
Abstract
Gestational diabetes mellitus (GDM) complicates 5%–25% of pregnancies worldwide and is the most prevalent metabolic complication of pregnancy. Risk factors for GDM include maternal obesity, advanced maternal age, family history of type 2 diabetes mellitus (T2DM), diagnosis of Polycystic ovarian syndrome (PCOS), and a prior history of GDM. GDM has both implications for the pregnant person and the offspring with increased risks of adverse pregnancy outcomes as well as increased chance of developing T2DM later in life. The first-line treatment for GDM includes behavior modification followed by pharmacologic therapy with insulin being preferred medication of choice. Standard of care for the management of continuous glucose monitors (CGM) currently includes self-monitored blood glucoses or finger sticks 4× per day and this can increase stress and anxiety in pregnancies. Continuous glucose monitorings have been used commonly in nonpregnant diabetic patients and patients with type 1 diabetes but their use in patients with GDM are increasing. Although there are no specific Continuous glucose monitoring targets for patients with GDM, CGMs have been used to help determine normative data in patients without GDM, which has helped provide expert opinion on GDM targets. In research studies, CGMs have also been used to explore glycemic profiles for patients early in pregnancy who go on to develop GDM as well as looking at adverse pregnancy outcomes in patients with higher Continuous glucose monitoring metrics. Using CGMs has the potential to provide more information about glycemia, ultimately leading to treatment recommendations in patients with GDM with the ultimate goal to improve adverse pregnancy outcomes and improve health and well-being at large.
Keywords
Introduction
Gestational diabetes mellitus (GDM) is the most common metabolic complication of pregnancy and has implications for both the pregnant person and their offspring. This review aims to summarize implications of GDM on the pregnant person and their offspring, review diagnosis, and discuss current standards of care regarding management of GDM as set by professional societies including the American College of Obstetricians and Gynecologists (ACOG) as well as the American Diabetes Association (ADA). We also discuss the use of continuous glucose monitors (CGM) as a new management strategy in pregnancies affected by GDM. In understanding the role of CGMs, we highlight literature demonstrating the use of CGM in determining normative data for pregnancies unaffected by GDM and discuss CGM patterns associated with pregnancies affected by GDM and perinatal complications.
Gestational Diabetes
Epidemiology
GDM complicates 5%–25% of pregnancies worldwide and is the most prevalent metabolic complication of pregnancy. Risk factors for GDM include maternal obesity, advanced maternal age, family history of type 2 diabetes, a diagnosis of polycystic ovarian syndrome, and a prior history of GDM. GDM has implications for both the pregnant person and the neonate. Pregnant patients are at increased risk for cesarean delivery, preeclampsia, and higher order perineal lacerations in pregnancy. 1 In addition, up to 70% of pregnant patients with gestational diabetes will develop type 2 diabetes later in life. 2 Neonates are at risk for fetal overgrowth including large for gestational age (LGA) and macrosomia, neonatal hypoglycemia, hyperbilirubinemia, and shoulder dystocia. 1 Similar to pregnant patients, the risks of diabetes in pregnancy extend beyond the immediate neonatal period. Infants born LGA are at risk for developing obesity, diabetes, and cardiovascular disease later in life. 3 Perinatal risks are lessened with improved glycemic control.
Similar to pregestational diabetes, GDM disproportionately affects patients of color. 4 In a retrospective study evaluating the rate of adverse pregnancy outcomes by race, Black pregnant patients with GDM were at increased risk of having cesarean delivery, hypertensive disorders of pregnancy, maternal Intensive care unit (ICU) admission, transfusion, small for gestational age infant, preterm birth at less than 37 weeks, and Neonatal Intensive Care Unit (NICU) admission compared with White counterparts with GDM. 5 The reason for disparities is likely multifactorial; however, an important potential contributing factor is systemic racism, which includes racial biases, differences in power structures, and institutional policies resulting in differences in access to safe housing, healthy food, financial resources, that may limit access to quality healthcare and resources. These differences in social determinants of health can impact glycemic control and in turn affect increase rates of adverse pregnancy outcomes. 5
Diagnosis
According to the ACOG and the ADA, the current standard of care for GDM includes self-monitoring of blood glucose (SMBG) by finger stick both fasting and postprandial 1 or 2 h after the start of the meal.1,6 Targeting treatment guidelines to postprandial blood glucoses has been associated with better glycemic outcomes and lower rates of preeclampsia.
