
Abstract
We have evaluated functional polymorphism (rs3087243; in literature known also as CTLA4 CT60) in the cytotoxic T lymphocyte antigen 4 (CTLA4) gene, previously associated with several autoimmune diseases, for potential association with inflammatory bowel diseases (IBD). In addition, we investigated correlations between CTLA4 CT60 polymorphism and CTLA4 gene expression in peripheral blood lymphocytes and colon biopsies from IBD patients. We genotyped CTLA4 CT60 polymorphism in 266 healthy control subjects and 481 IBD patients and found statistically lower frequency of CTLA4 CT60 AA genotype in IBD patients (13.72%) compared to control subjects (23.31%; p = 0.001, odds ratio [OR] = 0.504) as well as lower allele frequency of minor A allele in IBD patients (0.346) compared to control subjects (0.461, p < 0.001, OR = 0.623). The association was confirmed with both major forms of IBD, Crohn's disease, and ulcerative colitis (UC), but was slightly stronger in UC patients, particularly when we compared allele frequency of A allele in UC patients (0.299) and control subjects (0.461, p < 0.001, OR = 0.500). We found lower expression of the CTLA4 gene in blood lymphocytes from IBD patients compared to control subjects (p < 0.001) and higher CTLA4 expression in biopsies taken from inflamed part of the colon compared to noninflamed part of the colon (p = 0.021). We found lower expression of soluble CTLA4 isoform than membrane-bound full-length isoform in peripheral blood lymphocytes from IBD patients compared to control subjects (p = 0.010) and in lymphocytes from IBD patients with CTLA4 CT60 GG genotype compared to IBD patients with AA genotype (p = 0.034). Our genotype and gene expression data suggest that CTLA4 plays a role in IBD pathogenesis. Polymorphism CTLA4 CT60 contributes to genetic susceptibility to IBD in Slovenian population and regulates expression of CTLA4 isoforms.
Introduction
The cytotoxic T lymphocyte antigen 4 (CTLA4) gene is a key negative regulator of the T lymphocyte immune response (Teft et al., 2006). The CTLA4 gene region has been previously associated with risk for a number of chronic autoimmune diseases (Ueda et al., 2003), and association studies for CTLA4 in IBD were warranted (Kristiansen et al., 2000). In addition, genome scan metaanalysis suggested IBD susceptibility loci on 2q33 spanning 35 cM disease-associated region, which includes also the CTLA4 gene region (van Heel et al., 2004), thus further suggesting CTLA4 as a good candidate gene for IBD. CTLA4 is expressed on activated T cells and also on B cells when they are stimulated by activated T cells (Kuiper et al., 1995; Oaks et al., 2000). CTLA4 is a member of immunoglobulin superfamily and is highly homologous to another T cell surface receptor CD28. CTLA4 similarly as CD28 bind to the same ligands, B7-1 and B7-2, but CTLA4 binds with much higher affinity. B7-1 (CD80) and B7-2 (CD86) are members of the B7 family of molecules expressed on antigen-presenting cells. Activated T cells and antigen-presenting cells play a major role in the mucosal pathogenesis of IBD (Oaks et al., 2000; Niess, 2008). Further, CTLA4 has been also shown to regulate dendritic-cell-induced activation (McCoy et al., 1999), and mucosal dendritic cells are assumed to play a key role in regulating immune responses (Niess, 2008). CTLA4 protein exists in two forms (Linsley et al., 1995). Membrane-bound form is biologically more active. Soluble isoform of CTLA4 (sCTLA4) protein is the result of alternative splicing and deletion of the exon coding for the transmembrane region (Linsley et al., 1995) and has immunoregulatory properties in vitro (Oaks et al., 2000). It was also shown that an altered level of sCTLA4 mRNA could influence the activation of CTLA4 or CD28 (Ueda et al., 2003).
Several polymorphisms of the CTLA4 gene have been described and used in association studies in several immune and autoimmune diseases. Initially, single-nucleotide polymorphism (SNP) + 49A/G (rs231775) in the CTLA4 gene coding region causing Ser/Thr substitution was the most extensively studied SNP in CTLA4 disease association studies. Recently, however, it was suggested that another SNP rs3087243 (in literature known as CTLA4 CT60 or + 6230 A > G) located 3′ to the known polyadenylation site of the CTLA4 gene influences CTLA4 functional expression and is a major contributor to disease susceptibility to several autoimmune diseases statistically associated with the CTLA4 gene region (Ueda et al., 2003). Functional tests suggested that the disease-susceptible CTLA4 CT60-G allele regulates lower amount of sCTLA4 mRNA than the disease protective CT60-A allele, while the full-length form is not regulated by this variant (Ueda et al., 2003). CTLA4 CT60 was further associated with many immune diseases, including rheumatoid arthritis (Walker et al., 2009), leukemic relapse (Perez-Garcia et al., 2009), Grave's disease (Petrone et al., 2005), Addison's disease (Blomhoff et al., 2004), and type 1 diabetes (Howson et al., 2007).
