
Abstract
Chlamydial infection of the lower genital tract usually spreads to the upper genital tract and is then responsible for more serious consequences, such as infertility, ectopic pregnancy, pelvic pain, and pelvic inflammatory disease. Genital infection with Chlamydia trachomatis and the resulting cytokine response largely determines the outcome of infection and disease. To date, studies showing comparative effects of azithromycin and doxycycline treatment for C. trachomatis infection in women with reproductive sequelae like infertility and their effect on immune molecules like cytokines are lacking. Hence, our objective was to study the effect of azithromycin and doxycycline in vitro on cytokines in cells from C. trachomatis–positive fertile and infertile women as well as their efficacy in C. trachomatis infection. Fertile and infertile women with primary and recurrent C. trachomatis infection attending the gynecology outpatient department of Safdarjung Hospital, New Delhi, India, were enrolled. Enzyme-linked immunosorbent assay and real-time reverse transcription–polymerase chain reaction was performed for evaluating cytokines in cells stimulated with chlamydial elementary bodies (EBs) in the presence and absence of antibiotics (azithromycin and doxycycline). C. trachomatis–infected women were also followed up to assess the efficacy of azithromycin and doxycycline. We observed inhibition of cytokines (interleukin [IL]-1beta (β), IL-6, IL-8, IL-10, and tumor necrosis factor-alpha) in the presence of azithromycin in EB-stimulated cells from both fertile and infertile women with primary and recurrent C. trachomatis infection. However, in presence of doxycycline, inhibition of cytokines (IL-1β and IL-6) was only observed in stimulated cells from fertile women with primary C. trachomatis infection. The clinical efficacy of azithromycin was also better than doxycycline in recurrent C. trachomatis infection in women with complications such as infertility. Overall, this study suggests that azithromycin treatment with broader immunomodulatory effects may be preferable to doxycycline for the treatment of recurrent C. trachomatis infection associated with infertility.
Introduction
The specific balance between pro-inflammatory and anti-inflammatory cytokines at the site of inflammation influences tissue damage (Debattista et al., 2003; Kinnunen et al., 2003; Stephens, 2003; Hafner et al., 2008; Srivastava et al., 2008; Darville and Hiltke, 2010). Chlamydial infections are usually treated with azithromycin or doxycycline. Although several studies have shown satisfactory results in acute infections (Ossewaarde et al., 1992; Thorpe et al., 1996; Sendag et al., 2000), in chronic infections, treatment is less satisfactory (Oriel, 1982). In a study by Tuffrey et al. (1994) single-dose oral azithromycin therapy was found to prevent infertility in a mouse model of chlamydial salpingitis. Similarly, azithromycin was found to be more effective than doxycycline in treating C. trachomatis infection and prevention of immunopathological upper reproductive tract damage in a macaque model of PID (Patton et al., 2005). In our previous study, we have shown that azithromycin provides anti-inflammatory effects by inhibiting cytokine production in cervical secretions from women infected with C. trachomatis (Srivastava et al., 2009). Previous studies suggest that azithromycin and doxycycline are equally efficacious in chlamydial cervical infection; however, human studies for their effect on the long-term sequelae of chlamydial infections are limited (Patton et al., 1994).
To date, studies showing the comparative efficacy of azithromycin and doxycycline for C. trachomatis infection in women with reproductive sequelae such as infertility and their effect on immune molecules such as cytokines are lacking. Therefore, our objective was to study the effect of azithromycin and doxycycline in vitro on cytokines in cells from C. trachomatis–positive fertile and infertile women as well as their comparative efficacy in C. trachomatis infection.
Materials and Methods
Study population
After obtaining informed written consent, 748 patients attending the gynecology outpatient department, Safdarjung Hospital, New Delhi, India, for gynecological complaints (cervical discharge, cervicitis, and infertility) were enrolled in the study. The study received approval from the ethics review committee of Safdarjung Hospital, New Delhi, India (Srivastava et al., 2009). At recruitment, a detailed clinical questionnaire was administered to each patient for collecting information on reasons for referral, gynecology history, including menstruation, symptoms of genital and urinary tract infection, and obstetric and medical histories. Patients with positive urine pregnancy test were excluded from the study.
