
Abstract
In this study, we aimed to explore the impact of meal carbohydrate (CHO) content on postprandial hyperglycemia in hospitalized patients receiving fully automated insulin delivery (AID). We performed a post-hoc analysis of two trials and analyzed 844 postprandial periods from 48 adults treated with fully AID (FlorenceD2W-T2 or CamAPS HX) in hospital using generalized additive regression models. Meal CHO content had a nonlinear effect on postprandial hyperglycemia risk (P < 0.001). Postprandial hyperglycemia was more likely at breakfast compared with lunch and dinner (odds ratio or OR [95% confidence interval or CI] 1.8 [1.2, 2.6], P = 0.006; and 1.5 [1.1, 2.2], P = 0.05, respectively) and more frequent on days with glucocorticoid administration (OR [95% CI] 3.3 [2.1, 5.1]; P < 0.001). In conclusion, during fully AID in hospitalized patients, the risk of postprandial hyperglycemia remained <50% for meals ≤50 g CHO. The CHO tolerance was lowest at breakfast and with concomitant glucocorticoid therapy across all meals.
Keywords
Introduction
Fully automated insulin delivery (AID) systems simplify diabetes management by eliminating manual bolus administration, which is particularly valuable in resource-constrained hospitals.1,2 However, this may increase the risk of postprandial hyperglycemia.3,4 This post-hoc analysis examines the meal carbohydrate (CHO) content effect on the risk of postprandial hyperglycemia during fully AID in hospital. Additionally, it explores how meal timing, glucocorticoid use, and other clinical factors modify this effect. These investigations aim to optimize fully AID implementation in hospitals by identifying critical determinants of postprandial glucose excursions.
Methods
Design
We performed a post-hoc analysis using pooled data from two open-label, randomized controlled trials (NCT01774565, NCT05392452) evaluating the glycemic efficacy of fully AID in hospitalized patients.5,6
The study populations comprised noncritical care adults with insulin-requiring hyperglycemia (excluding patients with type 1 diabetes) who received ≥72 h of fully AID therapy at the University Hospital Bern, Switzerland. Fully AID was enabled using the Cambridge model predictive control algorithm implemented on a smartphone or tablet platform, which directed subcutaneous insulin infusion (rapid-acting or faster-acting aspart) based on continuous glucose monitoring. The system was initialized using each participant’s body weight and estimated total daily insulin dose, with a default glucose target of 5.8 mmol/L. As meals were unannounced, no manual boluses were given. The Bern Ethics Committee approved study protocols (2017-00321, 2022-D0034) and participants provided written informed consent.
Meal data collection
Meal macronutrient composition (CHO, fat, protein) was recorded using the hospital’s electronic meal management software (LogiMen® Station, LOGIMATIKA GmbH, Leonberg, Germany). The software tracked meal orders and detailed macronutrient content (g) for each meal’s components. Research staff or nursing personnel recorded the consumed percentage (0/25/50/75/100%) per component, allowing calculation of ingested macronutrients at the meal level. Meal timing was documented with electronic case report forms.
Definition of postprandial period and data preprocessing
We assessed a 180-min postprandial period following meal initiation, defining postprandial hyperglycemia as sensor glucose levels ≥10.0 mmol/L for ≥60 min, in line with continuous glucose monitoring (CGM) standards and the inpatient guidelines for noncritically ill patients.7–9 CGM gaps ≤60 min were imputed using linear interpolation, while longer gaps were not. Not fully imputed postprandial periods were still considered if a continuous period of >60 min with valid data occurred within the 180-min window. Postprandial CGM outcomes were quantified for each postprandial period and summarized as mean values per participant. Preprandial glucose was defined as the most recent CGM value within 15 min before the meal.
Insulin on board was calculated using a pharmacokinetic model 10 incorporating administration time, dose, and duration of action. Glucocorticoid exposure was considered per day and not specific to postprandial periods.