We performed an association study in Slovenian IBD patients as almost no comprehensive association studies for the CTLA4 CT60 SNP have been done in Caucasians and a limited number of association studies in some Asian populations were inconclusive about the role of CTLA4 CT60 SNP in IBD susceptibility. In addition, our study was the first that investigated CTLA4 gene isoform expression and correlation between SNP CT60 and isoform expression in peripheral blood lymphocytes and colon biopsies from IBD patients.
Materials and Methods
Subjects and samples
Patients and control subjects were enrolled in this study as described previously (Potocnik et al., 2004). In this study we enrolled 481 IBD patients, including 315 CD patients, 137 UC patients, and 29 patients with proctitis, as well as 266 healthy unrelated blood donors as a control group. Sex- and age-matched healthy blood donors were selected as control subjects in this association study. All control subjects were Slovenian and thus of Caucasian origin representing the general Slovenian population. The same control subjects as in this study were used in our previous association study (Potocnik et al., 2004) where several SNPs were genotyped and the resulting allele and genotype frequencies in control subjects and in patients did not differ significantly, thus suggesting the same genetic structure in control subjects and patients for the most of the genes except for the disease-associated genes. In this study, 49% of IBD patients were men. The mean age of IBD patients was 38.6 years and mean age at diagnosis was 27.2 years. All patients gave informed consent. The mean age in the control group was 37.15 years, and 44.7% of control subjects were men, which is not significantly different from that in the IBD patients. Demographic data and clinical characteristics of IBD patients and control subjects are described in Table 1. The study was approved by Slovenian national committee for medical ethics.
IBD, inflammatory bowel disease; SD, standard deviation; UC, ulcerative colitis; CD, Crohn's disease; TNF-α, tumor necrosis factor-α.
RNA and DNA were obtained from 9 mL of peripheral blood. First, we collect peripheral blood lymphocytes using FicollPaque PLUS (GE Healthcare), and then RNA and DNA were isolated from lymphocytes using TRI reagent (Sigma) according to manufacturer's instructions. We also obtained RNA and DNA from tissue samples. Biopsies were collected in RNAlater (Ambion) and stored at −20°C until analysis. Tissue was disrupted with homogenizer Bullet Blender (Next Advance) using zirconium oxide beads in TRI reagent from which RNA and DNA were isolated according to manufacturer's instructions (Sigma).
Genotyping of CTLA4 CT60 SNP
Genotyping of CTLA4 CT60 was performed by polymerase chain reaction (PCR) followed by restriction fragment length polymorphism. Primers and restriction enzymes were selected according to previous study (Torres et al., 2004). PCR products were resolved in 2% agarose gel that was stained with ethidium bromide. PCR product was 216 bp long. PCR products were digested using 1 unit of NcoI restriction enzyme (Fermentas) at 37°C overnight. Digested products were resolved in 2% agarose gel. Samples demonstrating a 216 bp band were assigned genotype GG, while samples demonstrating a 196 bp band were typed as AA. Samples demonstrating two bands of 216 and 196 bp were typed as AG. Genotyping was performed for all patients and healthy individuals.
Gene expression measurements
First, we reverse transcribed RNA samples derived from peripheral blood lymphocytes from patients and healthy individuals and also from tissue samples of patients, using High Capacity Reverse Transcription kit (Applied Biosystems). We measured total expression of the CTLA4 gene and expression of both CTLA4 isoforms: sCTLA4 and full length CTLA4 (flCTLA4) isoform. For detection of total CTLA4 expression, we performed quantitative real-time PCR using FAM-labeled TaqMan gene expression assay (Hs00175480_m1; Applied Biosystems) that targets exon 1/2 boundary and detects both CTLA4 isoforms. We used VIC-labeled probe for detection of 18S rRNA (Applied Biosystems), which was used as a reference gene in the multiplex PCR with CTLA4 Hs00175480_m1 assay. PCR cycling conditions were as follows: initial denaturation at 95°C for 10 min followed by 40 cycles of 95°C for 15 s and 60°C for 1 min. Real-time PCR was performed on LC480 instrument (Roche) using Maxima Probe qPCR Master Mix (Fermentas).