6
Current recommended targets for individuals diagnosed with GDM are the same for those individuals with pre-existing diabetes (type 1 and type 2) in pregnancy as follows:1,6
Fasting glucose 70–95 mg/dL (3.9–5.3 mmol/L) and either: One-hour postprandial glucose 110–140 mg/dL (6.1–7.8 mmol/L) or Two-hour postprandial glucose 100–120 mg/dL (5.6–6.7 mmol/L)
Management
In pregnancy, there are various strategies for partnering with patients to manage their finger stick blood glucoses. Some institutions rely on traditional in person appointments at a planned frequency to review blood glucoses in addition to providing routine prenatal care. Other clinical programs have adopted a remote monitoring practice for diabetes management that does not increase the number of in person visits and is conducted remotely through different mechanisms such as secure email or messaging through the electronic medical record. A meta-analysis performed by Yue et al. assessed differences in glycemic control in participants with GDM who were enrolled in remote monitoring versus standard care groups. In this meta-analysis, 11 RCTs were included with over 1000 participants from 9 countries. 7 There was no significant differences in glycemic control nor maternal or fetal outcomes between the groups. 7 With the increased demands of GDM surveillance, remote monitoring is a potential strategy to help alleviate the burden without compromising maternal, fetal, or glycemic outcomes.
First-line therapy for GDM is lifestyle modification including dietary management and physical activity; however, approximately 30%–50% of individuals will need medication to achieve recommended glucose targets.1,6 Individuals with diet and exercise controlled GDM are classified as GDMA1, whereas those who require medication management are classified as GDMA2. In individuals with GDMA2, insulin is the preferred pharmacologic agent as it does not cross the placenta and has been studied extensively.1,6 For patients who are unable or unwilling to inject insulin or with limited access to insulin, metformin may be used as an alternative therapy in pregnancy. Metformin has been associated with lower rates of neonatal hypoglycemia and lower maternal weight gain.6,8 Unlike insulin, metformin readily crosses the placenta and long-term outcomes of neonatal metformin exposure are still being explored.
Fetal assessment is an important part of antenatal management. Ultrasound estimation of fetal size is recommended at least once in the third trimester but may be performed more frequently based on clinical factors. Antenatal fetal testing, either with nonstress tests or biophysical profiles, is usually recommended to start at 32 weeks in patients with suboptimal glycemic control or those with GDM requiring medication. In those who do not require medication, recommendations for antenatal fetal testing vary based on the provider and/or clinical guidelines of the health system. Antenatal surveillance recommendations may also be influenced by other maternal clinical characteristics such as advanced maternal age, obesity, hypertension as well as fetal overgrowth or polyhydramnios.
Delivery recommendations for individuals with GDM are often based on glycemic control and the presence of any additional complications such as fetal overgrowth and/or gestational hypertension. 1 Individuals with well controlled glucose levels are often expectantly managed until full term. Intrapartum, it is important to maintain appropriate glucose levels as maternal hyperglycemia can increase the risk of neonatal hypoglycemia. Although it is generally thought to maintain maternal blood glucose between 70–110 mg/dL (3.9–6.1 mmol/L) or 120 mg/dL (6.7 mmol/L), some studies have shown that controlled glucose levels intrapartum do not decrease the rates of neonatal hypoglycemia.9,10 A single-center randomized control trial of pregnant patients with GDM who were randomized to “tight control” defined as intrapartum blood glucoses of 70–100 mg/dL (3.9–5.6 mmol/L), or “liberalized control” defined as intrapartum blood glucoses of 70–120 mg/dL (3.9–6.7 mmol/L), showed no difference in the primary outcome of first measured neonatal blood glucose after birth. 9 Similarly, in another single center equivalence randomized trial of 96 pregnant patients with a mixed population of gestational and pregestational diabetes, there was no difference in first neonatal blood glucose within 2 hours after birth for the standard intrapartum blood glucose 70–110 mg/dL (3.9–6.1 mmol/L) group versus the permissive intrapartum blood glucose 70–180 mg/dL (3.9–10 mmol/L) group. 10 Larger clinical trials are warranted prior to liberalizing glucose control intrapartum.