Infertile women were identified as those that lack recognized conception after 1.5 to 2 years of regular intercourse without the use of contraception. The infertile group included women with referred diagnostic laparoscopy/hysterosalpingography (Reddy et al., 2004). Women with male factor-related infertility were excluded from the study.
Collection of Samples
The vulva was examined for lesions and vaginal/cervical discharge. The cervix was inspected for ulcers, warts, ectopy, erythema, discharge, or any other abnormalities. After cleaning the endocervix with a cotton swab (Hi Media), endocervical swabs were collected from patients for diagnosis of C. trachomatis and other STD pathogens. Another cotton swab was collected in sucrose phosphate glutamate (SPG) media (pH 7.0) for isolation and propagation of C. trachomatis.
A cytobrush was placed within the endocervical canal so that cells from the endocervical region and the zone between the endocervical and ectocervical regions (transformation zone) could be obtained. All cytobrush samples had negative results for blood contamination. The cytobrush was then held in a sterile centrifuge tube containing phosphate-buffered saline (PBS). Two milliliters of nonheparinized blood was collected for separating serum.
Culture of cervical mononuclear cells
Cervical mononuclear cells were isolated and counted as described earlier (Srivastava et al., 2008). The cells were washed three times with PBS and suspended in RPMI-1640 (Sigma-Aldrich) containing 5% fetal calf serum (FCS; PAA). Briefly, cells were cultured in round-bottomed 96-well plates (5×104 cells/well) in a total volume of 200 μL and subsequently stimulated with inactivated C. trachomatis serovar D (a human clinical genital isolate) elementary bodies (EBs) at multiplicity of infection (MOI) 2 in the presence and absence of azithromycin (Sigma-Aldrich; 2 μg/mL) or doxycycline (Sigma-Aldrich; 5 μg/mL) and were incubated in humidified 5% CO2 at 37°C for 72 h (for enzyme-linked immunosorbent assay [ELISA]) and 12 h (for real time reverse transcription-polymerase chain reaction [RT-PCR]). Time points for evaluating cytokines (72 h for ELISA and 12 h for RT-PCR) were found to be optimum as reported earlier (Agrawal et al., 2009; Gupta et al., 2009a, 2009b). Cell viability was examined after isolation of cervical mononuclear cells and at time points 12 h and 72 h using trypan blue staining to ensure that cells were viable during the experiment. Concentrations of the above mentioned antibiotics (azithromycin and doxycycline) were chosen as it has been reported that approximately the same concentrations are present at the site of infection (Whelton et al., 1980; Worm and Osterlind, 1995).
Laboratory diagnosis
Spots were made on glass slides from cervical swab samples. These were stained with fluorescein isothiocyanate (FITC)–conjugated monoclonal antibodies to C. trachomatis major outer membrane protein (MOMP) using MicroTrak C. trachomatis Direct Specimen Test kit according to the manufacturer's instructions. Cervical samples positive/negative by direct fluorescent assay (DFA) were further confirmed by doing PCR analysis as mentioned earlier (Srivastava et al. 2011). Diagnosis for other STD pathogens were done by culture for Neisseria gonorrhoeae, Mycoplasma hominis, Ureaplasma urealyticum, and by microscopy on gram-stained smears for Candida spp., bacterial vaginosis and Trichomonas vaginalis as mentioned earlier (Reddy et al., 2004).
Treatment
Patients found to have C. trachomatis infections were prescribed azithromycin (1 g single dose) or doxycycline (100 mg twice daily for 7 days). Patients with recurrent infection were followed up for 3 months (12 weeks) and checked for C. trachomatis infection each month and, if found positive, the treatment was repeated and the same dose of azithromycin (1 g single dose) or doxycycline (100 mg twice daily for 7 days) was given.