We performed quantitative PCR using LCGreen dye (Idaho Technology) and previously published primers (Mayans et al., 2007) for specific quantification of sCTLA4 and flCTLA4 isoform. Cycling conditions on LC480 instrument (Roche) were as follows: initial denaturation at 95°C for 5 min followed by 45 cycles of 95°C for 1 min, 60°C for 30 s, and 72°C for 30 s.
Statistical analysis
We used the two-sided Fisher's exact test to compare CTLA4 CT60 genotype and allele frequencies between control group and IBD patients. Relative RNA quantification for total expression of the CTLA4 gene was determined using comparative Ct method as described by Livak and Schmittgen (2001). To determine the sCTLA4/flCTLA4 mRNA expression, we used the formula 2−(Ct[sCTLA4]−Ct[flCTLA4]) as described previously (Ueda et al., 2003). When comparing total expression of the CTLA4 gene and expression of CTLA4 isoforms in peripheral blood lymphocytes and tissue samples and also between different genotypes of CTLA4 CT60 SNP, we used nonparametric Mann–Whitney U-test. For all tests we used SPSS 17.0 (SPSS Inc.) statistical package. In all tests p < 0.05 was considered to indicate statistical significance.
Results
Genotyping of CTLA4 CT60 SNP
We genotyped CTLA4 CT60 SNP in 266 healthy control subjects and 481 IBD patients, including 315 CD patients, 137 UC patients, and 29 proctitis patients. We found statistically significant correlation between CTLA4 CT60 polymorphism and Slovenian IBD patients comparing both genotype and allele frequencies (Table 2). The frequency of CTLA4 CT60 AA genotype was lower in IBD patients (13.72%) than in control subjects (23.31%; p = 0.001, odds ratio [OR] = 0.504). Allele frequency of minor A allele was statistically lower in IBD patients (0.346) than in control subjects (0.461, p < 0.001, OR = 0.623).
Total IBD includes CD patients, UC patients, and proctitis patients; proctitis patients were, however, not analyzed separately due to low number of patients with this subphenotype.
p values showing statistically significant association are written in bold.
OR, odds ratio; CI, confidence interval.
When comparing CTLA4 CT60 SNP genotype and allele frequencies with healthy control subjects separately for each major form of IBD, we found slightly stronger association to UC than to CD. In the group of UC patients the frequency of AA genotype (8.76%) was statistically lower than in the control group (23.31%, p < 0.001, OR = 0.316) when AA homozygotes were compared to heterozygotes and GG homozygotes in one group (AG + GG) (dominant model for G allele and recessive model for A allele). Allele frequency of minor A allele was 0.461 in control subjects and it was reduced to 0.299 in UC patients (p < 0.001, OR = 0.500). In the group of CD patients we also found reduced allele frequency of minor A allele (0.367) compared to control group (p = 0.002, OR = 0.683). Frequency of AA genotype of CT60 SNP was also statistically lower in CD patients (15.24%) than in control subjects (p = 0.015, OR = 0.592). Genotype frequencies for CTLA4 CT60 polymorphism in control subjects and IBD patients were in Hardy–Weinberg equilibrium. We found no statistical correlation between CTLA4 CT60 polymorphism and clinical characteristics of IBD patients.
Gene expression analysis
Total CTLA4 gene expression in peripheral blood lymphocytes and tissue samples
We analyzed total CTLA4 gene expression in peripheral blood lymphocytes from 68 healthy individuals and from 88 IBD patients. In the group of IBD patients, 66 were CD patients and 22 were patients with UC. The CTLA4 genotype distribution in the patients and control subjects enrolled in expression analysis was similar to that in all patients enrolled in the association analysis. The frequency of AA genotype was similar in all IBD patients (13.7%) as in IBD (n = 88) patients used for expression analysis in lymphocytes (18.1; p = 0.321) and in IBD patients (n = 73) enrolled in expression analysis in tissue samples (12.33; p = 0.855). The frequency of AA genotype was similar in all control subjects (n = 266; 23.3%) as in the control subjects used for expression study (n = 68; 27.9%, p = 0.431). We found higher expression of the CTLA4 gene in peripheral blood lymphocytes from healthy control subjects compared to IBD patients (p < 0.001, Fig. 1). When comparing total expression in peripheral blood lymphocytes between control group and CD or UC patients separately, we found statistically lower expression of the CTLA4 gene in peripheral blood lymphocytes in both CD (p > 0.001) and UC (p = 0.003) cases (Fig. 1b, c). When comparing CTLA4 expression according to genotype, we found slightly higher expression of the CTLA4 gene in peripheral blood lymphocytes from IBD patients with AA genotype (mean normalized and calibrated expression 1.47) compared to patients with GG genotype (mean normalized and calibrated expression 0.76) although difference was not statistically significant (p = 0.273).
