
Abstract
Background:
Studies investigating the safety and efficacy of automated insulin delivery (AID) systems in people with cystic fibrosis-related diabetes are limited. There are no published studies investigating the tubeless Omnipod 5 (OP5) AID system.
Methods:
This dual-center retrospective cohort study compared 14 days of baseline continuous glucose monitoring (CGM) data with days 1–90 and 91–180 post-OP5 initiation. Multivariable mixed-effects linear regression models were used to assess changes in glycemic metrics.
Results:
Among the 26 individuals with sufficient data initiating OP5, 65% were female, with a median age of 27.3 years and median diabetes duration of 10.9 years. Six (23%) had a history of solid organ transplant, and 2 (8%) were receiving enteral tube feeds. Participants transitioned to OP5 from multiple daily injections (54%), prior Omnipod generation (31%), or another AID system (15%). CGM time in range (70–180 mg/dL) increased from 54% (95% confidence interval [CI]: 45.0, 63.0) to 64% (95% CI: 57, 71.8, P < 0.001) during the first 90 days and to 62.7% (95% CI: 54.9, 70.5, P < 0.001) during 91–180 days. Time above range (TAR) 181–250 mg/dL and TAR >250 mg/dL improved at 1–90 days and 91–180 days compared with baseline (P = 0.001 and P = 0.002, respectively). There were no significant changes in time below range (54–69 mg/dL, <54 mg/dL) or coefficient of variation. Two individuals discontinued OP5 within 14 days due to persistent hypoglycemia. One adult experienced a hypoglycemic seizure after 3 months of use.
Conclusions:
Use of the OP5 system in youth and adults with CFRD led to significant improvements in multiples measures of hyperglycemia without a change in CGM-measured hypoglycemia over a 6-month period, although patient experience with hypoglycemia may limit sustained use. Given the unique comorbidities and pathophysiology of CFRD, these results emphasize the need for future studies to investigate the safety and efficacy of AID devices in this patient population.
Introduction
Cystic fibrosis (CF) is an autosomal recessive genetic disorder caused by dysfunctional or absent CF transmembrane conductance regulator (CFTR) protein that leads to progressive lung disease, gastrointestinal complications, and early mortality. Therapeutic advancements in recent years have revolutionized care for people with CF (pwCF), leading to a significant improvement in predicted median survival increase from 37.7 years in 2008 to 61.4 years in 2023. 1 The prevalence of CF-related diabetes (CFRD) increases with age, affecting up to 30%–50% of adults with CF. 1 CFRD is associated with compromised nutritional status and lung function, decreased post-transplant survival, and increased mortality. 2 –5 The risk of developing CFRD is higher in individuals with more severe genotypes. 4 Although the introduction of highly effective CFTR modulator therapy (HEMT) in 2019 dramatically improved lung function and nutritional status for many pwCF, rates of CFRD continue to rise. 6 –8
Insulin is the only recommended treatment for CFRD and has been shown to improve CF-specific outcomes, including pulmonary function, nutritional status, and mortality. 9 Individuals with CFRD experience both insulin deficiency and insulin resistance, leading to variable insulin requirements, particularly in the setting of pulmonary exacerbations, supplemental nutrition therapy, and solid organ transplantation. Insulin therapy is associated with an increased treatment burden in pwCF, which can present a barrier to achieving glycemic targets. 10
Automated insulin delivery (AID) systems are increasingly used in the management of type 1 diabetes (T1D) and have been associated with improved glycemic control and reduced emotional burden. 11 –13 However, just 18.5% of pwCFRD reported using pump therapy in 2023, and no AID systems are specifically approved for CFRD management. 1 Limited research in pwCFRD has shown an improvement in glycemic control with selected AID systems, including increased percentage time in range (TIR, 70–180 mg/dL). 14 –16 To date, no studies have evaluated the outcomes of pwCFRD using the Omnipod 5 (OP5) tubeless AID system. This retrospective study aimed to evaluate the safety and efficacy of OP5 use over 6 months in youth and adults with CFRD.
