay). Baseline demographic data for the accuracy analysis dataset are presented in Table 1.

Study flow diagram of patients with included and excluded glucose pairs. BG, blood glucose; CGM, continuous glucose monitoring; EMR, electronic medical record; POC, point-of-care. Sum of admissions/patients in Excluded groups and Accuracy Analysis Dataset exceeds Full Dataset as some patients had both manual (excluded) and automated (included) EMR POC BG entries recorded during their admission.
Baseline Characteristics
Sum is greater than number of patients as some patients changed CGM devices between admissions.
BG, blood glucose; CSII, continuous subcutaneous insulin infusion; CGM, continuous glucose monitoring; DKA, diabetic ketoacidosis; HbA1c, hemoglobin A1c; ICU, intensive care unit.
CGM accuracy analyses
Utilizing the accuracy analysis dataset, inpatient CGM use was associated with an overall MARD of 12.8% (comprising 2199 CGM-reference BG pairs). Compared with POC BG, MARD was 12.3% (1708 CGM-POC pairs) and compared with GAS BG, MARD was 14.3% (491 CGM-GAS pairs). Population-level ARD results and absolute difference results are presented in Table 2 and Supplementary Table S1, respectively. Patient-level ARD results are presented in Supplementary Table S2.
Mean and Median Absolute Relative Difference of Population-Level Continuous Glucose Monitoring Measures Compared with Reference (Synchronous) Blood Glucose
ARD, absolute relative difference; BG, blood glucose; GAS, blood gas; ICU, intensive care unit; IQR, interquartile range; MARD, mean absolute relative difference; POC, point-of-care; SD, standard deviation.
Accuracy was significantly lower in critical illness requiring intensive care unit (ICU) admission (median Acute Physiology and Chronic Health Evaluation [APACHE] II 30 score of 11; IQR 6–15) than noncritical care wards for both pooled CGM-BG glucose pairs (MARD 16.1% vs 12.0%, and median ARD 12.5% vs. 8.9%, respectively, P < 0.001) as well as for CGM-GAS glucose pairs (MARD 17.9% vs. 12.6%, and median ARD 13.2% vs. 9.2%, P < 0.001) (Table 2). In addition, among patients admitted with diabetic ketoacidosis (DKA), MARD was 13.7% and median ARD was 10.0% (595 pooled CGM-BG pairs). Among patients admitted with DKA, those who required admission to ICU had numerically higher ARD results compared to those who did not require admission to ICU (MARD 16.7% vs. 12.8%, median ARD 11.0% vs. 9.7%, P = 0.078, comparing 140 to 455 pooled CGM-BG pairs).