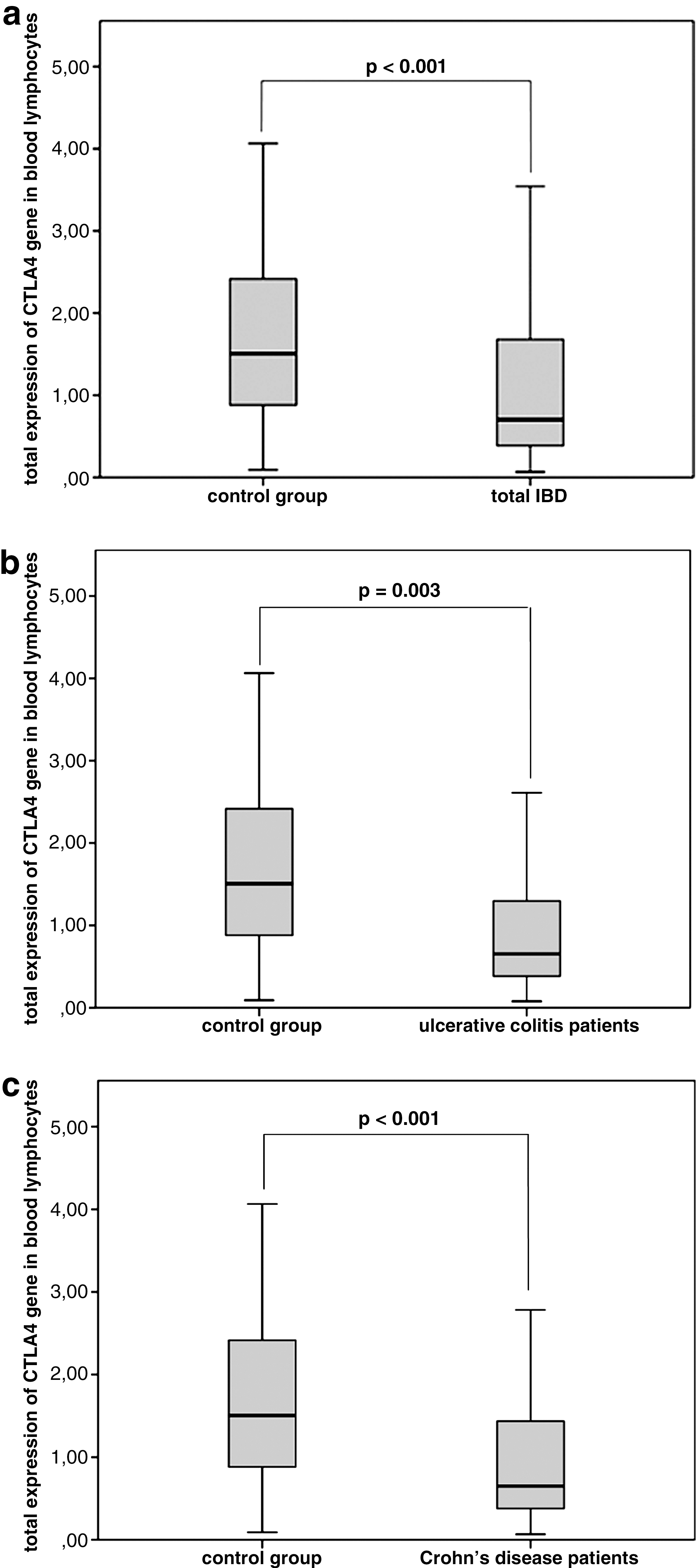
Total expression of the cytotoxic T lymphocyte antigen 4 (CTLA4) gene in peripheral blood lymphocytes compared between total inflammatory bowel disease (IBD) patients and healthy control subjects (
We analyzed tissue samples from 73 IBD patients. For 28 IBD patients, matching pairs of biopsies from inflamed and noninflamed part of the colon were available; for the rest 45 IBD patients, a single-biopsy sample either from inflamed or noninflamed part of the colon was available. All together, 105 biopsies, including 57 from noninflamed and 48 inflamed biopsies, were analyzed for CTLA4 expression. Using nonparametric Mann–Whitney U-test, we found statistically significant higher expression of the CTLA4 gene in inflamed parts of tissue compared to noninflamed parts (p = 0.021, Fig. 2). We also found higher expression of the CTLA4 gene in biopsies taken from inflamed parts of the colon from patients with AA genotype (mean normalized and calibrated expression 2.00) compared to patients with GG genotype (mean normalized and calibrated expression 0.44) although difference was not statistically significant (p = 0.096).
