
Abstract
Cyclooxygenase-2 (COX-2), an inducible enzyme, has been implicated in the progression and angiogenesis of breast cancer. The aim of the study is to quantify the concentration of COX-2 and its association with clinico-pathological parameters and response to treatment in patients with invasive ductal carcinoma receiving both neo-adjuvant and adjuvant chemotherapy. The level of COX-2 was estimated using a novel biosensor-based surface plasmon resonance technique in serum of 84 patients with breast cancer (48 patients of neo-adjuvant chemotherapy and 36 patients of adjuvant chemotherapy) and 40 age- and gender-matched normal individuals. A significant increase in COX-2 level was observed in patients compared with normal individuals (p > 0.0001). The COX-2 level in serum was found to be significantly higher in patients with lymph node involvement (p < 0.0061). 68% (33/48) of the patients receiving neo-adjuvant chemotherapy showed significantly (p < 0.0025) reduced COX-2 levels. This study shows significant decrease of COX-2 level in patients with breast cancer treated with both neo-adjuvant and adjuvant chemotherapy. Estimation of COX-2 level in serum may serve as a tumor biomarker in patients with breast cancer.
Introduction
A defect in the apoptotic pathway allows tumor cells to survive for prolonged periods of time, accumulate genetic errors, and live in a suspended state that permits spread of metastasis. COX-2 inhibitors, aspirin, and celecoxib can restore proper function to cell death pathways in breast cancer (Basu et al., 2005; Shen et al., 2006), but their mechanism of action is unclear. COX-2 has prognostic implication in patients with breast cancer. This study reports the concentration of COX-2 in the sera as well as tissue of patients with breast cancer and compares it with the normal individuals by SPR technology. COX-2 levels were also evaluated after three cycles of chemotherapy.
Materials and Methods
Selection of patients
The case-control study was performed on serum samples obtained from 84 patients with histologically confirmed breast cancer and 40 age, sex, and ethnicity matched healthy subjects. Only patients with invasive ductal carcinoma, attending the breast cancer clinic, Department of Surgery at All India Institute of Medical Sciences (AIIMS), New Delhi, India were included in the study. Patients with metastasis or who were already taking a nonsteroidal anti-inflammatory drug (NSAID) were excluded. TNM (tumor, node, and metastasis) classification was performed according to the diagnostic criteria of the American Joint Committee on Cancer. 15 breast cancer tissue samples were also collected from randomly selected patients. The Ethics Committee of AIIMS approved the study protocol, and informed consent was received from all participating subjects. The patients were treated with standard FEC regimen (5-fluorouracil, epirubicin, and cyclophosphamide) at 500 mg/m2, 75 mg/m2 and 500 mg/m2, respectively. The levels of COX-2 in serum were estimated in patients before and after three cycle of both neo-adjuvant and adjuvant chemotherapy.
Separation of sera from blood and extraction of protein from cancer tissue
Five milliliters of venous blood was collected from each individual in vaccutainers under aseptic conditions. It was allowed to settle for 1 h at room temperature. The buffy coat was removed from the blood and centrifuged at 3000 rpm for 20 min. Serum was collected and stored at −70°C in multiple aliquots.
Breast cancer tissue was collected in liquid nitrogen and crushed in a mortar and pestle to a fine powdered form. I.P. lysis buffer (5 mM Tris-HCl, pH-7.4, 2 mM EDTA,10 μL protease inhibitor cocktail,10 mg/mL benzamidine, 5 mg/mL leupeptin, and 5 mg/mL trypsin inhibitor) (1000 μL/g of tissue) was added to the tissue. The sample was centrifuged at 12,000 rpm for 20 min at 4°C. The supernatant was collected and stored at −80°C until use.