Postpartum screening
Although GDM often resolves after delivery, up to one-third of affected individuals will have impaired glucose tolerance or diabetes at postpartum screening. 1 It is believed that 15%–70% of patients with GDM will develop diabetes at some point later in life. 2 Current screening recommendations include performing a fasting glucose test and the 75-g, 2 h oral glucose tolerance testing (OGTT) between 4 and 12 weeks postpartum.1,6 With the demands of the postpartum period, adherence rates to the recommended postpartum screening remain low. Recent literature has shown similar diagnostic value between the traditional 2-h postpartum screening between 4–12 weeks compared with performing postpartum screening within 2 days postpartum. 11 In a retrospective study from this same group looking at real-life implementation of the immediate postpartum 2-h GTT, there were higher rates of impaired glucose tolerance and overt diabetes in the immediate postpartum 2-h GTT cohort compared with the clinical trial. 12 It is unclear whether these higher rates persist when follow-up testing is performed at a time further from pregnancy. Given the overall promising data with immediate postpartum glucose screening compared with traditional screening, ACOG is in support of offering immediate postpartum glucose screening to assess for type 2 diabetes. 13
The Role of CGMs in GDM
CGMs are increasing in popularity in pregnant individuals with diabetes. CGM provides real-time information about interstitial blood glucose levels throughout the entire day, including nocturnal glucose, which is uncaptured by SMBG, which can facilitate diabetes self-management. 14 CGM also provides detailed data on glycemic response to food choices and activity levels and may overcome some of the challenges to suboptimal adherence compared with four times per day SMBG via finger sticks.15–18
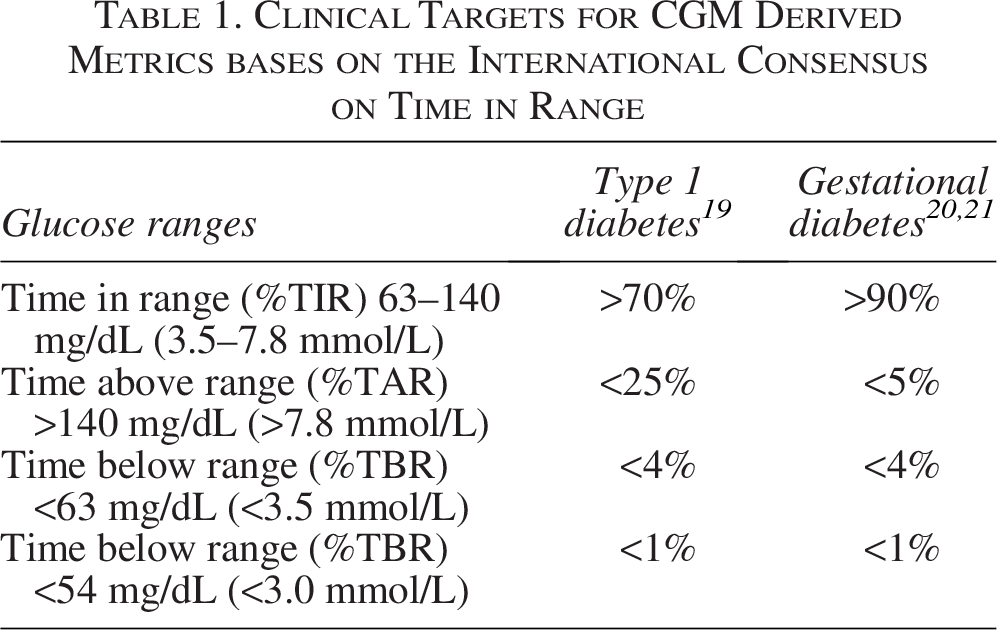
The CONCEPTT trial 19 is the seminal study evaluating the use of continuous glucose monitoring in pregnancy for patients with type 1 diabetes. The CONCEPTT trial was a randomized control trial of real-time continuous glucose monitoring in addition to standard care for pregnant patients with type 1 diabetes. 19 Although the study showed a slight statistical reduction in maternal hemoglobin A1C and a significant improvement in “time in range” (TIR) in type 1 individuals using CGM compared to SMBG with finger stick, the greatest benefit was seen in the reductions in LGA neonates, decreased length of hospital stays, and reductions in severe neonatal hypoglycemia 19 with a number needed to treat of 6 for LGA infants and NICU admissions and a number needed to treat of 8 for neonatal hypoglycemia. After the completion of this trial, clinical targets for CGM data interpretation were adopted for type 1 diabetes in pregnancy by the International Consensus on Time in Range, which currently are the only evidence-based targets for CGM management of diabetes in pregnancy (Table 1). 20 Randomized clinical trials for type 2 diabetes and GDM in pregnancy are currently underway in both the United States and the United Kingdom. Until these data become available, we must rely on expert opinion to guide clinical management in these individuals.