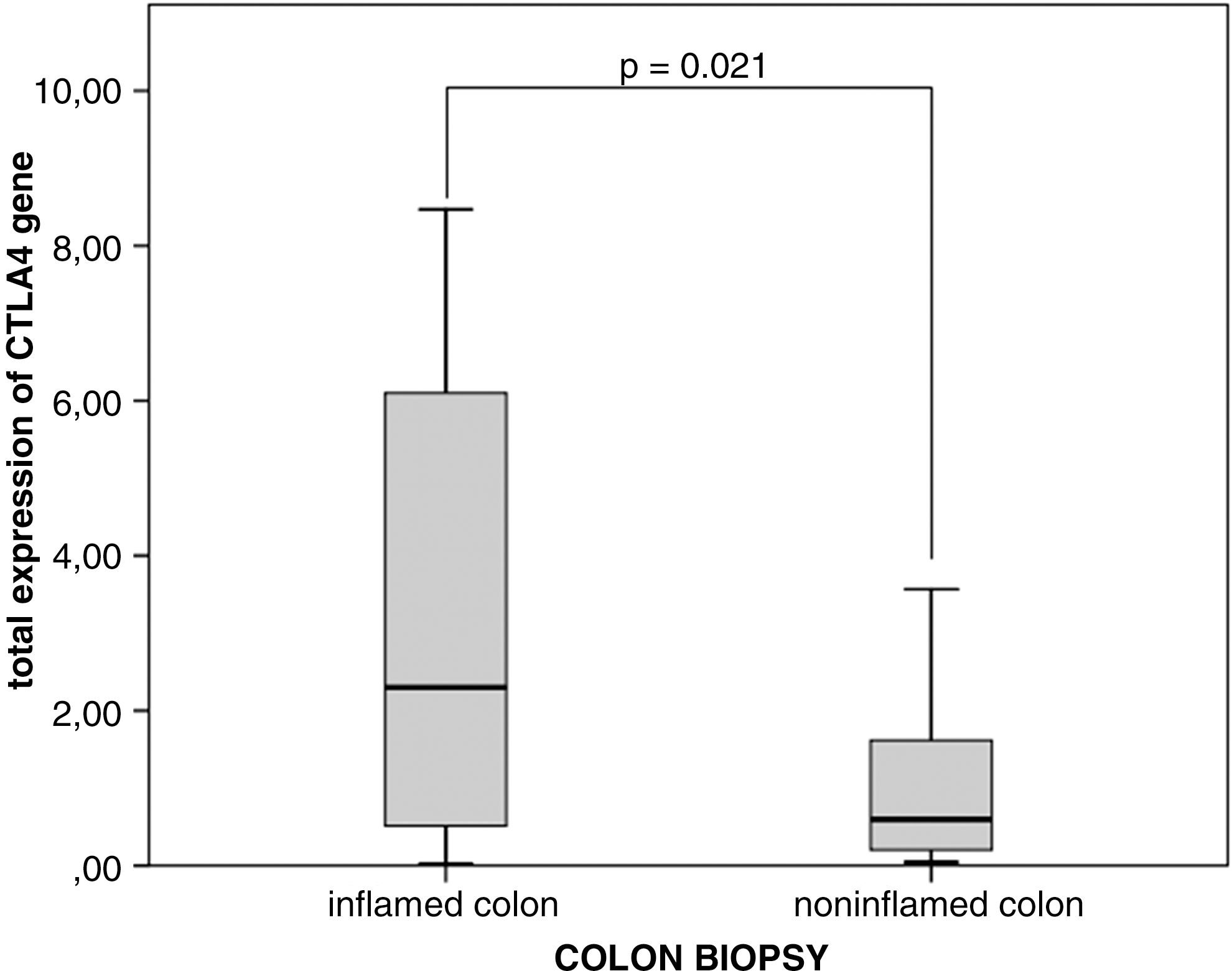
Relative expression of the CTLA4 gene in tissue samples. The CTLA4 gene is upregulated in biopsies taken from inflamed parts of colon compared to biopsies taken from noninflamed parts of the colon.