Statistical analysis
To examine the effect of meal CHO content on the risk of postprandial hyperglycemia, a generalized additive logistic regression model was used. A directed acyclic graph (DAG) (DAGitty software, version 3.1., https://www.dagitty.net/dags.html#, R package “dagitty”) 11 guided covariate selection for causal inference, identifying the minimally sufficient adjustment set to block confounding backdoor paths. To improve precision, we adjusted for variables that influence postprandial hyperglycemia but not meal CHO content. Meal energy content in kilocalories was not observed. The DAG is shown in Supplementary Figure S1. The regression model included smooth terms for meal CHO content to capture possible nonlinear effects of CHO intake on postprandial hyperglycemia and was adjusted for meal timing (breakfast, lunch, dinner), fat and protein content, preprandial glucose level, insulin on board, and participant characteristics (age, sex, body mass index [BMI], HbA1c, glucocorticoid use). Random effect for participant was included to account for repeated observations in one subject. Postprandial hyperglycemia risk was compared by meal timing (breakfast/lunch/dinner) and glucocorticoid use in a secondary model. Meal timing, glucocorticoid exposure, and participant characteristics were included as fixed effects (Supplementary Figs. S2 and Figs. S3). In this second model, preprandial glucose and insulin on board were excluded (per DAG) as meal timing inherently affects them via prior meals, insulin dosing, and circadian influences. Adjusting for these variables could distort meal-based comparisons by removing differences in premeal glycemic conditions related to meal timing. Similarly, for the glucocorticoid analysis, these variables were omitted because glucocorticoids may influence both preprandial glucose and insulin requirements. The models’ formulas are displayed in Supplementary Table S3. To assess the robustness of our findings, we conducted a sensitivity analysis using generalized additive mixed models, with the percentage of postprandial time above 10 mmol/L as the continuous outcome. These models included the same covariates as the primary analyses.
For categorical variables with more than two levels (e.g., meal timing), overall effects were evaluated using Wald chi-square tests. Significant effects were followed by Tukey–Kramer-adjusted pairwise comparisons of marginal means.