Normative data
In order to more effectively implement CGM technology for milder forms of metabolic dysfunction, such as GDM, it is important to understand glucose trends and patterns in individuals without a diagnosis of GDM. In a prospective, observational study, CGM-derived metrics were obtained in 413 uncomplicated pregnancies defined as those without a diagnosis of a hypertensive disorder of pregnancy, GDM, or delivery of an LGA infant. 21 In these individuals, the mean glucose was 98 ± 7 mg/dL (5.4 ± 0.4 mmol/L) throughout the entire gestational period and stable across all three trimesters as follows: first trimester 103 ± 7 mg/dL (5.7 ± 0.4 mmol/L), second trimester 98 ± 7 mg/dL (5.4 ± 0.4 mmol/L), and third trimester 98 ± 8 mg/dL (5.4 ± 0.4 mmol/L), respectively. Median percent TIR using currently accepted pregnancy targets of 63–140 mg/dL (3.5–7.8 mmol/L) was 94% and using a tighter TIR of 63–120 mg/dL (3.5–6/7 mmol/L) was 86%. Of the 413 participants included for analysis in this study, 157 of them voluntarily recorded mealtimes to provide information on postprandial glycemia. 23 Mean peak postprandial glucose was 126 ± 22 mg/dL (7.0 ± 1.2 mmol/L) and the median time to peak postprandial glucose was 62 min [IQR 40–124 min]. 21 These data provide important information regarding CGM-derived glycemic metrics in pregnant individuals without a diagnosis of GDM and may provide the framework to begin to develop GDM-specific CGM targets for pregnancy.