Antibody assay
Sera of patients were assayed for IgG antibodies to C. trachomatis by commercially available ELISA kit (Ridascreen), according to the manufacturer's instructions.
Minimum inhibitory concentration determination
Minimum inhibitory concentration (MIC) was determined by immunofluorescence assay and RT-PCR method. C. trachomatis isolates were propagated in human cervical epithelial adenocarcinoma cell line HeLa 229 cells as described previously (Bhengraj et al., 2010), purified, and stored at −80°C in SPG medium. Fresh monolayers of HeLa cells were prepared by seeding 2×105 cells/well in 24-well tissue culture plate (Nunc) in Eagle's minimum essential medium (HiMedia) supplemented with 10% FCS, 2 mM L-glutamine (Sigma-Aldrich), HEPES buffer (SRL), and 25 mM sodium bicarbonate (Sigma-Aldrich). Before infection, the cell monolayers were washed once with PBS (pH 7.0) and treated with 30 μg/mL DEAE-dextran (Sigma-Aldrich) and incubated at 35°C for 30 min. Chlamydial inoculum was added on to the cell monolayers at an MOI of 1 and incubated for 1h at 35°C. Cells were centrifuged at room temperature for 30 min at 1000 rpm and incubated at 35°C for 2 h. After incubation, inoculum was replaced with twofold serially diluted doxycycline prepared in Dulbecco's modified Eagle's medium (Sigma-Aldrich) supplemented with 5% FCS, and 1 μg/mL cycloheximide (Sigma-Aldrich) and incubated for 48 h in a humidified incubator at 35°C with 5% CO2. As control, infected cells were incubated in the absence of doxycycline.
Immunofluorescence assay
C. trachomatis inclusion bodies were detected by immunofluorescence assay after staining with FITC-labeled monoclonal antibody against C. trachomatis MOMP. The MICs were determined by counting the number of inclusions, the MIC being the lowest concentration of antibiotic with no inclusions visible.
Reverse transcription-polymerase chain reaction
Total RNA was isolated using Trizol reagent (Invitrogen) according to the manufacturer's instructions. Complementary DNA (cDNA) was prepared using a SuperScript™ First-Strand Reverse Transcriptase kit (Invitrogen), in accordance with the manufacturer's instructions. Amplification of cDNA was carried out using the primer sequences of 16S rRNA gene (5′CTGCAGCCTCCGTAGAGTCTGGGCAGTGTC 3′ and 5′TTCAGATTGAACGCTGGCGGCGTGGATG 3′) as described earlier (Bhengraj et al., 2008). The PCR product was visualized by electrophoresis on a 2% agarose gel stained with ethidium bromide. The lowest concentration of antibiotic which inhibited the appearance of a PCR product determined the MIC.
Quantification of cytokines
Interleukin (IL)-1beta (1β), IL-2, IL-4, IL-6, IL-8, IL-10, IL-13, interferon-gamma (IFN-γ), and tumor necrosis factor-alpha (TNF-α) were quantified by commercially available ELISA kits (eBiosciences) in accordance with the manufacturer's instructions.
RNA extraction and real-time RT-PCR analysis for cytokines
Total RNA was isolated using RNeasy Mini Kit (Qiagen) in accordance with the manufacturer's instructions and stored at −80°C. cDNA was prepared using a SuperScript First-Strand Reverse Transcriptase kit (Invitrogen) in accordance with the manufacturer's instructions. Real-time PCR was performed with the DyNAmo™ SYBR® Green qPCR Kit (Finnzymes). Sequences for endogenous control (β-actin) and cytokine genes (IL-1β, IL-2, IL-4, IL-6, IL-10, IFN-γ, and TNF-α) used in this study were same as reported earlier by Jasper et al. (2006). Sequences for IL-8 primers were as mentioned by Hara et al. (2009). All primers were of HPLC-purified grade and were commercially synthesized (MWG-Biotech AG). The negative control included in each reaction consisted of nuclease-free water substituted for cDNA. PCR amplification was performed in an Applied Biosystems 7000 Real-Time PCR System (Applied Biosystems). For data analysis, the 2−ΔΔCt method was used to calculate fold change (Livak and Schmittgen, 2001).