Descriptive statistics are presented as mean ± standard deviation for normally distributed and median (25th, 75th percentile) for nonnormally distributed variables (normality assessed using the Shapiro–Wilks test). We show the model-predicted probability of postprandial hyperglycemia (mean and 95% confidence interval [CI]) as a function of CHO intake stratified by glucocorticoids use for an average patient (majority label for categorical variables, mean for continuous ones). Other estimation results are reported as odds ratios (ORs) with 95% CIs and P-values. All analyses were performed using R (software version 4.1.0). Generalized additive models were estimated using the mgcv package. 12 Estimated marginal means and pairwise comparisons were calculated using the emmeans package. 13
Results
Clinical context
The analysis included 844 postprandial periods from 48 patients. Patient characteristics are reported in Table 1. Mean age was 70 ± 10 years, BMI was 31 ± 7 kg/m2, and 9 (19%) patients were female. At admission, all patients had type 2 diabetes except one with pancreatic diabetes and one with prediabetes scheduled for total pancreatectomy. HbA1c at admission was 7.8 ± 1.0% (63 ± 19 mmol/mol) and total daily insulin use during fully AID was 34 (25, 50) IU/d. The number of patients admitted for surgery was 8 (17%), of which three underwent total pancreatectomy.
Patient Characteristics
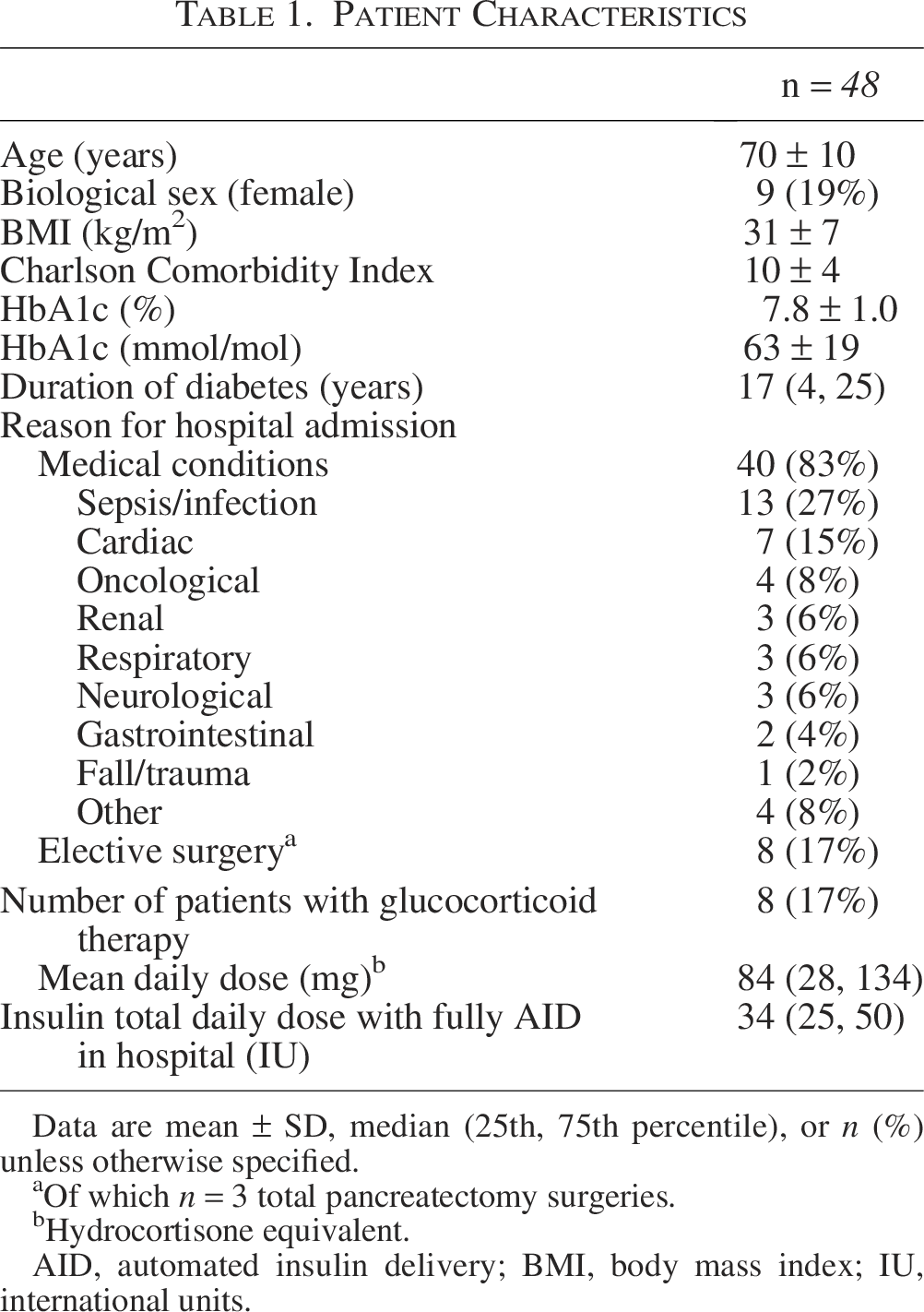
Data are mean ± SD, median (25th, 75th percentile), or n (%) unless otherwise specified.
Of which n = 3 total pancreatectomy surgeries.
Hydrocortisone equivalent.
AID, automated insulin delivery; BMI, body mass index; IU, international units.
The CHO content of meals was 61 (46, 73) g for breakfast, 49 (37, 64) g for lunch, and 53 (36, 76) g for dinner. The frequency distribution of meal macronutrient content is illustrated in Supplementary Figure S4.
Glucose control
Postprandial glucose and insulin metrics are presented in Supplementary Table S1. The percentage of time spent with CGM values between 3.9 and 10.0 mmol/L was 75 (62, 87)%. Postprandial time above 10.0 mmol/L was 24 (13, 38)%. There were 281 (33%) postprandial events with sensor glucose ≥10 mmol/L lasting ≥60 min, with mean event duration of 109 ± 22 min. The mean postprandial sensor glucose was 8.4 (8.0, 9.1) mmol/L. The median postprandial insulin dose was 6.6 (4.2, 8.5) IU, of which 25 ± 8% was infused during the first hour, 42 (34, 44)% during the second hour, and 35 ± 8% during the third postprandial hour. Glucose metrics calculated over the entire duration of fully AID therapy are provided in Supplementary Table S2.
Impact of meal macronutrient composition on postprandial hyperglycemia risk
We observed a dose-dependent effect of meal CHO content on postprandial hyperglycemia risk (P < 0.001). Hyperglycemia risk increased markedly with carbohydrate intake (0–75 g; Fig. 1). Beyond 75 g, hyperglycemia risk rose minimally. Higher preprandial glucose increased postprandial hyperglycemia risk (OR 1.8, CI [1.6, 2.1], P < 0.001).