Methods
We conducted a dual-center retrospective cohort study evaluating youth and adults with CFRD cared for at the Massachusetts General Hospital (MGH) and Children’s Hospital of Philadelphia (CHOP) CF Centers. The protocols were approved by each hospital’s institutional review board with a data sharing agreement between the institutions. As this was a retrospective analysis, written informed consent was not obtained.
Study population
Individuals with a diagnosis of CFRD who had started OP5 for their clinical diabetes care between July 2022 and October 2024 were included. Individuals were excluded from analyses if there were insufficient baseline or follow-up continuous glucose monitoring (CGM) data, defined as less than 14 days of CGM data with a wear time ≥70%. All enrolled individuals received education regarding the different diabetes management strategies, particularly multiple daily injection (MDI) versus AID pump systems, the currently available AID systems, and the unique pros and cons of each before making their own treatment decision. Individuals received formal Omnipod training from an in-house diabetes educator (CHOP) or Insulet representative (MGH) before pump initiation. Initial pump settings, including target glucose value, varied by patient/provider.
Clinical data collection
All demographic and clinical data were recorded from the electronic medical record. Baseline anthropometric, spirometry, and hemoglobin A1c (HbA1c) data were obtained from individuals’ in-person clinic visits at the time closest to initiation of the OP5. Other clinical data included CFTR genotype, pancreatic insufficiency (defined as use of pancreatic enzyme replacement requirement), history of solid organ transplant, medications, hospitalizations, and pulmonary exacerbations over the 3 months preceding OP5 start, previous diabetes regimen, use of gastrostomy tube feeds, and spirometry results (percentage predicted forced expiratory volume in 1 s [FEV1] and forced vital capacity [FVC]). Follow-up clinical data were obtained from the in-person clinic visit closest to 180 days post-OP5 initiation.
CGM measures and OP5 AID data
Baseline CGM data were downloaded from the Dexcom Clarity™ and/or Glooko™ applications. CGM data were collected from the 14 days preceding OP5 start for those with ≥70% CGM active time during that period; for those with <70% wear time, any 14 days of CGM data from the 30 days before OP5 initiation were used. Follow-up CGM and insulin delivery data from days 1 to 90 and days 91 to 180 after OP5 initiation were downloaded from the Glooko software application.
The primary outcome was percentage of time spent in target range 70–180 mg/dL (TIR). Secondary outcomes included glucose management indicator (GMI), average glucose (AG), coefficient of variation (CV), time below range (TBR, 54–69 mg/dL, <54 mg/dL), and time above range (TAR, 181–250 mg/dL, >250 mg/dL). AID metrics included total daily dose of insulin, time in automated mode, percent basal and bolus delivery, number of boluses per day, number of carbohydrate entries per day, and percent overrides. Total daily dose of insulin in units/kg/day was calculated if a weight was available from 120 to 210 days after OP5 initiation. Baseline weight was used for calculation if no follow-up weight value was available (days 1–90, n = 2, days 91–180, n = 1).
Statistical analysis
Statistical analyses were performed using STATA (version 18, 2024; College Station, TX: StataCorp LLC). All tests were two-sided, and P < 0.05 was considered statistically significant. Normality was assessed for all variables using the Shapiro–Wilk test. Summary data were reported as median (interquartile range [IQR]) due to skew or absolute number (percentage) for continuous and categorical data, respectively.
Multivariable mixed-effects linear regression models controlling for clinical site were used to determine the change in key glycemic metrics from baseline to days 1–90 and days 90–180. Unadjusted and adjusted outputs from our regression analyses are presented as beta-coefficient (95% confidence interval [CI]).
Results
A total of 35 pwCFRD were identified as starting the OP5 during the study period (Fig. 1). Five were missing baseline CGM data. One person had very limited use of the OP5 and ultimately had insufficient data for inclusion; two other subjects receiving low-dose insulin at baseline discontinued OP5 use within 14 days of initiation due to persistent hypoglycemia. Another had complete clinical data and clinical note confirmation of ongoing OP5 use, however, CGM and Glooko data were missing from days 91 to 180. Twenty-six had sufficient baseline CGM and 90-day data available for review and were included in the analyses. All pediatric individuals were enrolled at CHOP and all apart from one adult were enrolled at MGH.