Statistical analysis
Differences between two groups were evaluated using Mann–Whitney U test. p<0.05 was considered significant.
Results
Study population
Cervical C. trachomatis infection was diagnosed by DFA/polymerase chain reaction in 260 patients. Fifty-eight of these were excluded from the study as they were found to be co-infected with either bacterial vaginosis, Candida spp., T. vaginalis, M. hominis, U. urealyticum, or Neisseria gonorrhea in the cervix or had previous history of these infections.
Based on clinical history and diagnosis, the patients were categorized into following groups: Group A comprised of women with primary C. trachomatis infection (n=144) without any records for previous history of chlamydial infections and were also found to be negative for IgG antibodies against C. trachomatis in serum. Group B comprised women having recurrent C. trachomatis infection (n=58) and being tested positive for infection for ≥2 times within a period of ≥3 months after appropriate antibiotic treatment. Further, they were found to be positive for IgG antibodies against C. trachomatis in serum (Agrawal et al., 2007a, 2007b), confirming previous C. trachomatis infection. The median ages of women with primary and recurrent infections were comparable (28 and 30 years, respectively).
Primary and recurrent infection
Group A was further divided into two groups: Group I (n=85) comprised of fertile women and Group II (n=59) comprised of infertile women.
Group B was divided into two groups: Group III (n=20) comprised of fertile women and Group IV (n=38) comprised of infertile women.
Groups I, II, III, and IV were further divided on the basis of antibiotics (azithromycin and doxycycline) given: Group IA comprised C. trachomatis–positive fertile patients who were given azithromycin; Group IB comprised C. trachomatis–positive fertile patients who were given doxycycline. Group IIA comprised C. trachomatis–positive infertile patients who were given azithromycin; Group IIB comprised C. trachomatis–positive infertile patients who were given doxycycline. Group IIIA comprised C. trachomatis–positive fertile patients who were given azithromycin; Group IIIB comprised C. trachomatis–positive fertile patients who were given doxycycline. Group IVA comprised C. trachomatis–positive infertile patients who were given azithromycin; Group IVB comprised C. trachomatis–positive infertile patients who were given doxycycline.
Efficacy of Azithromycin and Doxycycline for C. trachomatis infection in women
Out of 202 C. trachomatis–positive patients, 19 were excluded because other antibiotics were also prescribed to them. Thirty-six patients were lost to follow-up and 12 patients were excluded as the compliance for doxycycline was not 100%. Further, six patients were not included as their partners denied to participate in the study.
In Group A the treatment efficacies for both the antibiotics were similar:
Azithromycin: In Group IA (n=21), 20 were found negative for C. trachomatis after treatment (Table 1). In Group IIA (n=19), 18 were found negative for C. trachomatis after treatment (Table 1).
Group I comprised C. trachomatis–positive fertile women; Group II comprised C. trachomatis–positive infertile women; CT represents Chlamydia trachomatis.
Doxycycline: In Group IB (n=27), 26 were found negative for C. trachomatis after treatment (Table 1). In Group IIB (n=27), 25 were found negative for C. trachomatis after treatment (Table 1).
In Group B the treatment efficacies for both the antibiotics were found to be different:
Azithromycin: In Group IIIA (n=7), four were found negative for C. trachomatis after 4 weeks of treatment and three were found negative for C. trachomatis after 8 weeks of treatment (Table 2). In Group IVA (n=12), five were found negative for C. trachomatis after 8 weeks of treatment and seven were found negative for C. trachomatis after 12 weeks of treatment (Table 2).
Group III comprised C. trachomatis–positive fertile women; Group IV comprised C. trachomatis–positive infertile women.
