
Abstract
Cyclin D1 (CCND1) is a key protein in regulation of cell cycle at the G1-to-S transition phase and is essential for regulation of cell proliferation, differentiation, and transcriptional control. We hypothesized that the CCND1 G870A polymorphism is associated with risk of bladder cancer. The CCND1 G870A polymorphism was genotyped in a hospital-based case–control study of 402 bladder cancer cases and 402 control subjects using the polymerase chain reaction–restriction fragment length polymorphism method. Unconditional univariate and multivariate logistic regression analyses were used to evaluate the associations between the CCND1 G870A polymorphism and bladder cancer risk. A significantly increased risk of bladder cancer was associated with the combined variant CCND1 870GA/AA genotypes (adjusted odds ratio, 1.54; 95% confidence interval, 1.08–2.20) compared with the GG genotype, particularly among subgroups of age ≥65 years (1.74; 1.06–2.88), men (1.67; 1.15–2.44), and smokers (1.82; 1.12–2.93). Further, the G870A polymorphism was significantly associated with risk of developing superficial bladder cancer (grade 1). In addition, a meta-analysis of the G870A polymorphism and bladder cancer risk showed that the variant 870GA/AA genotypes were associated with an increased risk of bladder cancer in Asians, but not in Caucasians, which was consistent with the results of our study. The CCND1 G870A polymorphism may be a marker for the development of bladder cancer in Chinese populations. Larger studies are required to validate these findings in diverse populations.
Introduction
Cyclin D1 (CCND1) is a key cell cycle regulatory protein, playing a critical role in the G1-to-S transition phase of the cell cycle progression (Stacey, 2003). Overexpression of CCND1 induces excessive cellular proliferation, one of the cancer features (Zhou et al., 1996). The CCND1 gene (also known as PRAD1/BCL1/U21B31/D11S287E) is located on chromosome 11q13, and amplification of this region is frequently detected in bladder carcinoma (Lee et al., 1997), suggesting that CCND1 may contribute to the etiology of bladder cancer.
As shown in the HapMap (
Several studies have been conducted to examine the associations between the CCND1 G870A polymorphism and bladder cancer risk (Wang et al., 2002; Cortessis et al., 2003; Ito et al., 2004; Sanyal et al., 2004; Ryk et al., 2006; Wu et al., 2006; Chung et al., 2008; Ye et al., 2008). However, the results remain conflicting rather than conclusive. To investigate the association between the CCND1 G870A polymorphism and bladder cancer risk, we genotyped this polymorphism in our ongoing hospital-based retrospective study of bladder cancer in a Chinese population and verified our findings in an additional meta-analysis of published studies.
Materials and Methods
Study subjects
The recruitment of subjects has been described previously (Wang et al., 2009). Briefly, 408 patients with newly diagnosed and histologically confirmed transitional cell carcinoma of bladder and 402 cancer-free control subjects were recruited from the First Affiliated Hospital and Huai-An Affiliated Hospital of Nanjing Medical University between January 2003 and February 2009. The patients who had previous cancer, metastases from other or unknown origins, or previous radiotherapy or chemotherapy were excluded. The cancer-free control subjects were recruited from those seeking health care in the outpatient departments at the same hospital. These control subjects had conditions other than cancer, such as ischemic heart diseases, cerebrovascular diseases, and chronic airway obstruction diseases. The response rate of eligible cases and control subjects was >85%. Only Han Chinese patients and control subjects were included in this analysis, because genotype frequencies can vary among ethnic groups. Demographic and tobacco smoking information was obtained through face-to-face interviews. Individuals who smoked once a day for >1 year were defined as smokers. Smokers who had quit smoking for >1 year were defined as former smokers, and the other smokers as current smokers. Pack-years [(cigarettes per day ÷ 20) × years smoked] were calculated to indicate the cumulative smoking dose. The research protocol was approved by the institutional review board of Nanjing Medical University.
Clinical data collection
Clinical information about the stage and grade of bladder cancer was provided by the urologists who followed the 2002 International Union Against Cancer (UICC) tumor-nodes-metastasis classification and the World Health Organization 1973 grading of urothelial papilloma: well differentiated (grade 1, G1), moderately differentiated (grade 1, G2), or poorly differentiated (grade 3, G3). Of the 402 total bladder cancer patients, 255 patients had superficial tumors (pTa-pT1), whereas the other 147 had invasive tumors (pT2-pT4). Among the patients, 163 were grade 1, 175 grade 2, and 64 grade 3. Having signed an informed consent, each participant donated 5 mL of blood, which was used for genomic DNA extraction.