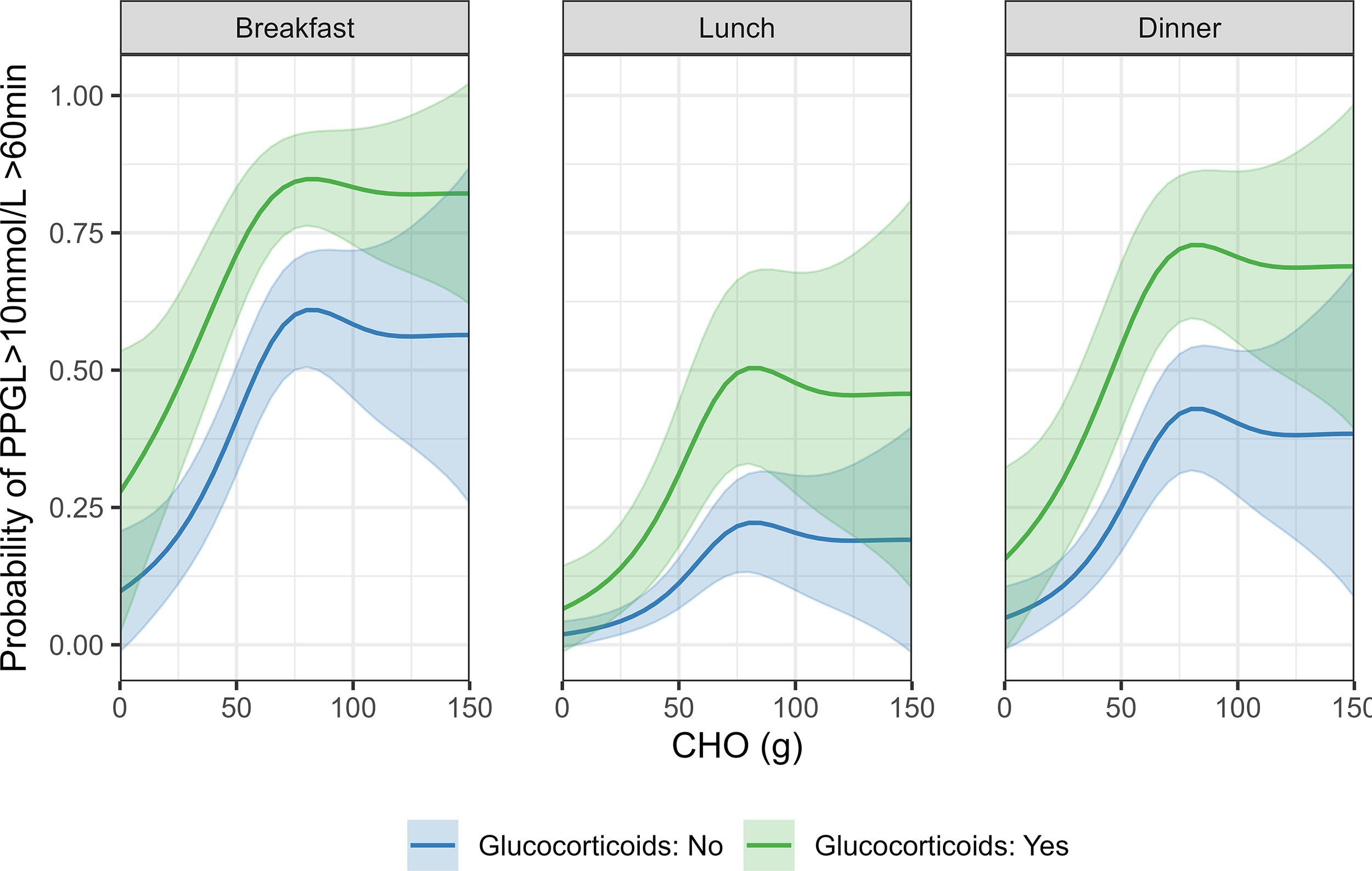
The effect of meal carbohydrate content on probability of postprandial hyperglycemia, with and without glucocorticoid exposure. Bold lines represent the mean predicted values and ribbons the confidence intervals. CHO, carbohydrate; PPGL, postprandial glucose.
Association of meal timing and glucocorticoid therapy with postprandial hyperglycemia risk
The probability of postprandial hyperglycemia was higher following breakfast than lunch or dinner (OR 1.8, CI [1.2, 2.6], P = 0.005 and OR 1.5, CI [1.1, 2.2], P = 0.05, respectively), based on Tukey–Kramer-adjusted comparisons of marginal means differences. Glucocorticoid administration increased postprandial hyperglycemia likelihood (OR 3.3, CI [2.1, 5.1], P < 0.001).
We did not find strong evidence of an association of age, sex, HbA1c, and BMI with postprandial hyperglycemia. Detailed estimation results are provided in Supplementary Table S4.
Sensitivity analysis
In line with the primary analysis, meal CHO content had a nonlinear effect on the predicted postprandial time >10 mmol/L (effective degrees of freedom = 4.3, F-value = 11.1, P < 0.001). Glucocorticoid administration increased the predicted value of postprandial time >10 mmol/L (Estimate = 15.2%, CI [2.3, 28.0], P < 0.001). The predicted postprandial time >10 mmol/L was 4.6% higher after breakfast compared with lunch (95% CI [0.0, 9.3], P = 0.12) and 3.9% higher compared with dinner (95% CI [−0.7, 8.6], P = 0.22). Also, there were no strong associations of age, sex, HbA1c, and BMI with postprandial time >10 mmol/L. The detailed results of the sensitivity analysis are provided in Supplementary Table S5.