Expression of sCTLA4 and flCTLA4 isoforms in peripheral blood lymphocytes and tissue samples
We measured expression of CTLA4 isoforms in peripheral blood lymphocytes from 68 healthy control subjects and from 88 patients with IBD, and correlated results with CTLA4 CT60 SNP genotype. First, we found statistically lower expression of sCTLA4 in peripheral blood lymphocytes from IBD patients (mean normalized and calibrated expression 0.51) compared to healthy individuals (mean normalized and calibrated expression 0.61, p = 0.010). Further, we found statistically lower sCTLA4/flCTLA4 ratio in peripheral blood lymphocytes from IBD patients with CT60 GG genotype than from patients with AA genotype (p = 0.034). Mean normalized and calibrated expression in IBD patients with AA genotype was 0.60 compared to 0.47 in patients with GG genotype. Results are shown in Figure 3. The difference is even higher when we compared mean normalized and calibrated sCTLA4/flCTLA4 ratio expression between CD patients with AA genotype (0.63) and CD patients with GG genotype (0.45, p = 0.011). We also found increased mean normalized and calibrated sCTLA4/flCTLA4 ratio expression in UC patients with AA genotype (0.80) compared to UC patients with GG genotype (0.49), but due to small number of UC patients available for expression analysis, we had no enough statistical power to confirm this correlation. In the control group, statistical difference was not reached (p = 0.095) although individuals with CT60 GG genotype showed lower expression of sCTLA4 isoform.
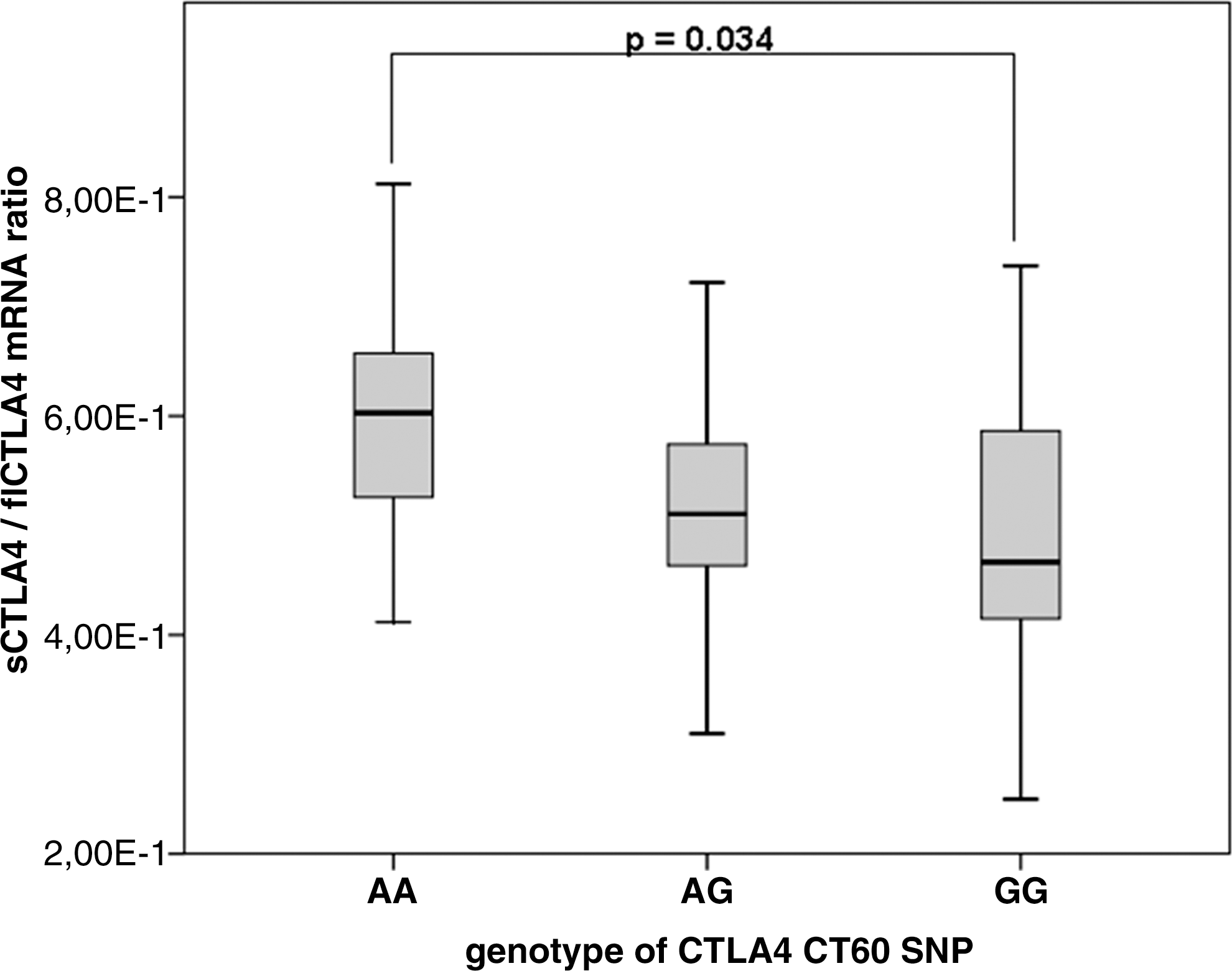
Ratio between expression levels of soluble isoform of the CTLA4 (sCTLA4) gene and membrane bound full length CTLA4 (flCTLA4) isoform. Ratio measured by real-time quantitative polymerase chain reaction of RNA purified from peripheral blood lymphocytes from patients with IBD divided in the three CTLA4 CT60 genotype groups.