Genotyping
The CCND1 G870A polymorphism was determined using the polymerase chain reaction–restriction fragment length polymorphism method (Betticher et al., 1995), and the primers, length, and restriction enzymes (Wang et al., 2002) have been previously described. The genotyping was performed by two persons independently and blindly. About >10% of the samples were randomly selected for confirmation, and the results were 100% concordant. However, six cases (1.5%), but no control subjects, failed in genotyping due to DNA quality or quantity, and these samples were excluded in further analyses. The final analysis included 402 cases and 402 frequency-matched control subjects.
Statistical analysis
χ 2-Test was used to evaluate the differences in frequency distributions of selected demographic variables, smoking status, and each allele and genotype of the CCND1 G870A polymorphism between the cases and control subjects. Hardy–Weinberg equilibrium of the control subjects' genotype distributions was tested by a goodness-of-fit χ 2-test. Unconditional univariate and multivariate logistic regression analyses were used to obtain the crude and adjusted odds ratios (ORs) and their 95% confidence intervals (95% CIs).
A meta-analysis was conducted to summarize our findings along with previously published studies on the association between the CCND1 G870A polymorphism and bladder cancer risk. Data searches and search strategy were conducted on two online electronic databases (PubMed and Embase) to select studies published before March 1, 2009, containing data for the CCND1 G870A polymorphism and bladder cancer risk with a case–control design. The search was limited to articles published in English, and additional studies were identified by a hand search of the references of original studies. Of the two studies with overlapping data published by the same investigators (Wu et al., 2006; Ye et al., 2008), we selected the most recent one with the larger number of subjects (Ye et al., 2008). Two studies without control subjects were excluded in the meta-analysis (Ito et al., 2004; Ryk et al., 2006).
We identified a total of six studies including 2228 cases and 2578 control subjects and estimated crude ORs and their 95% CIs for each genotype in each study. Values from single studies were combined using both fixed effect (Mantel–Haenszel) model. Egger's linear regression test was used to provide diagnosis of potential publication bias (Egger et al., 1997). All analyses were done with SAS (version 9.1; SAS Institute Inc., Cary, NC) and Stata software (version 8.2; StataCorp LP, College Station, TX) with two-sided p values.
Results
Characteristics of the study subjects
The frequency distributions of selected characteristics of the cases and control subjects are summarized in Table 1. No significant differences were identified between cases and control subjects with regard to age (cases vs. control subjects [mean ± standard deviation], 63.9 ± 13.0 vs. 62.9 ± 11.8; p = 0.262) and sex (p = 0.716). There were more smokers among the cases (54.2%) than among the control subjects (41.8%) (p < 0.001). Further analysis indicated that 25.3% of the cases smoked >20 pack-years, significantly higher than that of the control subjects (19.9%) (p = 0.002).
SD, standard deviation.
Association between the CCND1 G870A polymorphism and bladder cancer risk
The genotype and allele distributions of the CCND1 G870A polymorphism in the cases and control subjects are presented in Table 2. The observed genotype distributions of the G870A polymorphism was in agreement with Hardy–Weinberg equilibrium among the control subjects (p = 0.788). For the G870A polymorphism, the GG, GA, and AA genotype frequencies were 16.7%, 50.0%, and 33.3%, respectively, among the cases, and 23.4%, 49.3%, and 27.3%, respectively, among the control subjects (p = 0.032). Further, the 870A allele frequency was 0.583 for cases and 0.520 for control subjects, and the difference was also statistically significant (p = 0.011).
Two-sided χ 2-test.
Adjusted for age, sex, and pack-years smoked in a logistic regression model.
CCND1, cyclin D1; OR, odds ratio; CI, confidence interval.
Multivariate logistic regression analysis revealed that the ORs for cases carrying the GA and AA genotypes were 1.44 (95% CI, 0.98–2.10) and 1.71 (95% CI, 1.14–2.57), compared with the GG genotype, suggesting that the polymorphism acts in an allele dose-dependent manner (P trend = 0.012). Further, a significantly increased risk of bladder cancer was found in the combined variant GA/AA genotypes compared with the GG genotype (OR, 1.54; 95% CI, 1.08–2.20) (Table 2). Further stratification analysis showed that this increased risk was more pronounced among subgroups of age ≥65 years (1.74; 1.06–2.88), men (1.67; 1.15–2.44), and smokers (1.82; 1.12–2.93) (Table 3). However, we did not find any statistical evidence for gene–environment interactions in bladder cancer risk (data not shown).