Consort diagram depicting the individuals included and excluded from the final analysis.
Baseline clinical characteristics of the analyzed sample (n = 26) are outlined in Table 1. The ages of participants ranged from 11.2 to 58.0 years, including six individuals younger than 18 years. Seventeen (65%) participants were female, 14 (54%) were homozygous for the F508del mutation, and 23 (88.5%) had pancreatic insufficiency. Eighteen (69%) participants were taking CFTR modulator therapy. Two (8%) individuals required overnight gastrostomy tube feeds, and six (23%) individuals had a history of solid organ transplantation. The median duration of CFRD was 10.9 years (IQR: 4.6, 17.1), and mean HbA1c was 6.8% (IQR: 6,7.6). The majority of individuals (n = 14, 54%) transitioned to the OP5 from multiple daily injection (MDI) therapy, although eight (31%) were using an older version of the Omnipod without AID and four (15%) were using a different AID system at baseline.
Baseline Characteristics
Data displayed as # (%) or median (interquartile range).
n = 5.
BMI, body mass index; CFRD, cystic fibrosis-related diabetes; CFTR, cystic fibrosis transmembrane conductance regulator; CHOP, Children’s Hospital of Philadelphia; FEV1, forced expiratory volume in 1 s; HbA1c, hemoglobin A1c; MGH, Massachusetts General Hospital.
CGM outcomes before and after OP5 initiation are presented in Table 2. TIR increased by 10.4 percentage points [95% CI: 5.7, 15.1] from 54% (95% CI: 45.0, 63.0) at baseline to 64.4% (95% CI: 57.0, 71.8) during the first 90 days of use, with sustained improvement during days 91–180 (62.7%, [95% CI: 54.9, 70.5], P < 0.001; Fig. 2A). The goal TIR of >70% was attained in 46.2% of individuals during days 1–90 (n = 12) and in 42.3% (n = 11) during days 91–180. There were significant improvements in AG (Fig. 2B), GMI, TAR 181–250 mg/dL, and TAR >250 mg/dL during both periods compared with baseline (P < 0.05 for all). TBR <54 mg/dL, TBR 54–69 mg/dL, and CV did not change significantly after OP5 initiation (P > 0.05 for all).
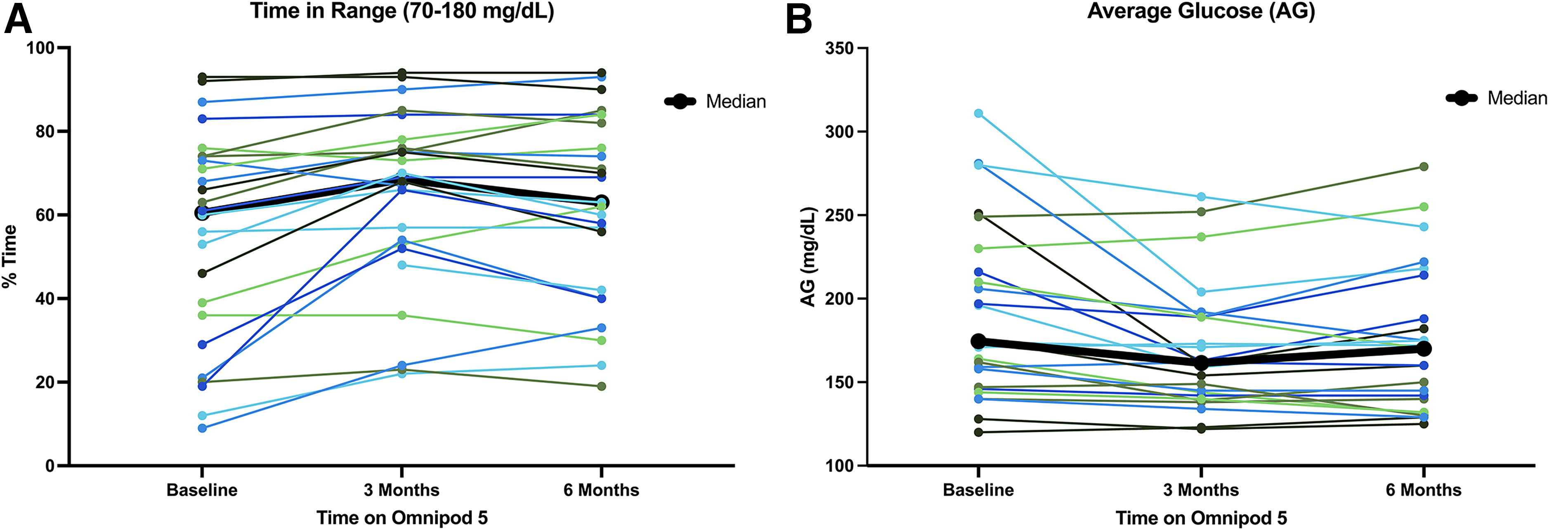
Change in key continuous glucose monitoring (CGM) measures from baseline to days 1–90 and 91–180 post-Omnipod 5 (OP5) initiation. The figure depicts the changes in two glycemic measures (% time in range 70–180 mg/dL and average glucose [AG]) with each individual represented by a different color. Thicker black lines represent the median across all individuals.