Doxycycline: In Group IIIB (n=6), one was found negative for C. trachomatis after 4 weeks of treatment, two were found negative for C. trachomatis after 8 weeks of treatment, and three were found negative for C. trachomatis after 12 weeks of treatment (Table 2). In Group IVB (n=10), only two were found negative for C. trachomatis after 12 weeks of treatment (Table 2).
Further, we also evaluated the MIC for the isolates from C. trachomatis–positive women (Group IV) with treatment failure (after 12 weeks of continuous doxycycline treatment) and found all were susceptible to doxycycline in vitro. The results of in vitro susceptibility testing against representative isolates are summarized in Table 3.
Group IV comprised C. trachomatis–positive infertile women.
MIC, minimum inhibitory concentration; IF, immunofluorescence; RT-PCR, reverse transcription–polymerase chain reaction.
Quantification of cytokines by ELISA
Out of 202 C. trachomatis–positive patients, 75 were excluded, as either the count of mononuclear cells in the cervical cells was too low or epithelial cells were present.
Group A, comprising women with primary infection, was divided into Group I (n=52; comprising C. trachomatis–positive fertile women) and Group II (n=44; comprising C. trachomatis–positive infertile women). Group B, comprising women with recurrent infection, was divided into Group III (n=17; comprising C. trachomatis–positive fertile women) and Group IV (n=14; comprising C. trachomatis–positive infertile women).
A significant decrease in the IL-1β, IL-6, IL-8, and TNF-α was observed in Group I and Group II in the presence of azithromycin in C. trachomatis–stimulated cells (Table 4). In the presence of doxycycline, a significant decrease in the levels of IL-1β and IL-6 was observed in Group I, whereas a decrease in the levels of IL-1β and IL-6 was also observed in Group II but it was not significant (Table 4). There was no detectable IL-4 level in any culture supernatant (data not shown).
Group I comprised C. trachomatis–positive fertile women; Group II comprised C. trachomatis–positive infertile women; cytokine concentration is denoted by median and range in parenthesis.
Significance level between CT+Azithromycin and CT in Group I.
Significance level between CT+Doxycycline and CT in Group I.
Significance level between CT+Azithromycin and CT in Group II.
Significance level between CT+Doxycycline and CT in Group II.
Significance level.
IL, interleukin; IFN, interferon; TNF-α, tumor necrosis factor-alpha.
A significant decrease in the levels of IL-1β, IL-6, IL-8, IL-10, and TNF-α was observed in Group III and Group IV in the presence of azithromycin in C. trachomatis–stimulated cells (Table 5). In the presence of doxycycline no significant decrease in the levels of cytokines was observed in either group (Table 5). There was no detectable IL-4 level in any culture supernatant (data not shown).
Group III comprised C. trachomatis–positive fertile women; Group IV comprised C. trachomatis–positive infertile women; cytokine concentration is denoted by median and range in parenthesis.
Significance level between CT+Azithromycin and CT in Group III.
Significance level between CT+Doxycycline and CT in Group III.
Significance level between CT+Azithromycin and CT in Group IV.
Significance level between CT+Doxycycline and CT in Group IV.
Significance level.
Cytokine mRNA expression levels
mRNA expression levels for IL-1β, IL-2, IL-4, IL-6, IL-8, IL-10, IFN-γ, and TNF-α were detected in C. trachomatis–stimulated cervical cells in the presence and absence of antibiotics.
In Group A, a significant decrease in mRNA expression levels of IL-1β, IL-6, IL-8, IL-10, and TNF-α was observed in Group I and Group II in the presence of azithromycin, whereas only decrease in IL-1β and IL-6 mRNA expression levels was observed in Group I and none in Group II in the presence of doxycycline (Fig. 1).