Adjusted for age, sex, and pack-years smoked in a logistic regression model.
Association between the CCND1 G870A polymorphism and clinicopathologic characteristics of bladder cancer
We further examined the association between the CCND1 G870A polymorphism and clinicopathologic characteristics of bladder cancer. As shown in Table 4, a statistically significantly increased risk was associated with bladder cancer with grade 1 (1.81; 1.10–2.97), but not with grade 2 (1.42; 0.90–2.25) or grade 3 (1.45; 0.72–2.94), which is likely due to a limited study power of the reduced sample size in the stratum. Further, we found that an increased risk was significant only in superficial bladder cancer (1.86; 1.10–3.16). No significant association (1.42; 0.95–2.12) between the genotypes and invasive bladder cancer was observed, which is also likely due to the reduced number of subjects.
Adjusted for age, sex, and pack-years smoked in a logistic regression model.
Meta-analysis
We further performed a meta-analysis based on the published studies to better assess the association between the CCND1 G870A polymorphism and risk of bladder cancer. As shown in Table 5, five eligible and independent published studies were identified (Wang et al., 2002; Cortessis et al., 2003; Sanyal et al., 2004; Chung et al., 2008; Ye et al., 2008), in which the genotype distribution among the control subjects was consistent with Hardy–Weinberg equilibrium. Figure 1A shows that individuals with the 870AA genotype had no significantly increased risk (OR, 1.12; 95% CI, 0.95–1.32) compared with those with the GG genotype, and no significant association with risk of bladder cancer was observed in a dominant model of the 870A allele in all studies (1.02; 0.89–1.16) (Fig. 1B). Stratifying the studies by ancestry (i.e., Caucasians and Asians) showed that the AA genotype was associated with a significant risk for bladder cancer in Asians (1.48; 1.04–2.11), but not in Caucasians (0.90; 0.73–1.11). Similar effects for the G870A polymorphism on bladder cancer were observed in the dominant model either in Asians (1.31; 1.05–1.64) or Caucasians (0.89; 0.76–1.05). There was no evidence for between-study heterogeneity or publication bias by both the Q test and the Egger' and Begg's tests.
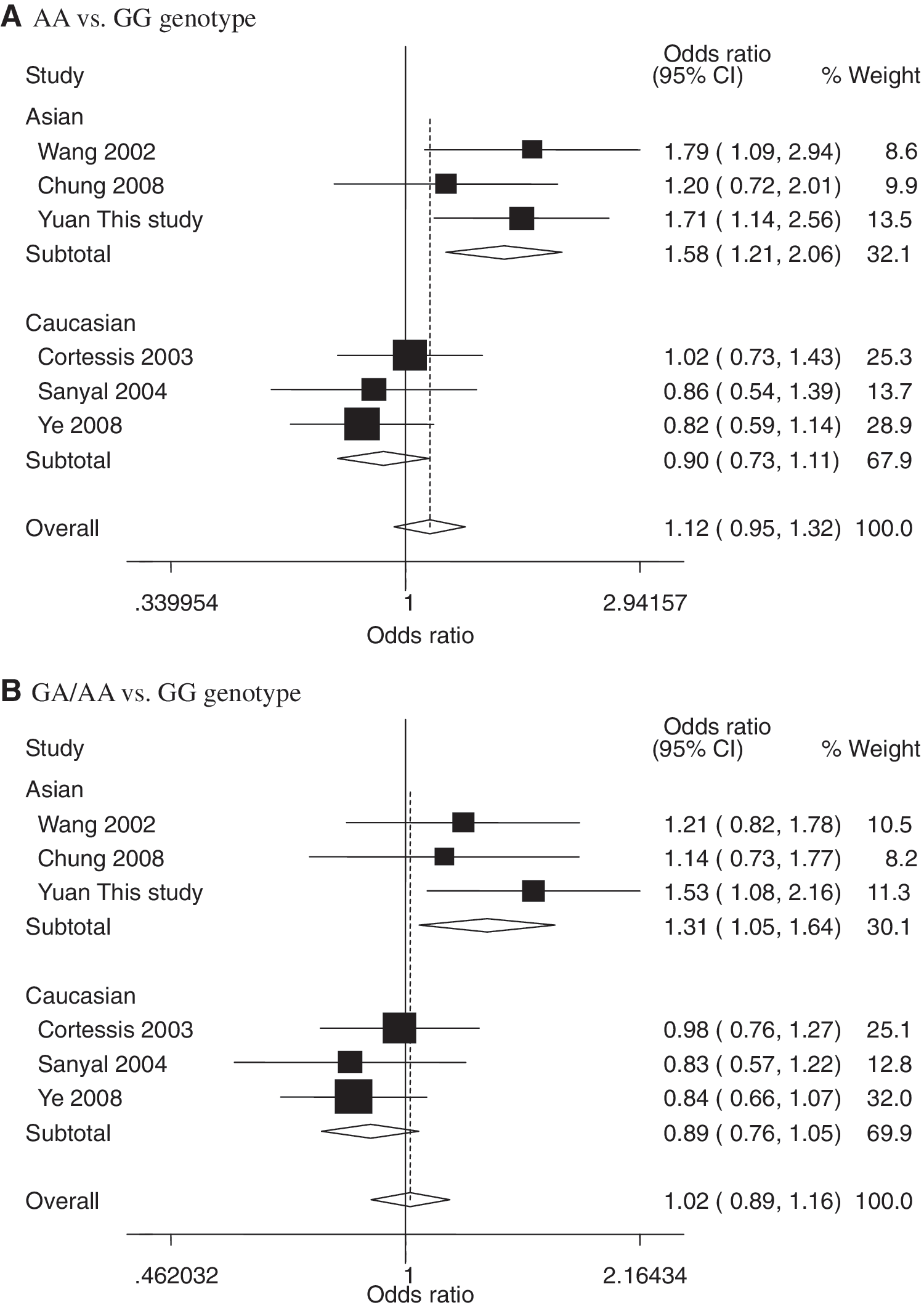
Forest plot of bladder cancer risk associated with the CCND1 G870A polymorphism. The squares and horizontal lines correspond to the study-specific odds ratio and 95% CI. The area of the squares reflects the study-specific weight (inverse of the variance). The diamond represents the pooled odds ratio and 95% CI. (
Discussion