Expression of CTLA4 isoforms measured in tissue samples showed higher sCTLA4/flCTLA4 ratio in noninflamed parts (mean normalized and calibrated expression 0.035) than in inflamed parts (mean normalized and calibrated expression 0.020) with borderline statistical significance (p = 0.065).
Discussion
In our study we found a statistically significant association of CTLA4 CT60 polymorphism and both major forms of IBD, UC and CD. We also found upregulated expression of the CTLA4 gene in inflamed colon biopsies compared to noninflamed parts and lower expression of sCTLA4 isoform in lymphocytes from IBD patients with CTLA4 CT60 GG genotype than in lymphocytes from IBD patients with AA genotype. Our genotype and gene expression data suggest that CTLA4 plays a role in IBD pathogenesis. Our study is the first that associated genotype of CT60 SNP with the expression level of sCTLA4 isoform in IBD patients and also first that associated disease-susceptible CTLA4 CT60-G allele with IBD among Caucasians.
The CTLA4 polymorphisms were previously associated with IBD in some Asian populations (Hou et al., 2005; Machida et al., 2005; Jiang et al., 2006; Luo et al., 2009), but in some studies no association between CTLA4 and IBD was reported like in Chinese (Xia et al., 2002) and Iranian populations (Lankarani et al., 2006). There is limited data on IBD association studies in Caucasian population. No association between CTLA4 and IBD was reported in a Hungarian population; however, the only analyzed CTLA4 SNP in this study was +49 C > T (Magyari et al., 2007), which has been proved not to be in highest linkage disequilibrium with functional SNP in the CTLA4 gene region (Ueda et al., 2003). CTLA4 CT60 SNP analyzed in our IBD association study, however, was functionally proven (Ueda et al., 2003) and was associated with several autoimmune (Ueda et al., 2003; Machida et al., 2005) and other diseases, including celiac disease (van Belzen et al., 2004) and systemic lupus erythematosus (Torres et al., 2004).
Recent genome-wide association (GWA) studies in IBD patients confirmed several previously identified genes and discovered several new IBD loci. GWA studies greatly contributed to improved replication of candidate genes in different populations; however, many of the highly significant genes are still reported only by a few or even a single GWA study. For example, the CDKAL1 gene was reported as an IBD-associated gene after at least six previous GWA studies fail to associate this gene with IBD (The Wellcome Trust Case Control Consortium, 2007). More over, 21 of 30 candidate genes were identified only by metaanalysis and were not reported by single GWA study (Barrett et al., 2008). This disconcordance between GWA studies could be due to different populations or different genotyping platforms used in the study. Candidate-gene-focused association studies, as is the case in our study for CTLA4, could still identify new IBD genes missed or not reported as the most significantly IBD-associated genes in GWA studies. Such examples include the TNF-α gene associated with IBD in >15 independent candidate-gene-focused association studies and the TLR4 gene confirmed in three meta-analysis, but neither TNF-α or TLR was reported in the recent GWA studies.