Estimation of COX-2 level in serum and tissue of patients with breast cancer by SPR
Human IgG-COX-2 (Santa Cruz Biotechnology, Inc.) was immobilized on the surface of CM5 sensor chips by amine coupling. Equal volumes (115 μL) of N-hydroxysuccinimide (2.3 mg in 200 μL of water) and N-ethyl-N′-(3-dimethyl-aminopropyl) carbodiimide (15 mg in 200 μL of water) obtained from Pharmacia were mixed, and 75 μL of this solution was passed at the flow rate of 5 μL/min across the CM5 sensor chips to activate the carboxy methylated dextran surface. After this, 0.1 μL (20 ng) of COX-2 antibody in 10 mM sodium acetate (209.9 μL) pH 4.7 was passed at the flow rate of 5 μL/min across the activated surface, and the unreacted groups were blocked by ethanolamine (50 μL).
To prepare a standard curve for COX-2, 15 different concentrations of purified recombinant COX-2 (3.3, 6.6, 9.9, 13.2, 16.5, 19.8, 23.1, 26.4, 29.7, 33.0, 36.3, 39.6, 42.9, 46.2, and 49.5 μg) were passed over the immobilized antibody, and the corresponding resonance unit (RU) was obtained. A standard curve of RU versus concentration of COX-2 was plotted. After this, 40 μL of 1:99 dilutions (in HBS-EP buffer [0.01M HEPES, 0.15M NaCl, 2mMEDTA, 0.005% surfactant P20, pH 7.4]) of serum and tissue lysate were passed over the immobilized COX-2 antibody on the sensor chip at a flow rate of 10 μL/min. The RU for each sample was recorded, and the concentration of COX-2 was derived from the standard curve.
Western blot of blood sera
To confirm the presence of COX-2 in serum, 3 patients were randomly selected from the study group of 84. Samples were prepared by removing major interfering protein by plasma 7 multiple affinity removal spin cartridge (Agilent Technologies) according to the manufacturer's protocol and concentrated by centricon (Agilent Technologies) at 4°C at 2000 rpm. The protein concentration of the supernatant was determined by Bradford assay (Bio-Rad). The concentrated samples (50 μg) were boiled for 5 min with gel-loading buffer (100 mM Tris, 10% mercaptoethanol, 20% glycerol, 4% sodium dodecyl sulfate, and 2 mg/mL bromophenyl blue). Protein was separated on 10% sodium dodecyl sulfate-polyacrylamide minigels using the Laemmli buffer system and transferred to nitrocellulose membranes (Millipore). Nonspecific IgGs were blocked with 5% nonfat dried milk in TBS-I (10 mM Tris-Cl pH 7.5, 150 mM NaCl in milliQ water) for 2 h. The blot was incubated with specific antibodies of COX-2 (1:400; Santa Cruz Biotechnology). Protein bands were detected using enhanced chemiluminescence (Pierce ECL Western Blotting Substrate).
Statistical analysis
Statistical procedures were carried out using Graphpad Instat 3 software, and p < 0.05 was considered statistically significant. For the comparison of the findings, paired and unpaired t-test was performed by reject hypothesis. The degree of freedom was measured by subtracting 2 from the total number of the study group. The power calculation was 1.00.
Results
Clinicopathological data of patients with breast cancer
The clinical profile of the patients with breast cancer has been shown in Table 1. The age of the patients in this study ranged from 22 to 67 years with a mean ± standard deviation (SD) of 43.81 ± 9.94. According to TNM staging 28 patients (39.3%) had T4 tumor size (growing into the chest wall or skin) and 24 patients (10.8%) had T2 size (less than 2 cm). Fifty one percent patients presented with stage III tumors, followed by stage II (44.3%) and 4 patients had stage I (4.7%). Most of the patients had a history of lymph node involvement (66.6%) and were denoted as N+, whereas those lacking lymph node metastasis were N0 (33.4%). Estrogen receptor (ER)+ 63.0% (53 of 84), ER− 37.0% (31 of 84), and PR+ 58.3% (49 of 84), progesteron receptor (PR)− 41.7% (35 of 84), HER2+ 73.8% (62 of 84), and human epidermal growth factor receptor 2 (HER2)− 26.2% (22 of 84) were observed in patients.
ER, estrogen receptor; PR, progesteron receptor; HER2, Human epidermal growth factor receptor 2.