In this hospital-based case–control study, we investigated the association of the CCND1 G870A polymorphism and risk of bladder cancer in a Chinese population. We found that the variant 870GA/AA genotypes were associated with a significantly increased risk of bladder cancer, and the association was more evident in older male smokers. Meanwhile, we also observed that a significantly increased bladder cancer risk was associated with superficial bladder cancer with grade 1, but not grade 2 or grade 3, compared with the control subjects. In the meta-analysis, we found that the 870GA/AA genotypes were associated with an increased risk of bladder cancer in Asians, but not in Caucasians.
The cell cycle is critical in cell proliferation, and the deregulation of G1 to S phase progression of the cell cycle is a frequent target in malignant transformation (Collins et al., 1997). CCND1, a regulatory protein involved in the cell cycle from G1 to S phase, has been regarded as an oncogene (Stacey, 2003), because overexpression of the protein accelerates the G1 phase and thus increases cell proliferation involved in carcinogenesis. To data, however, the biological mechanism of CCND1 in carcinogenesis has not been fully examined (Gupta et al., 2008). Over 100 SNPs have been identified in the CCND1 gene, and none of these SNPs result in amino acid changes. The CCND1 G870A variant occurs at the final intron–exon boundary and may alter the recognition of the exon 4 splice-donor site (Knudsen et al., 2006). It has been reported that the 870A allele may be correlated with both the increased risk of carcinoma and the poor patient outcomes of cancer. In the present study, we found that individuals who carried the 870GA/AA genotypes had an increased risk of bladder cancer compared with the GG genotype. The possible explanation is that the 870A allele may result in the elevated expression of a CCND1 variant with the increased oncogenic potential (Betticher et al., 1995).
Recently, several meta-analysis studies have been conducted to investigate the association between the CCND1 G870A polymorphism and risk of cancers (Pabalan et al., 2008; Tan et al., 2008). To date, a number of epidemiologic studies have reported the associations between the G870A polymorphism and bladder cancer risk, but the results are conflicting (Wang et al., 2002; Cortessis et al., 2003; Sanyal et al., 2004; Chung et al., 2008; Ye et al., 2008). Here, we also conducted a meta-analysis with more extensive data to assess the effect of this polymorphism on risk of bladder cancer. Our meta-analysis results further support our results for the Chinese population (1.54; 1.08–2.20), which showed that the variant 870GA/AA genotypes were associated with an increased risk of bladder cancer in Asians (1.31; 1.05–1.64), but not in Caucasians. These discrepant results could be due to genetic differences attributable to different ethnic populations, because the 870A minor allele frequency between Asians and Caucasians was different: 0.52 in Asians and 0.46 in Caucasians. The differences may contribute to the distinct distribution and frequency of subjects with age, tobacco exposure, and other unknown variables.