CGM accuracy results according to %15/15, %20/20, and %30/30 metrics are presented in Table 3. In CEG analysis, 99.6% of CGM-POC pairs, and 98.3% of CGM-GAS pairs, were within the clinically benign zones A and B (Fig. 2 and Supplementary Table S3). Similarly in SEG analysis, 99.6% of CGM-POC pairs, and 98.6% of CGM-GAS pairs, were within the “None” or “Slight” Risk level categories (Supplementary Table S4 and Supplementary Fig. S1).
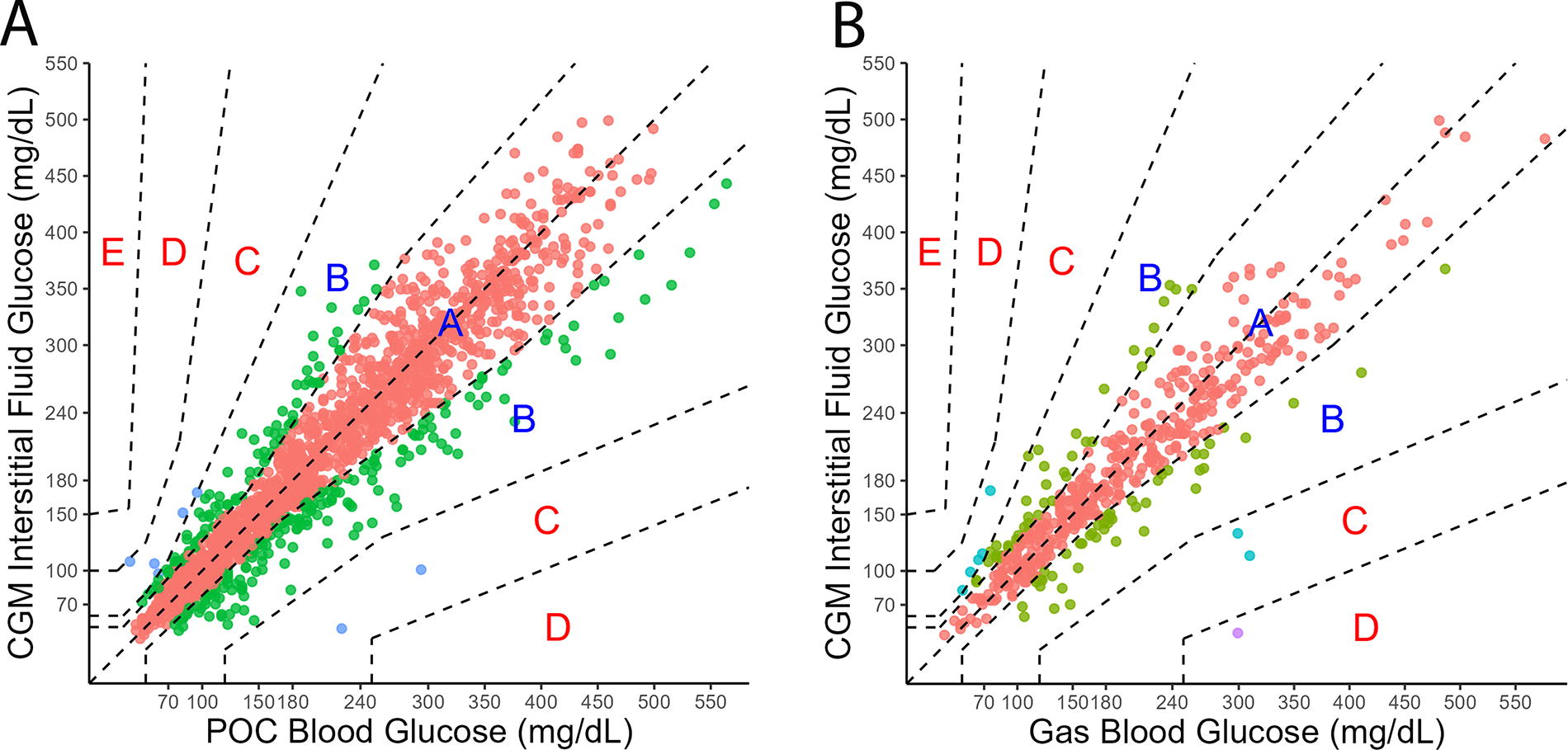
Consensus error grid comparison of continuous glucose monitoring interstital fluid glucose vs. blood glucose. (Panel
Continuous Glucose Monitoring Accuracy Results According to %15/15, %20/20, %30/30 Metrics a
where %x/x indicates % of glucose readings within ±x mg/dL when reference glucose ≤100 mg/dL or within ±x% when reference glucose >100 mg/dL.
BG, blood glucose.
Reduced Major Axis regression was performed (Table 4), with results from the two most prevalent CGM models (Libre 2 and Dexcom G6) suggesting neither CGM model experienced proportional bias (with the regression slope 95% CI including 1), but both demonstrated a degree of fixed bias (given regression intercept 95% CI did not include 0). Libre 2 had a fixed bias of −8.59 mg/dL (95% CI: −12.30 to −4.95), whereas Dexcom G6 had a fixed bias of +10.22 mg/dL (95% CI: 5.43 to 14.88), compared with pooled reference BG.
Continuous Glucose Monitoring Accuracy Results According to Reduced Major Axis Regression Analysis
Indicates proportional bias present.
Indicates fixed bias present.
95% CI, 95% confidence interval; CGM, continuous glucose monitoring.
Time series offset analysis
For both automated and manual EMR entry of POC BG measures, time differences to nadir MARD value were calculated after applying time series offset analyses (Fig. 3). Nadir MARD for automated EMR entry POC BG occurred with a +5 min offset to the POC BG EMR entry time, suggesting overall CGM sensor lag was 5 min in our study. In contrast, nadir MARD for manual EMR entry POC BG was in the opposite direction, with a −3 min offset to the EMR entry time, hence there was an overall 8-min time difference between automated and manual EMR entry POC BG measures to achieve MARD nadir. This would be consistent with a delay between performing a POC test at the bedside and manually entering the glucose result into the EMR workstation. It is also relevant to note MARD for the time-offset glucose pairs was lower than MARD for the original time pairs (Fig. 2).

Time offset analysis of automated vs. manual electronic medical record entry point-of-care glucose. (Filled circles: automated EMR entry; open triangles: manual EMR entry; gray arrow: sensor lag of 5 min). EMR, electronic medical record; MARD, mean absolute relative difference.