COX-2 assessment by SPR
The SPR signal for immobilization of COX-2 antibody was 20148.0 RU (Fig. 1). Fifteen different concentrations of pure recombinant COX-2 in HBS-EP buffer were passed over the immobilized COX-2 antibody, and the RU obtained were 20192.1, 20248.5, 20309.7, 20343.1, 20438.6, 20397.8, 20490.1, 20514.7, 20607.5, 20622.6, 20717.2, 20728.1, 20808.9, 20978.2, and 21053.3 respectively. The standard curve was plotted with RU obtained from the sensogram with different concentrations of pure COX-2. The slope and intercept are in the following form: y = 17.149x + 20111.

Sensogram of immobilization of anti-COX-2 antibody on CM5 sensor chip. COX-2, cyclooxygenase-2, RU, resonance unit; EDC, N-ethyl-N′-(3-dimethyl-aminopropyl) carbodiimide; NHS, N-hydroxysuccinimide.
The concentration of serum COX-2 in patients was determined from the standard curve (Fig. 2A) using RU obtained from binding of serum over the COX-2 antibody. One RU corresponds to immobilized protein concentration of 1 pg/mm2 (Kretschmann and Raether, 1968; Otto, 1968; Nylander et al., 1982).

Figure 2B shows the concentration of COX-2 for all 84 patients and normal individuals. The serum COX-2 levels of the patients with breast cancer included in the study (Mean ± SD = 14.55 ± 5.74 μg/mL) was almost fivefold higher (p < 0.0001) than healthy subjects (Mean ± SD = 3.5 ± 1.3 μg/mL) (Fig. 2C).