CGM-derived patterns associated with GDM diagnosis
Using a CGM in the second trimester of pregnancy, prior to standard OGTT, has also been shown to identify individuals who are diagnosed with GDM later in pregnancy using standardized testing via an OGTT later. In a prospective, observational study conducted at two academic-based clinical sites, 768 participants wore a blinded CGM as continuously as possible throughout their pregnancy with the primary objective to compare CGM-derived glycemic patterns between participants with GDM diagnosed via OGTT compared with those without. 22 Participants diagnosed with GDM were found to have higher mean glucose, lower TIR 63–140 mg/dL (3.5–7.8 mmol/L) and spent more time above range, both >120 mg/dL (6.7 mmol/L) and >140 mg/dL (7.8 mmol/L), during the gestational period prior to the OGTT than those who were not diagnosed with GDM (Table 2). In evaluating percent time spent above 140 mg/dL (7.8 mmol/L), those that developed GDM had higher mean glucose and percent time >140 mg/dL (7.8 mmol/L) as early as 13–14 weeks gestation and remained consistently higher at all 2-week intervals until the OGTT (Fig. 1). 22
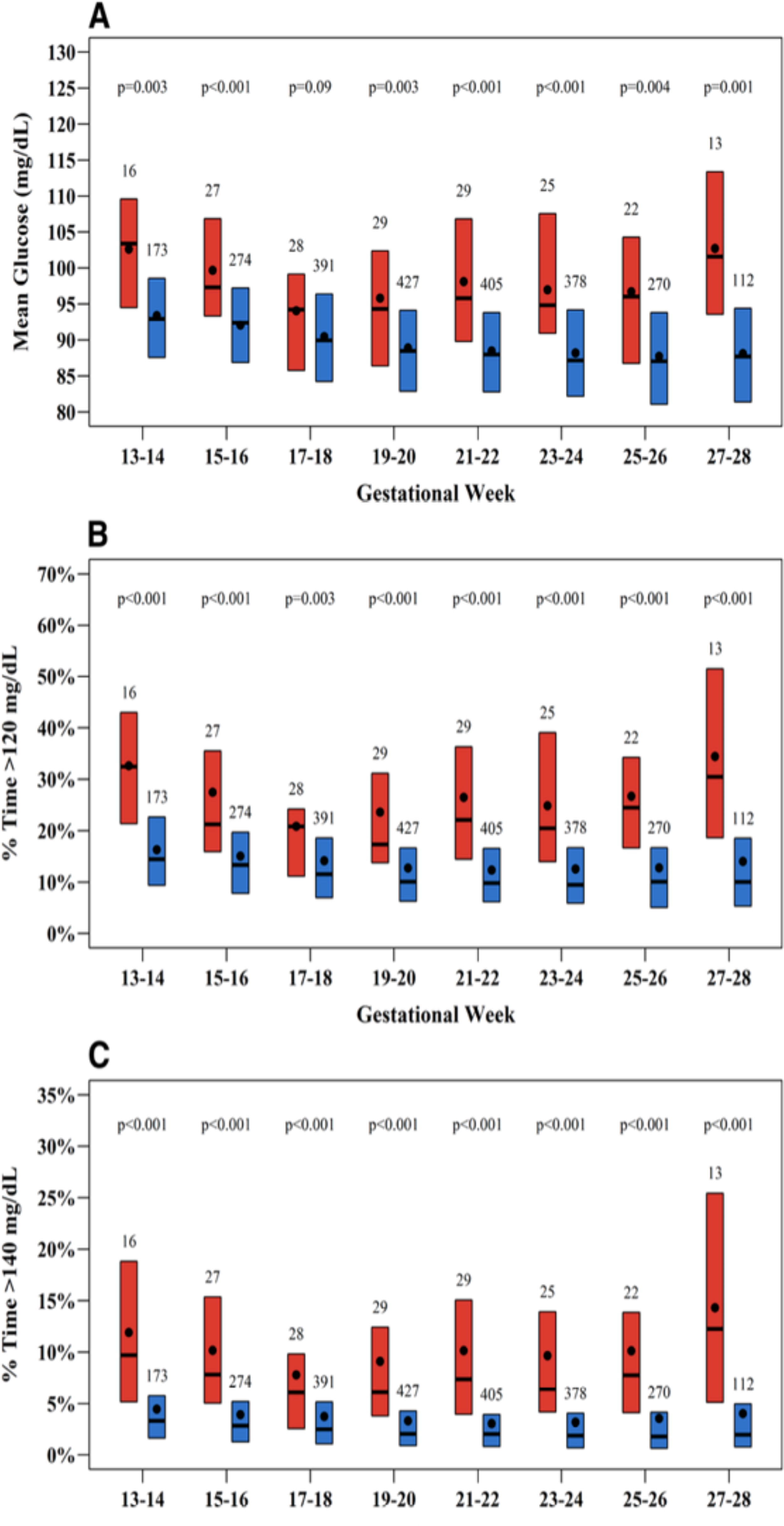
Boxplots of glycemic metrics of pregnancies with versus without GDM by 2-week period. Boxplots of

Entire gestational period before oral glucose tolerance test.
OGTT, oral glucose tolerance test; CGM, continuous glucose monitors; GDM, gestational diabetes mellitus.