Glucose values excluded from accuracy analysis
Substantial differences in the ARD results for patients using CGM Reader/Receiver devices (especially for Dexcom “Receiver” devices in our study sample) compared with patients using smartphones suggest inaccurate date/time settings in some Reader/Receiver devices (Supplementary Table S5). The markedly lower ARD results for the excluded manually entered POC BG measures is consistent with substituting POC BG measures with CGM measures (Supplementary Table S5). The ARD results in the presence of potential interfering medications with CGM are also listed in Supplementary Table S5.
Discussion
In the CONFIDE-1 real-world multicenter observational study of inpatient CGM use and accuracy in hospitalized adults with T1D, we assessed data across a range of CGM device models and reference BG methods. The CONFIDE-1 study results suggest that inpatient CGM use in adults with T1D has satisfactory accuracy when compared with pooled BG measures, with an overall MARD of 12.8% and a median ARD of 9.4%. This is comparable with CGM MARD accuracy (9.2–9.9%) when tested in later models (FreeStyle Libre 2, Dexcom G6) under optimal experimental conditions (compared with laboratory glucose measures) outside of the real-world acute health care setting. 31,32 The very high number of glucose pairs in zones A and B of error grid analyses suggest that differences between CGM and reference BG results are generally clinically benign and unlikely to result in clinically significant differences.
Existing studies of in-hospital CGM accuracy predominantly focus on people with T2D. 16 –19 However, CGM accuracy in people with T1D warrants specific assessment, 24 as apparent CGM accuracy may be different in people with T1D, compared with people with T2D, due to greater glycemic variability. 33 The CONFIDE-1 study of pooled Abbott, Dexcom, and Medtronic CGM device model usage is the largest study reported to date of inpatient CGM use in patients with T1D, and observed that CGM accuracy among adults with T1D was reassuringly similar to previous studies consisting predominantly of adults with T2D (81–100% of study population), which reported noncritical care MARD of 11.0–21.4%, and critical-care MARD of 12.4–17.4%. 16 –18,34,35
In addition, we found that Dexcom G6 had a fixed positive bias of +10.2 mg/dL. This falls between results reported by two small studies, one which reported no significant bias 36 and another which reported positive bias of +20 mg/dL. 37 We also found that Libre 2 had a fixed negative bias of −8.6 mg/dL, consistent with other published reports of Libre and Libre 2. 34,35
These data suggest that assessments of inpatient CGM accuracy are influenced by a combination of CGM device factors (interfering medication use; CGM sensor lag), patient clinical scenario, and health care system factors (health care staff substitution of POC capillary BG with CGM ISFG in the EMR; time delays in manual EMR BG entry).
CGM device
The use of inpatient medications known to interfere with the accuracy of CGM devices was high, especially for CGM models affected by therapeutic doses of acetaminophen (Dexcom G5 and Guardian 3) (Supplementary Table S5). Given the retrospective design of this study, it was not possible to determine whether CGM measures were used to guide diabetes treatment decisions during periods of interfering medication prescription.
When considering inpatient CGM accuracy it is important to appreciate that CGM ISFG measures are usually reflective of slightly delayed estimates of real-time BG levels. Physiological delay of glucose diffusion from the blood into the interstitium, and additional delays from CGM device filtering processes contribute to sensor lag. 38 Our time series offset analysis used networked BG meters with accurate time entry, with POC BG MARD nadir reached by a forward offset of 5 min (Fig. 3) corresponding to overall CGM sensor lag of 5 min, compared with 4 min for Dexcom G6 39 and 2.4 min for Libre 2 40 reported in outpatient studies. During periods of rapid fluctuations in BG, especially during hypoglycemia and immediately posthypoglycemia treatment, time-matched accuracy will be lower due to CGM sensor lag, hence capillary BG measures rather than CGM ISFG should be utilized to guide key treatment decisions.
Patient clinical scenario
Inpatient accuracy differs according to inpatient scenario. We examined CGM accuracy during admission to the ICU or non-ICU wards and observed CGM accuracy was lower during stays in ICU.
In our pooled analysis, CGM accuracy was significantly lower during critical illness requiring ICU ward care, compared with non-ICU care wards (MARD 16.1% vs. 12.0%, P < 0.001), although 98.5% of glucose pairs were still within CEG zones A and B. Previous studies report mixed results regarding the impact of critical illness upon CGM accuracy; 18,41 however, the largest study examining this issue reported lower accuracy in critically ill patients, 18 similar to our study.