Serum COX-2 levels were significantly higher, 17.5 ± 4.7 μg/mL (p < 0.0061), in patients with lymph node involvement (N+) as compared to those with no lymph node metastasis (N0), 13.5 ± 3.7 μg/mL (Fig. 3A).
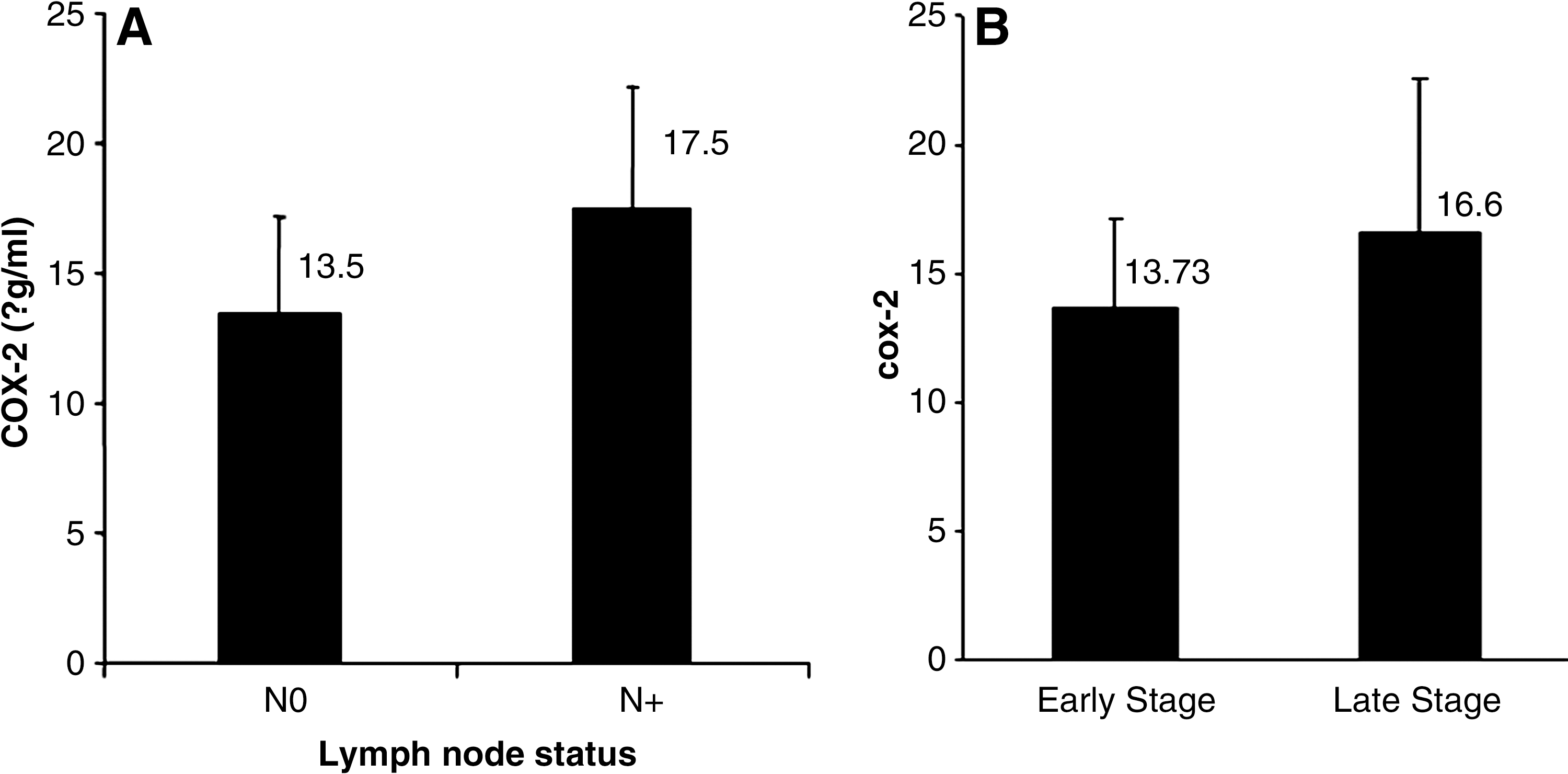
COX-2 levels were found to be significantly higher (p < 0.015) with increasing tumor stage. The mean ± SD level was 13.73 ± 3.4 μg/mL for patients with early stage (stage I+II) breast cancer and 16.6 ± 6.02 μg/mL for patients with late stage (stage III) breast cancer (Fig. 3B).
Serum COX-2 level in relation to tumor size was analyzed by classifying the patients according to small tumor size (T1+T2) and large tumor size (T3). No significant difference in circulating COX-2 levels was observed in patients with small and large size tumors (15.08 ± 4.8 μg/mL vs. 14.07 ± 6.5 μg/mL; p = 0.24).
Patients with breast cancer were grouped according to their ER, PR, and HER2 positivity. As shown in Table 1, the circulating levels of COX-2 did not show any correlation with the ER, PR, or HER2 status of the patients, though an increasing trend was seen in patients with HER2 positivity.
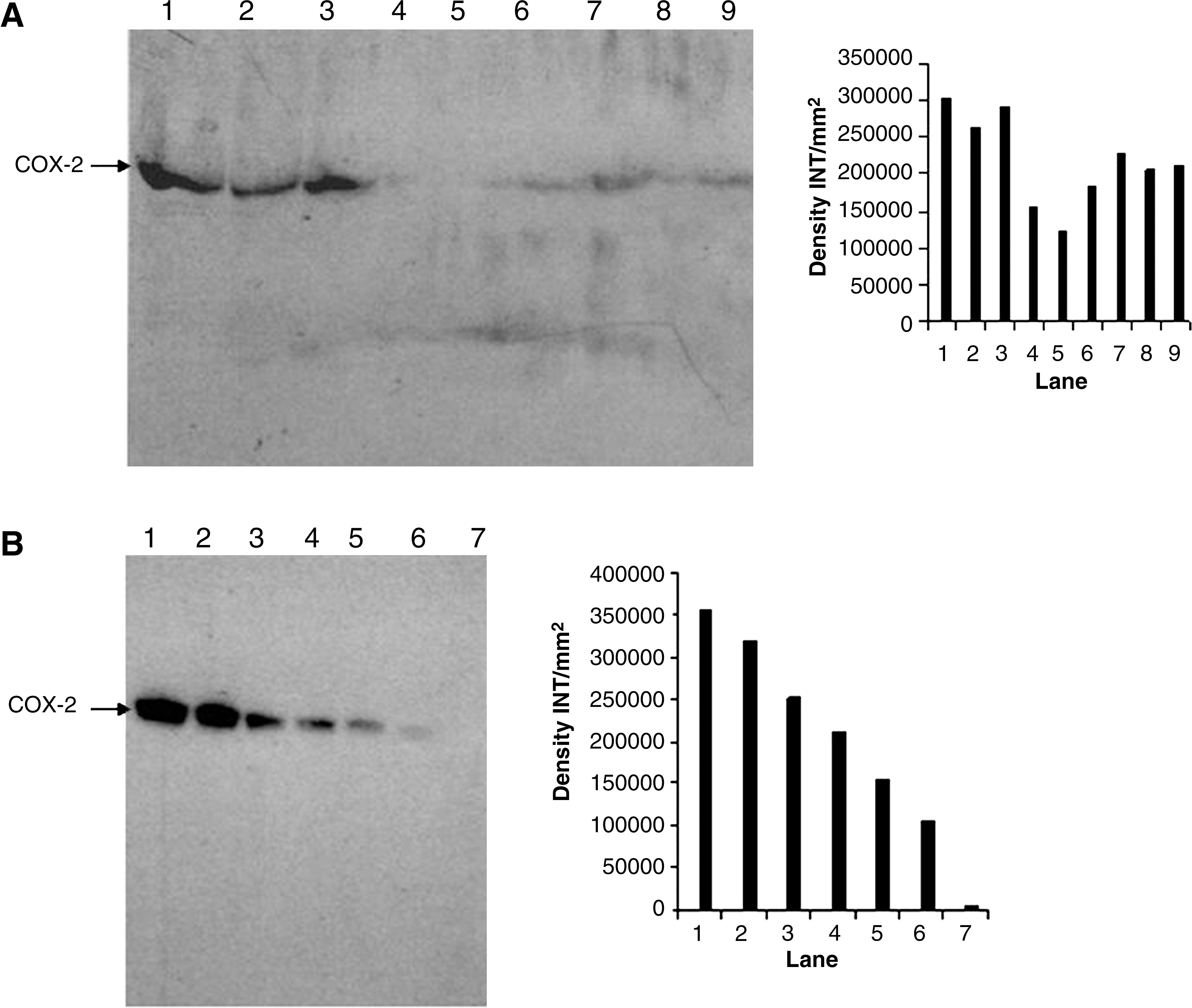
Western blot to confirm the presence of COX-2 in serum