Discussion
In this study of hospitalized patients receiving fully AID, we demonstrated a nonlinear effect of meal CHO content on postprandial hyperglycemia, with reduced CHO tolerance at breakfast and during glucocorticoid therapy.
The risk of hyperglycemia increased sharply with CHO intake up to 75 g, plateauing thereafter, while meals containing less than 50 g of CHO were associated with a hyperglycemia risk of below 50%. Postprandial periods following breakfast showed the lowest CHO tolerance, likely attributable to both the prolonged “dawn phenomenon,” characterized by reduced hepatic insulin sensitivity upon awakening, common in diabetes,14–16 and lower preprandial insulin on board after an overnight fast, reducing the AID system’s capability to mitigate breakfast glucose peaks. These findings align with previous research showing reduced time-in-range (3.9–10.0 mmol/L) after breakfast (58%) compared with dinner (72%) in fully AID-treated patients. 3 Overall postprandial time-in-range was higher than in earlier studies (75% vs. 40.2%–51.2%). 17
Glucocorticoid therapy significantly reduced CHO tolerance across all meals, consistent with its known effects on glucose metabolism through decreased insulin sensitivity, increased hepatic gluconeogenesis, and attenuated endogenous insulin secretion.18–20 As expected, elevated premeal glucose levels inherently predisposed to higher postprandial hyperglycemia risk.
A sensitivity analysis, with the postprandial time above 10 mmol/L (%) as the outcome, validated the robustness of the data analysis by yielding consistent effects for CHO intake (significant nonlinear), glucocorticoids (significant), and meal timing (greater effect for breakfast than lunch or dinner). The results were primarily reported using a binary outcome (risk for postprandial hyperglycemia) to facilitate risk estimation and enhance clinical interpretability. This approach offered a more direct translation of findings into practical application, while not affecting the overall conclusions of the study. As a practical consideration, our findings recommend moderating meal CHO contents (<50 g/meal) with increased emphasis on high-quality fat and/or proteins, particularly for breakfast and glucocorticoid-treated patients receiving fully AID. Future technological solutions could address postprandial hyperglycemia without manual operations or CHO restrictions. Promising approaches include artificial intelligence-based meal detection systems coupled with automated insulin priming algorithms.21,22
We acknowledge limitations inherent to post-hoc analyses, missing information on carbohydrate quality, and a postprandial period that was too short to detect late postprandial effects of high-calorie meals; however, the choice of a 180-min period is a widely used standard to avoid overlap between meals. We further acknowledge limited generalizability to other AID systems or less structured meal and lifestyle settings. Notably, the cohort of studied patients represented predominantly elderly male patients with preserved insulin secretion, with only 6% having absolute insulin deficiency post-pancreatectomy. Finally, although we carefully specified our models to minimize confounding and strengthen the validity of our findings, the observational nature of the study precludes definitive conclusions about causality.
Conclusions
In conclusion, while fully AID systems effectively manage the challenge of unannounced hospital meals, breakfast timing and glucocorticoid therapy emerge as critical modulators of postprandial hyperglycemia risk. Given the increasing interest in expanding the use of diabetes technology in the hospital, addressing these limitations through nutritional strategies and technological innovations will be essential for optimizing fully AID implementation in hospital care.
Authors’ Contributions
L.B. and D.H. designed and coordinated the study. N.B. created the script for statistical data analysis. G.K., N.B., and D.H. contributed to data analysis, including statistical analyses. All authors contributed to the interpretation of the results, critically revised the article, and approved the final article. All authors made the decision to submit for publication. L.B. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Footnotes
Acknowledgments
The authors are grateful to all study participants for their contribution, time, and support. They acknowledge administrative support from Laura Cavalli and Nina Schorno, University Hospital Bern. They thank David Studer and the Clinical Research Nursing Assistants Sophie Brunner and Vera Zenklusen (University Hospital Bern) who contributed to patient care, study logistics, and data management.
Author Disclosure Statement
L.B. reports having received speaker and advisory board honoraria from Dexcom, Novo Nordisk, and Ypsomed. D.H. reports having received speaker honoraria from Ypsomed. For the remaining authors, no conflicts of interest were declared.
Funding Information
The authors acknowledge financial project support from the Swiss Foundation for Anaesthesiology & Intensive Care, Scherbarth, and Helmut Horten foundations. They also acknowledge the participants’ commitment in wearing devices. Dexcom Inc., USA, and Ypsomed, Switzerland, provided unrestricted product support.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.