Tobacco smoking is known to cause bladder cancer, contributing to a >2.5-fold risk in smokers than in nonsmokers (Zeegers et al., 2000). Our results indicated that the risk associated with the G870A polymorphism was more evident in smokers. This may be because cigarette smoke generates reactive oxygen species production and induces DNA adducts (Hecht, 2002). In addition, our data suggest that the older men with the variant genotypes of the G870A polymorphism had a higher risk of bladder cancer. The possible explanation is that the people may be exposed to unknown risk factors involved in the etiology of bladder cancer over time as age increases, such as environmental pollutants (Cohen and Johansson, 1992). However, our small sample size might not have a sufficient power to detect the significant gene–environment interactions; thus, larger studies with more detailed environmental exposure data are needed to verify these findings.
Biomarkers for bladder cancer aim to replace or reduce the use of cystoscopy for diagnosis or surveillance of bladder cancer. Although much better tests than prostate-specific antigen (for prostate cancer detection) are needed, none of the reported bladder tumor markers are widely used. Many of the genetic markers associated with bladder cancer risk have been subjected to extensive studies that have examined their biological roles in bladder cancer development and progression. For example, Sanchez-Carbayo et al. (2007) reported that the SNP309 polymorphism in MDM2 was found to be associated with an earlier age onset of superficial disease, TP53 mutations, and poor outcomes in invasive bladder cancer. Similarly, Nadaoka et al. (2008) demonstrated that the HIF-1a polymorphism had a significant effect on the poor prognosis, but not the occurrence, of the patients undergoing radical cystectomy for bladder cancer. Others found genetic variations in genes involved in inflammation to be associated with bladder cancer risk, treatment response, and survival (Leibovici et al., 2005).
In the present study, we further investigated the association between the CCND1 G870A polymorphism and clinicopathologic characteristics of bladder cancer, which may help identify prognostic factors involved in different bladder cancer progression pathways (Murta-Nascimento et al., 2007). In the stratification for tumor grade and T stage, it appeared that individuals with the CCND1 870A allele had an increased risk of developing superficial bladder cancer with grade 1. It has been proposed that superficial and invasive bladder carcinomas have different etiologies involving different genetic and epigenetic defects (Wu, 2005). Therefore, it seems plausible that CCND1 is involved in the onset of superficial bladder cancer.
Although some of the results presented in this study are novel, the study has some limitations. First, only six case–control studies could be included for the meta-analysis as well as fewer ethnic groups for the stratification (three for Asians and three for Caucasians). Therefore, the results should be interpreted with caution. Second, because this study was a hospital-based study with lack of follow-up data, more detail clinical parameters in the follow-up are needed in the further study. Third, information on family history and occupations of bladder cancer patients in the study was not available, which restricted our further analysis on the role of family history and occupations in bladder cancer risk. Thus, our results in gastric cancer need to be validated in large studies in other populations with more detailed information on family history and occupations. Fourth, CCND1 contains many more polymorphisms than the G870A polymorphism mentioned in the study. Given the limited evidence available on other CCND1 polymorphisms, this study was restricted to the most extensively studied G870A polymorphism. Finally, our study has an 80% power to detect the lowest effect of OR = 1.52 with an exposure frequency of 30% under the current sample size; however, the power to detect interaction was very limited.
Conclusion
In this present study, we found that the CCND1 G870A polymorphism had an effect on increasing risk of bladder cancer in a Chinese population. In addition, our meta-analysis showed that the G870A polymorphism may contribute to susceptibility to bladder cancer risk in Asians, which was consistent with the results of our present study. However, our findings need to be validated by larger studies with diverse ethnic populations and more detailed environmental exposure information.
Footnotes
Acknowledgments
This study was partly supported by the National Natural Science Foundation of China (30872084, 30972444, and 30901166), the Key Program for Basic Research of Jiangsu Provincial Department of Education (08KJA330001), “Qinglan Project” Foundation for the Young Academic Leader of Jiangsu Province, and Jiangsu Provincial Graduates Innovative Project (CX08B-183Z).
Disclosure Statement
No competing financial interests exist.