To confirm the presence of COX-2 in serum, western blot analysis was performed with three randomly selected patients' serum samples collected before and after chemotherapy and three control samples. Figure 4A shows the progression and decline of COX-2 in patients with breast cancer compared with normal individuals. The linearity of the reactivity and specificity of the COX-2 antibody is illustrated in Figure 4B.
Effect of chemotherapy on COX-2 expression
Patients with breast cancer were divided into two groups based on the treatment modality: those receiving chemotherapy before surgery (neo-adjuvant chemotherapy) and those receiving chemotherapy after lumpectomy or mastectomy (adjuvant chemotherapy). Out of the 84 patients, 48 patients were in the neo-adjuvant chemotherapy group, and 36 patients received adjuvant chemotherapy.
Out of 48 neo-adjuvant cases, a significant decrease in the levels of COX-2 after each cycle of chemotherapy was observed in 33 patients (68.75%), especially those who were clinically responsive. This trend was not observed in 15 (31.25%) nonresponders. The mean ± SD prechemotherapy COX-2 levels were 14.55 ± 5.6 μg/mL, whereas the postchemotherapy levels at the end of the second cycle of chemotherapy (after 42 days) were 8.87 ± 3.97 μg/mL, which is highly significant (p < 0.0025) (Fig. 5).