Despite the slightly higher MARD during critical illness, the high proportion of glucose pairs in zones A and B of error grid analyses implies that, despite some differences between CGM ISFG and reference BG, use of CGM measures during these inpatient scenarios may not result in adverse management. In some settings, use of CGM in hospital can reduce POC capillary BG testing rates by approximately two-thirds, 11,42 which could greatly improve patient experience and nursing workload in highly acute hospital scenarios.
We did not explore the effects of other inpatient scenarios upon CGM accuracy, including exposure to ionizing radiation or magnetic fields from radiological studies, and electrical diathermy during surgical procedures, for which further studies are recommended.
Health care system
Automated BG entry into the EMR captures accurate glucose level and test time data. Manual BG entry typically occurs minutes after the BG measure is performed, as suggested by our time series offset analyses. In addition, despite the lack of regulatory approvals, substitution of POC BG measures with CGM ISFG measures in the EMR is occurring in real-world practice, as suggested by the much lower MARD and median ARD calculated from excluded manual-entry POC BG measures (Supplementary Table S5). One driving factor for this is likely patient preference for continued CGM use in hospital over finger prick POC testing. 19 While we await endeavors to approve the use of CGM in hospital, it is important to standardize manual data entry processes into EMR to ensure the source of glucose measure is defined. In addition, the use of automated EMR POC BG entry systems is encouraged to ensure the fidelity of glucose data.
The limitations associated with this study include its retrospective, observational nature with the use of unmasked CGM by patients. As such, nursing staff could potentially substitute POC BG measures with CGM measures for manual EMR BG entries, although we excluded POC measures whose provenance was uncertain. In addition, limited laboratory plasma glucose samples were available for accuracy comparisons and some inpatients had data included for more than one hospital admission. Finally, given the relatively low use of CSII in our study population, our ability to assess the impact of CGM accuracy upon CSII dosing algorithms was limited. Future inpatient studies assessing accuracy of newer generation CGM devices, such as the Libre 3, Guardian 4, and Dexcom G7, across a range of differing patient groups and inpatient scenarios will be necessary.
The field of inpatient diabetes management is rapidly evolving, with in-hospital CGM use likely to be transformative, if approved. Inpatient CGM accuracy is influenced by the clinical scenario of the patient, health care system, and CGM device factors. In the CONFIDE-1 study, we observed CGM measures had reasonable accuracy in a real-world hospital setting, with sensor lag on par with performance in experimental laboratory conditions.
The use of inpatient CGM has the potential to transform acute diabetes care in hospitals by enhancing patient and health professional experience, as well as clinical outcomes. Ongoing research efforts to understand the inpatient use and accuracy of CGM devices, including newer generation models, will soon become paramount for delivering better diabetes care in hospital.
Footnotes
Acknowledgments
The authors would like to thank each hospital’s diabetes educators for their efforts linking patient CGM devices with hospital CGM software accounts, as well as the Business Intelligence team (including Liz Singelton and Tim Fazio) at The Royal Melbourne Hospital, the Data Analytics and Insights service at Eastern health, and the Data Analytics and Reporting team at Peninsula Health (including Tanya Ravipati) for their support.
Authors’ Contributions
R.W., M.K., A.C., and S.F.: Involved in conception and design of the study. M.K., A.C., C.C., D.R., and S.F.: Supported methodological decisions. R.W., B.K., and J.T.: Performed data acquisition. R.W.: Performed the statistical analysis and wrote the first draft of the article. M.K., R.B., and S.F.: Provided critical revisions to the article. All authors made a significant contribution to finalizing the article and approved the final version of the article. S.F.: Provided overall study supervision and is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Author Disclosure Statement
S.F. contributes to the advisory panel for Viatris Inc. and Pfizer Inc., has received honoraria for speaker fees for AstraZeneca, Boehringer-Ingelheim, Lilly, Novo Nordisk, and has received honoraria for advisory fees for Medtronic, Mylan, Pfizer, and Sanofi. M.K. has received honoraria for speaker fees for AstraZeneca.
Prior Presentation
Parts of this study were presented in abstract form at the 60th Annual Meeting of the European Association for the Study of Diabetes, Madrid, Spain, September 10–13, 2024, and the Australasian Diabetes Congress, Perth, Australia, August 21–23, 2024.
Funding Information
R.W. is the recipient of an Australian Commonwealth Government RTP Scholarship, ACADI PhD Grant, Fred Knight Research Scholarship, Rowden White Scholarship, and Gordon P Castles Scholarship.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.