In another prospective observational study, Fishel Bartal and colleagues sought to describe glycemic profiles wearing a blinded CGM starting at the time of oral glucose tolerance. The primary composite neonatal outcome, including LGA infant, shoulder dystocia, respiratory distress, and hypoglycemia requiring intravenous treatment, was higher in the cohort of patients who had time above range >140 mg/dL (7.8 mmol/L) of 10% or greater than those with time above range <10% (47% vs. 14.5%, P = 0.009), respectively. 25 Notably, GDM was only diagnosed in two patients based on the standard two-step criteria, suggesting that patients with hyperglycemia below the standard thresholds for diagnosis of GDM are still at risk for adverse neonatal outcomes. 23
CGM-derived patterns associated with perinatal outcomes
When evaluating CGM trends in a low-risk population of 760 pregnant individuals with singleton pregnancies and initial hemoglobin A1c <6.5%, those who developed a hypertensive disorder of pregnancy or delivered an LGA infant had higher mean glucose levels (103 ± 8 vs. 99 ± 8; P < 0.001 and 102 ± 9 vs. 100 ± 8; P = 0.01) and spent more time above both 120 mg/dL (6.7 mmol/L) (median 16% vs. 12%; P < 0.01 and 16% vs. 12%; P = 0.006) throughout gestation compared with those who without these outcomes 24 (Fig. 2). These findings highlight that the association between glucose levels and perinatal outcomes likely represent a continuous association rather than dichotomous cut-offs. Furthermore, the glucose levels associated with perinatal complications are likely below current diagnostic or treatment thresholds for GDM similar to the findings of the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study. 27 These findings highlight the potential advantages in using CGM for glucose management compared with SMBG via finger stick because CGM allows for continuous assessment of glucose data throughout the entirety of the day. It also may identify potential targets for treatment that were previously unrecognized with four times per day finger stick testing, which left large gaps of time without any glucose data. 26
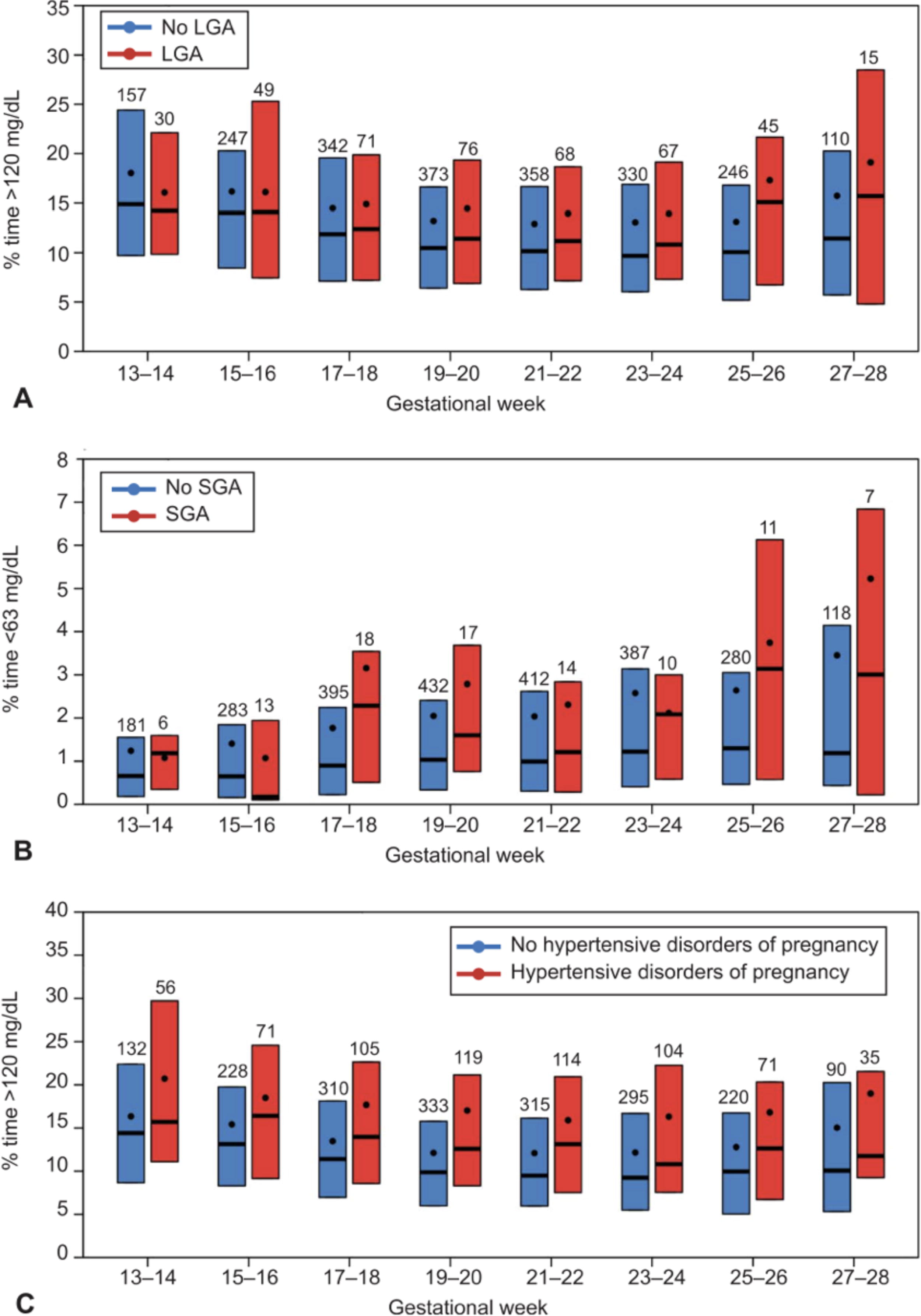
Boxplots of glycemic metrics of pregnancies with versus without fetal growth disturbance and hypertensive disorders of pregnancy. Boxplots of
In a small retrospective study evaluating the use of CGM intrapartum of 98 patients with type 2 diabetes, McCarley et al. found that rates of neonatal hypoglycemia were similar in groups that had that a TIR <70% and TIR >70% for 6 h predelivery using recommended glucose targets of 65–110 mg/dL (3.6–6.1 mmol/L). 27 In the authors’ sensitivity analysis, TIR >70% 2 h prior to delivery was associated with lower odds of hypoglycemia (36.8% vs. 60.0%, amor 0.38, 95% CI: 0.16–0.88). Similarly, rates of hypoglycemia treatment and initial neonatal glucose <40 mg/dL (2.2 mmol/L) were lower in the group with TIR >70% 2 h prior to delivery. 27 While there is still debate whether tight maternal glucose control intrapartum helps to reduce the risk of neonatal hypoglycemia, this study highlights the potential utility of intrapartum CGM to effectively provide information regarding maternal glycemia and potentially decrease neonatal complications.