To the best of our knowledge, we were the first to perform CTLA4 expression studies including total CTLA4 expression and isoform expression in IBD patients. Initially, Ueda et al. (2003) found that the ratio of sCTLA4 to flCTLA4 mRNA splice forms in unstimulated CD4 T cell lines was 50% lower in cell lines derived from individuals with disease-susceptible CT60 GG genotype compared to those derived from individuals with disease-protective AA genotype, and warranted further CTLA4 isoform expression studies in comprehensive cohorts of clinical samples. We first analyzed expression of CTLA4 isoforms in peripheral blood lymphocytes from 68 healthy individuals and 88 IBD patients and found statistically lower sCTLA4/flCTLA4 ratio in IBD patients with CTLA4 CT60 GG genotype compared to patients with AA genotype (Fig. 3). We also found lower sCTLA4/flCTLA4 ratio in peripheral blood lymphocytes from IBD patients compared to sCTLA4/flCTLA4 ratio in lymphocytes from healthy individuals. We found slightly lower sCTLA4/flCTLA4 ratio in peripheral blood lymphocytes from healthy individuals with CTLA4 CT60 GG genotype compared to AA genotype. Previously, lower sCTLA4/flCTLA4 ratio was identified in peripheral blood lymphocytes from myasthenia gravis patients compared to sCTLA4/flCTLA4 ratio in lymphocytes from healthy individuals regardless to the CTLA4 genotype status; however, only +49 and −318 SNPs, but not CT60 SNP, were analyzed in this study (Gu et al., 2008). Atabani et al. (2005) found lower sCTLA4/flCTLA4 ratio in CD4 + CD25 + T regulatory lymphocytes from healthy individuals with CT60 GG genotype compared to individuals with AA genotype. Palacios et al. (2008) confirmed the influence of CTLA4 CT60 SNP on sCTLA4/flCTLA4 ratio expression in peripheral blood lymphocytes from multiple sclerosis patients but not in healthy individuals, suggesting that epigenetic changes or changes in transregulation that are generated by the disease process might affect isoform CTLA4 expression and regulatory T-cell function in lymphocytes from multiple sclerosis patients. Palacios et al. (2008), in addition, found changes in sCTLA4/flCTLA4 ratio in lymphocytes from patients after chemotherapy. We also found a stronger effect of CTLA4 CT60 genotype on sCTLA4/flCTLA4 isoform expression in peripheral blood lymphocytes from IBD patients compared to healthy individuals, further confirming epigenetic influences.
In addition to the analysis of CTLA4 isoforms, we have also analyzed total expression of the CTLA4 gene in peripheral blood lymphocytes from healthy individuals and IBD patients and from tissue samples. We found statistically lower expression of the CTLA4 gene in peripheral blood lymphocytes from IBD patients compared to healthy control subjects, and also higher expression of the CTLA4 gene in patient tissue biopsies taken from inflamed parts of colon compared to those taken from noninflamed parts of colon. Increased CTLA4 expression on activated T cells compared to nonactivated T cells was detected (Lindsten et al., 1993; Linsley et al., 1994; Kuiper et al., 1995); therefore, increased relative expression of CTLA4 identified in the inflamed colon as compared with that in noninflamed colon detected in our study most probably reflects the increased number of activated T cells in the inflamed part of the colon. The precise molecular mechanism of how increased relative expression of CTLA4 in the inflamed colon compared to noninflamed colon is involved in IBD pathogenesis needs to be further determined. Altered CTLA4 expression might disturb the CTLA4-dependent regulation of dendritic-cell-induced activation and cytotoxicity of CD8 + T cells (McCoy et al., 1999). Disregulation of dendritic cells contributes to pathogenesis of IBD (Coombes and Powrie, 2008; Niess, 2008). Also, in the mouse model for UC, increased expression of CTLA4 was identified on mice T cells (Liu et al., 2001). Total expression of the CTLA4 gene also differed between different genotypes of CTLA4 CT60 SNP. The exact mechanism of how the expression ratio between sCTLA4 and flCTLA4 isoforms and total CTLA4 expression influences the lymphocyte function and disease pathogenesis also needs further study. However, our work suggests an important role of the CTLA4 gene in pathogenesis of IBD.
Conclusions
We showed the association of CT60 polymorphism in the CTLA4 gene with IBD, especially UC, in Slovene patients. The frequency of the CTLA4 CT60 disease susceptible G allele was significantly higher in patients with IBD than in the control group. We also found a correlation between CT60 genotype and expression of CTLA4 isoforms, as it was shown in a previous study for other autoimmune diseases (Ueda et al., 2003). Results also showed higher expression of the CTLA4 gene in inflamed tissue parts compared to noninflamed parts. These data indicate that the CTLA4 gene is involved in pathogenesis of IBD among Slovene patients and that CT60 polymorphism is an important target that can regulate its expression. Our study also demonstrates feasibility to detect correlations between CTLA4 genotype and gene expression in peripheral blood lymphocytes and colon biopsies from IBD patients. Our study suggests that genotype/gene expression studies could be helpful in linking most significantly disease-associated SNPs in noncoding regions or “gene deserts” with genes they regulate.
Footnotes
Acknowledgments
We would like to thank Department of Gastroenterology and Endoscopy of University Clinical Centre Maribor for clinical samples. This study was supported by Slovenian Research Agency.
Disclosure Statement
No competing financial interests exist.