Changes in Glycemia After 90 and 180 Days of Omnipod 5 Use
Data displayed as beta-coefficient (95% confidence interval [CI]).
One individual had complete clinical data and clinical note confirmation of ongoing Omnipod 5 (OP5) use; however, continuous glucose monitoring (CGM) and Glooko™ data were missing from days 91 to 180 and therefore not included in the analysis.
P values comparing days 1–90 with baseline data.
P values comparing days 90–180 with baseline data.
CV, coefficient of variation; GMI, glucose management indicator; TAR, time above range, TBR, time below range; TIR, time in range.
CGM active time was 93% (IQR: 81.1, 97.1) and 97% (IQR: 77.8, 100) during days 1–90 and 91–180 of OP5 use, respectively (Table 2). Despite no change in CGM active time, time in automated mode declined from days 1–90 to 91–180 (89% [IQR: 71, 97] vs 83% [IQR: 68, 97], P = 0.03).
There were no significant changes in total daily dose of insulin in units or in units/kg/day from baseline to 90 days or 180 days. The median boluses per day exceeded 3 throughout the 180-day study period (Table 3). Weight, body mass index (BMI), and ppFEV1 did not significantly differ before or after OP5 initiation (Table 4).
Changes in Insulin Delivery After 90 and 180 Days of Omnipod 5 Use
Data displayed as median (IQR).
n = 23.
P values comparing changes in total daily insulin dose (TDD) and TDD per kg were nonsignificant.
Changes in Additional Clinical Metrics
Adults only (n = 20).
FVC, forced vital capacity.
Two youth with poor adherence to bolus-only insulin therapy before OP5 initiation chose to discontinue OP5 within 14 days due to excessive hypoglycemia with >10% TBR <70 mg/dL. One adult who experienced a severe hypoglycemic event shortly after 90 days of OP5 use continued to use the OP5 thereafter. This patient developed loss of consciousness with seizure activity while wearing the OP5, with CGM data showing glucose <40 mg/dL at the time of the event. She recovered with emergency medical service (EMS) assistance, and subsequent medical evaluation excluded other inciting causes. The seizure did not occur postprandially and was not related to a late meal announcement. This individual had no seizure history, a normal subsequent neurology evaluation, and has not had any additional seizures since that time.
Two patients received overnight continuous gastrostomy tube feeds before and after transitioning to the OP5. Given that the OP5 algorithm does not allow for adjustment of basal rates in auto mode, the OP5 was changed to manual mode overnight, with higher basal rates programmed to cover the carbohydrate intake of the continuous feeds.
Discussion
In this multicenter retrospective cohort analysis, initiation of the OP5 AID system in youth and adults with CFRD resulted in significant improvements in TIR, GMI, and TAR with a similar amount of daily insulin usage. These improvements occurred within 90 days of OP5 initiation and were sustained over 6 months of AID use; however, a majority of patients did not achieve the recommended TIR threshold of 70% during the follow-up period. Although there were no statistically significant changes in measures of glycemic variability or TBR, one participant experienced a hypoglycemic seizure, and two individuals discontinued OP5 due to persistent hypoglycemia. To our knowledge, this is the first study investigating the use of the OP5 and its effect on glycemia in CFRD.