CGM for management of GDM
There are limited data on the utilization of CGM for glucose management after a diagnosis of GDM including no evidence-based targets for treatment. Current recommendations for clinical targets for the treatment of patients with GDM are based on expert opinion,26,28 emphasizing stricter glycemic control due to the lower likelihood of hypoglycemia compared with patients with type 1 diabetes and emerging normative data in pregnant individuals without a diagnosis of diabetes. Based on expert opinion, it is proposed that the treatment goal for TIR for patients with GDM is around 90% (Table 1). The percent time below range has not been defined for individuals with GDM. The time below range targets may not apply to individuals with diet controlled GDM (GDMA1) without hypoglycemic symptoms because levels below 63 mg/dL (3.5 mmol/L) may represent normal physiology of pregnancy especially overnight or during periods of fasting.
The majority of studies published evaluating CGM use in GDM populations are limited by small sample size, different diagnostic criteria for GDM, different CGM systems, older generation of sensors than currently in use, and limited sensor wear (72 h to 4 weeks). In a recent systematic review of 14 studies (prospective observational cohorts and randomized clinical trials) evaluating the efficacy of CGM for maternal glycemic control, CGM use was associated with a higher detection of both hyperglycemia and nocturnal hypoglycemia compared with SMBG. 29 Nearly all the studies included demonstrate that CGM was superior to SMBG in predicting the need for pharmacologic therapy and the ability to adjust medication doses as needed. In a separate meta-analysis of five small randomized clinical trials, the association between CGM and select maternal and neonatal outcomes were analyzed. The use of CGM was associated with lower HbA1c at the end of pregnancy but no difference in mean fasting or postprandial glucose; less gestational weight gain; and lower infant birth weight but no difference in rates of LGA infant or macrosomia (birth weight > 4000 g). 30
In a mixed population of pregnant individuals with type 2 diabetes and GDM utilizing CGM for management, the association between perinatal outcomes and TIR was explored. In this retrospective study of 65 individuals (53 with type 2 and 12 with GDM), those who spent ≤70% TIR 63–140 mg/dL (3.5–7.8 mmol/L) had a 4.8-fold higher rate of a composite neonatal morbidity (LGA, NICU admission, need for IV glucose, respiratory support, neonatal death) compared with those who achieved >70% time above range (71.4% vs. 37.8%, P = 0.02). 31 Similarly, rates of hypertensive disorders of pregnancy, preterm birth, and cesarean delivery were also higher in those individuals who spent ≤70% TIR 63–140 mg/dL (3.5–7.8 mmol/L).