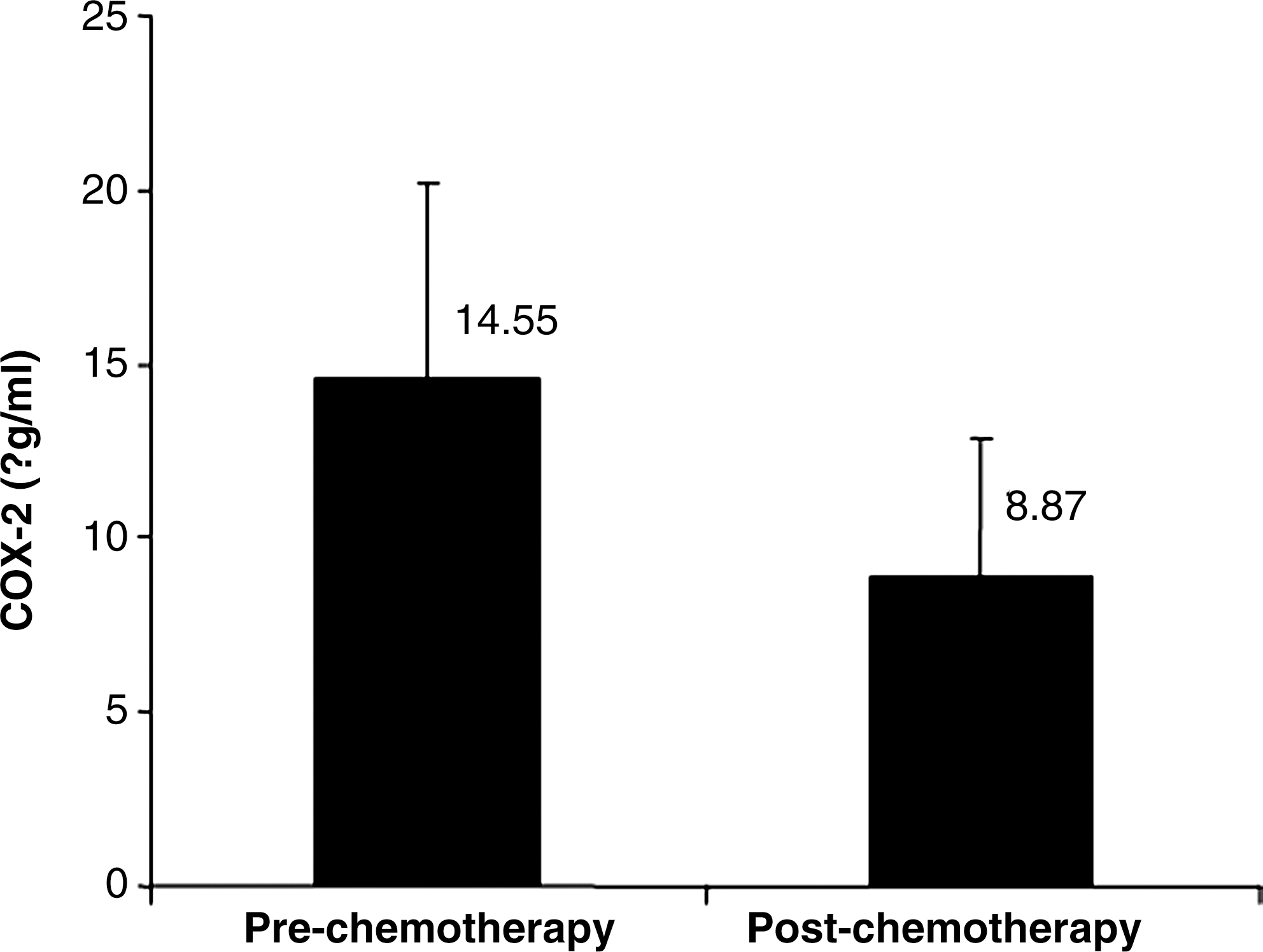
Effect of neo-adjuvant chemotherapy on serum COX-2 level.
In the case of 36 adjuvant patients, the level of COX-2 was significantly reduced after surgery (presurgery = 15.15 ±5.89 μg/mL whereas postsurgery = 10.07 ± 3.5 μg/mL).
The COX-2 levels in cancerous tissue ranged from 14.03–24.35 μg/mL with a mean ± SD of 16.03 ± 3.08 μg/mL, whereas the normal tissue levels were in the range of 8.92–12.85 μg/mL (9.84 ± 2.85), which was very significant (p < 0.0001).