The OP5 received Food and Drug Administration (FDA) approval for the management of T1D in individuals 6 years and older in January 2022 and for ages 2 and older since August 2022. It also received FDA approval for the management of T2D in individuals ≥18 years of age in August 2024. The pivotal trial of the OP5 system in 235 individuals with T1D (111 youth, 129 adults) showed significant reductions in HbA1c (−0.7%) and improvements in TIR (+15% in youth and +9% in adults). 17 Several subsequent studies looking at the effect of the OP5 system on real-world glycemic outcomes in people with T1D found similar significant sustained improvements in glycemia. 18,19 One recent retrospective analysis of 69,902 OP5 users in the United States, age ≥2 years, reported median TIR of 64.2%, whereas a pediatric study showed an 11 percentage point improvement in TIR in the first 90 days of OP5 use. 20 We found similar changes in TIR (+10.4 percentage points) and final TIR (64.4% during days 1–90 and 62.7% during days 91–180) in individuals with CFRD, suggesting that the OP5 may perform similarly in this patient population as in T1D.
Although there was no significant change in CGM-measured hypoglycemia, the attrition of two individuals due to hypoglycemia and the occurrence of a hypoglycemic seizure in this small sample size are noteworthy. Individuals with CFRD commonly have residual endogenous insulin secretion, which makes them more vulnerable to postprandial reactive hypoglycemia. 21,22 In practice, entering carbohydrate boluses before meals may blunt the postprandial glucose excursions that stimulate endogenous insulin secretion and could be particularly important in this form of diabetes when using the OP5. Further studies will be needed to investigate strategies to minimize hypoglycemia in pwCFRD with this device. 23 –25
Similarly, although studies in adults with T1D using the OP5 demonstrated decreases in glycemic variability as measured by CV with use, 17 this effect was not identified in our study in CFRD, and the 6-month time point (38.1%) exceeded the international recommendations for CV (<36%). PwCF are known to have significant glycemic variability and dysregulated insulin secretion; early in the disease course this is primarily due to the loss of first-phase insulin secretion. 8,9,24 However, dysregulated endogenous insulin secretion typically persists throughout the disease course in pwCFRD and contributes to ongoing postprandial glycemic variability. These data should be carefully considered in light of emerging evidence linking glycemic variability to microvascular complications, particularly as pwCFRD are living longer and the prevalence of diabetes complications will likely increase. 26,27
Although there are currently no FDA-approved AID systems for the management of CFRD, there is a growing body of evidence supporting their potential beneficial impact on glycemia in this form of diabetes. A prospective study published in 2009 found significant improvements in fasting and postprandial hyperglycemia, HbA1c, body weight, and dual-energy x-ray absorptiometry (DXA)-measured lean mass among nine individuals who transitioned to a nonautomated insulin pump without CGM over a 6-month period. 28 We previously conducted a dual-center retrospective study of 13 adults and adolescents with CFRD, comparing baseline glycemic control to 1 and 3 months after transitioning to the Tandem T:slim X2 with Control IQ™ AID system. Control IQ utilization resulted in significant improvements in TIR (baseline 54.3% vs 1 month 70.9% vs 3 months 69.5%, P 0.001), alongside reductions in TAR and standard deviation, without significantly increasing hypoglycemia. 15 A random-order crossover trial in 20 adults with CFRD compared 14 days of usual diabetes care with 14 days of the iLet Bionic Pancreas™, revealing significant improvements in TIR (75% vs 62%, P = 0.001) and AG (150 mg/dL vs 171 mg/dL, P = 0.007) with use of the iLet. Although participant-reported subjective hypoglycemia was higher with the iLet, there was no increase in CGM-measured TBR or severe hypoglycemia episodes. 16 We did notice a trend toward decrease in time in automated mode over the course of our study; however, this decrease was similar to that seen in other diabetes populations and likely reflects technology fatigue as opposed to a CF-specific process. 18 Future studies are needed to determine whether differences in AID algorithms may render one system superior for use in this population given the unique underlying pathophysiology of CFRD.