Larger clinical trials are needed to better understand the role of CGM in the GDM population, including appropriate clinical targets for TIR, time above range, and mean glucose as well as the influence of CGM metrics on perinatal outcomes associated with maternal metabolism such as hypertensive disorders of pregnancy, fetal overgrowth and neonatal outcomes such as respiratory distress syndrome, hyperbilirubinemia, and hypoglycemia.
CGM as a prediction tool for GDM
Exploration into using CGM to predict GDM is also an area of active research. Li et al. used predictive models to assess various CGM-derived metrics in identifying individuals who were diagnosed with GDM by OGTT. The authors found % time above range greater than 140 mg/dL (7.8 mmol/L) performed best with an Area Under the Receiver Operating Characteristic curve (AUROC) of 0.84. This signal could be detected as early as 13–14 weeks gestation. 32 The addition of other CGM metrics did not improve the predictive ability of the model. In this cohort, CGM metrics performed better than clinical characteristics such as body mass index (BMI) and initial hemoglobin A1c. Similarly, in a cohort of Southeast Asian pregnant patients, using a combination of CGM metrics including % glucose variability, glucose management index, continuous overlapping net glycemic action, and mean amplitude of glycemic excursions, was more predictive at diagnosing GDM compared with traditional methods such as maternal age, ethnicity, BMI, and blood pressure. 33 Further investigation is needed to determine the role of CGM in detection of early pregnancy hyperglycemia and potential interventions that may mitigate risks associated with altered glucose metabolism.
Practical approaches to use of CGM in GDM
The use of CGM also has benefits outside of assisting with therapy choices with research indicating behavior modifications in patients who wear CGMs. 26 Through the ability to see real-time glycemic information, patients are directly able to see the effect of exercise and food choices on glycemia. 26 This allows patients to make informed decisions regarding dietary choices and exercise. A review of the literature by Ehrhardt and Zaghal reported on small studies that demonstrated increased physical activity, decreased intake of high glycemic foods, and decreased BMI in nonpregnant patients with type 2 diabetes. 34 Although pregnant patients were not included in these studies, it is likely that CGM can have similar effects on physical activity and dietary choices for patients with GDM. Furthermore, CGMs can reduce stress and anxiety that are often accompanied with frequent finger sticks. 26 The ease of using CGMs compared with finger sticks cannot be understated as SMBG via finger sticks is disruptive to daily activities and requires supplies to be with the person. Given the disruption, many patients have expressed difficulty with the compliance of the finger stick and CGM can be useful in easing the burden. 26
In summary, GDM is one of the most prevalent perinatal complications and is the most common type of diabetes in pregnancy. With increasing maternal age, BMI, and other maternal factors, the rates of GDM are likely to continue to increase. Patients with GDM represent a heterogenous group of individuals with metabolic dysfunction with treatment that ranges from dietary management alone to multidose insulin therapy. Based on current guidelines, it requires patients to make dietary changes, perform SMBG via finger sticks, which can increase stress and anxiety in pregnancy. 17 The first-line treatment for patients with GDM is behavioral modification with dietary modifications and increased physical activity, followed by pharmacologic therapy. CGM has been used commonly in nonpregnant diabetes populations and pregnant patients with type 1 diabetes; however, its use is expanding in the GDM population. With use of CGM, there is potential for improved satisfaction and improved compliance. Given the direct observation of behaviors and/or medications on glycemia, CGM has the potential to increase patient comfort with recommendations from their providers. 26 Improving the health of these individuals may improve overall health and well-being with the potential to lead to healthy lifestyle behaviors that can delay progression to type 2 diabetes.