Discussion
The over expression of COX-2 was first reported in colorectal carcinoma and adenomas (Andrew et al., 2007, 2009); however, now it has been detected in various human cancers including breast cancer. The over expression of COX-2 increases the level of PG, which has been observed in cancer. In breast tissue, PG may also stimulate proliferation indirectly by increasing estrogen biosynthesis (Harris et al., 1999). COX-2 over expression may lead to DNA damage, thereby contributing to carcinogenesis.
In the present study, the age of the patients ranged from 22–67 years (mean ± SD = 43.81 + 9.94). a majority of patients were in the age group of 40 years and above with the incidence being lowest in the age group of 20–30 years. The age distribution showed higher incidence with increasing age that peaks in the 40–50 year age group, which is similar to other studies (Brinton et al., 1979). This may be attributed to hormonal factors as reported earlier (Weiss et al., 1999). The size of the tumor influences prognosis or 5 years survival in patients with breast cancer. The smaller the size, the higher is the incidence of 5-year survival and vice versa (Berg and Robbins, 1966). In patients with breast cancer, tumor tissues exhibited significantly higher levels of COX-2 as compared with normal breast tissue (Jiang et al., 2003). Similarly, COX-2 over expression was also associated with indicators of breast cancer development, such as lymph-node metastasis and large tumor size (Denkert et al., 2004).
The correlation of COX-2 expression and clinical course of breast cancer, however, is inconclusive. Zhao et al. (2008) examined COX-2 mRNA in 13 human breast tumors with no detectable expression. Hwang et al. (1998) found only 2 out of 44 patients with tumor expressing COX-2. Cejas et al. (2005) found that COX-2 mRNA and protein were over expressed in nontumor ductal epithelium as compared with invasive ductal carcinoma. Similarly, COX-2 expression was decreased in a breast cancer cell line and immortalized human mammary epithelial cells and cancer specimens as compared with normal mammary epithelial cells (Zhao et al., 2008). The expression of COX-2 mRNA is significantly higher in estrogen receptor negative tumors compared with the receptor positive group, but no correlation with tumor size, nodal status, and presence of vascular invasion was observed (McCarthy et al., 2006). COX-2 was suggested as a marker of precursors and risk of breast cancer (Shim et al., 2003; Crawford et al., 2004). However, Zhao et al. (2008) showed that COX-2 expression does not predict a breast cancer precursor cell.
Rozenowicz et al. (2010) observed no association of COX-2 with response to neo-adjuvant chemotherapy by immunohistochemistry. However, we observed a significant association of COX-2 with response to neo-adjuvant chemotherapy by real-time SPR. The level of COX-2 in serum was found to be higher before chemotherapy, and it continuously decreases with each neo-adjuvant chemotherapy cycle. SPR is a very sensitive technique that can detect the protein concentration in picogram quantity. The patients whose level of COX-2 was declining with chemotherapy and having ER+ tumor were also the ones responding clinically. The level was also high in stage III compared with early stages. The patients had a very high level of COX-2, which abruptly decreased after removal of the tumor by surgery.
It can be concluded by comparing the results of normal patients and those with cancer at different stages that the expression level of COX-2 increases significantly with the progression of breast cancer. A gradual decrease in the serum COX-2 levels was observed in patients undergoing neo-adjuvant chemotherapy treatment. COX-2 can be used as a prognostic molecule for the detection of the disease in the early stage of breast cancer. The advantage of SPR technology over western blot for determining the serum COX-2 level is the real-time analysis with the use of a label-free antibody. Although SPR has been widely employed for antigen-antibody interaction in various settings, this study co-related the effect of chemotherapy on breast cancer progression by demonstrating a decline in serum COX-2 level by this technology. This decrease in expression of COX-2 after chemotherapy is due to the inhibition of DNA and RNA synthesis. SPR technology can also set a platform for widespread use and better correlating the COX-2 levels in different stages in breast cancer.
Footnotes
Acknowledgments
The authors acknowledge financial support from the Council of Scientific and Industrial Research and Indian Council of Medical Research, Government of India.
Disclosure Statement
No competing financial interests exist.