pwCFRD face distinct challenges in the management of their diabetes. In addition to risk of hypoglycemia from endogenous insulin production, pwCFRD often experience fluctuations in insulin requirements related to changes in insulin resistance in the setting of illness and glucocorticoid treatment, which can be challenging to manage with AID. In addition, nutritional needs are higher in this population to optimize pulmonary function. In this study, two participants used overnight gastrostomy tube feeds with the OP5, which often requires work-arounds with AID systems to optimize carbohydrate coverage over the 8–12-h feeding duration. This study represents the first report of successful management of overnight feeds while using the OP5 by utilizing manual mode overnight during feeding, which can be a useful strategy for clinicians to consider in using AID in these clinical scenarios.
For pwCF already facing significant day-to-day medical burden, the addition of CFRD management, including frequent glucose monitoring, counting carbohydrates, administering insulin, and preventing hypoglycemia, negatively affects quality of life (QoL). 10,29 A multicenter prospective study in 115 adults before and 3 months after transition to the OP5 found significant improvements in diabetes distress scores, hypoglycemia confidence measures, diabetes treatment satisfaction, sleep quality, and overall well-being metrics 30 ; how the OP5 impacts patient-reported outcomes in CFRD will be an important area of future research. Historically, the perception and utilization of diabetes technology within the CF community have been relatively poor. 29,31,32 An online survey of 83 pwCF (61% with CFRD) and 35 parents of children with CF (34% with CFRD) found low use of insulin pumps (29%) compared with the T1D population. Furthermore, discontinuation rates of both CGM (19%) and insulin pumps (28%) were higher than typically seen within the T1D community. 31 Additional studies are needed to determine whether AID use can improve QoL in pwCFRD and to identify strategies to encourage sustained use.
The strengths of this study include the multicenter data collection, inclusion of both youth and adults with CFRD, utilization of CGM data for baseline glycemic status characterization, and the extended period of data accrual post-AID system initiation (180 days). However, there are several notable limitations that require consideration. Although we were able to detect significant changes in glycemic status, the study sample size was relatively small. Power was limited to detect an effect of the OP5 on clinical metrics pertinent to this patient population, including weight, BMI, and pulmonary function. Individuals were also from a limited geographical area and received care from two centers, limiting the diversity of the sample. Data collection was also limited by the retrospective nature of the study. Similarly, certain data of interest that may impact glycemic status could not be obtained, such as detailed dietary histories, episodes of symptomatic hypoglycemia, socioeconomic factors, educational level, and patient-reported outcomes.
Conclusions
Initiation of the OP5 AID system was associated with sustained improvements in TIR, TAR, AG, and GMI in youth and adults with CFRD over 6 months. Although no difference in CGM-measured hypoglycemia was identified, AID attrition due to hypoglycemia and a severe hypoglycemic event occurred within this small sample. To our knowledge, this is the first study investigating the impact of the OP5 in pwCFRD, and further studies are needed to understand the potential long-term benefits of the OP5 and other AID systems on dysglycemia, pulmonary function, nutritional status, mortality, and QoL in this patient population.
Footnotes
Acknowledgment
The authors thank the patients and the clinical and research teams of the MGH and CHOP CF centers.
Authors’ Contributions
K.J.S., M.R., J.D., and B.E.M. researched and analyzed data and wrote the article. B.E.M., K.J.S., and M.S.P. conceived and designed the study and reviewed and edited the article. K.J.S., M.S.P., and B.E.M. are the guarantors of this study and, as such, had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Author Disclosure Statement
M.S.P. has received research funding and honoraria from Vertex Pharmaceuticals, investigator-initiated research funding from Dexcom and Samsung, and serves on the scientific advisory board of Anagram Therapeutics. B.E.M. receives consulting and speaker honoraria from Insulet (unrelated to this study) and has investigator-initiated research support from Tandem Diabetes Inc., Dexcom, Digostics, and Medtronic. The other authors have nothing to disclose. The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
This study was funded by the CFF Harry Shwachman Clinical Investigator Award and Cystic Fibrosis Foundation EnVision CF Program. B.E.M. is supported by the National Institutes of Health (PI: B.E.M., NIH: K23DK129827).