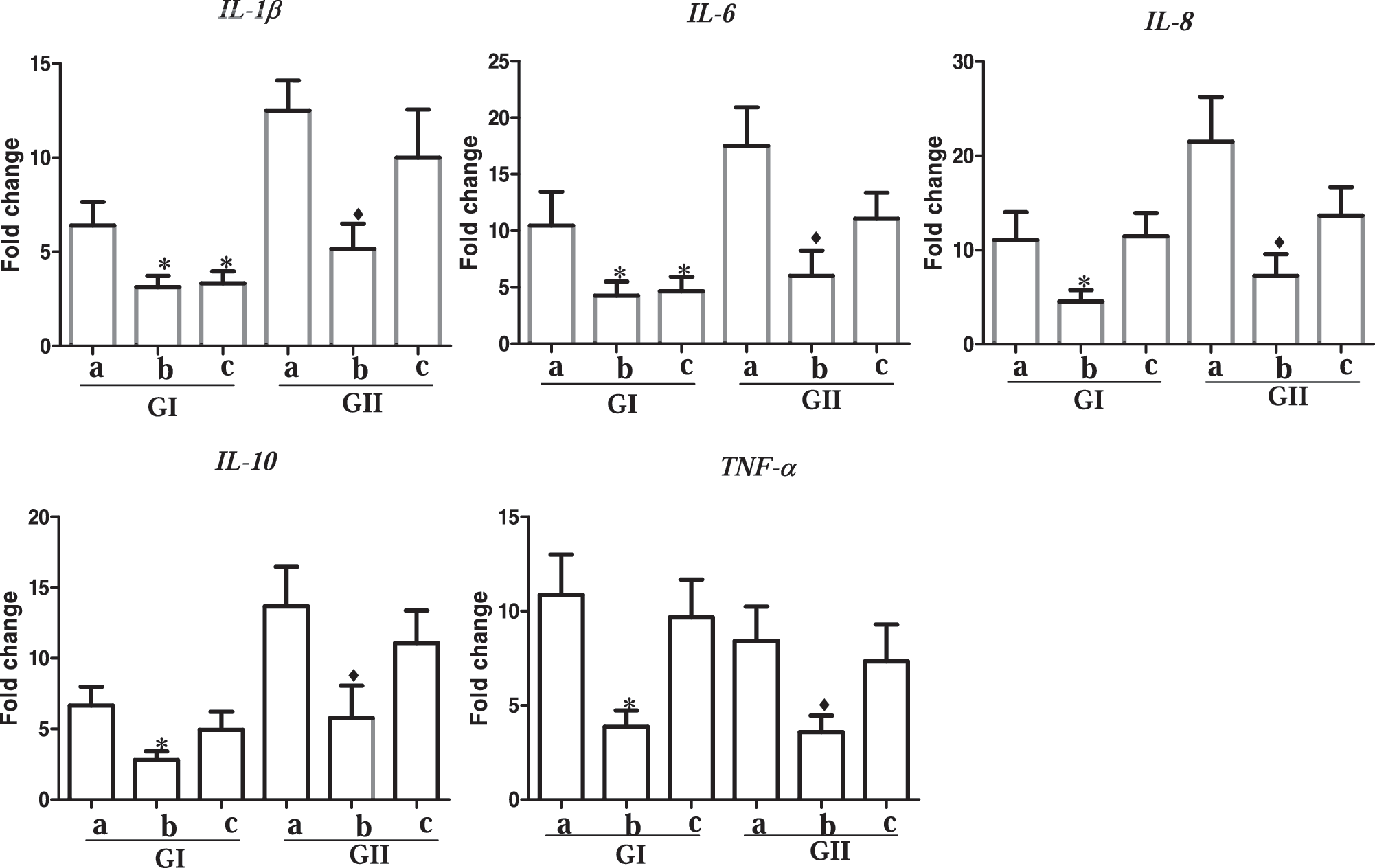
Estimation of mRNA expression of cytokines upon Chlamydia trachomatis EBs stimulation in the presence and absence of azithromycin and doxycycline in cervical cells obtained from women with primary infection. Real-time RT-PCR analysis of mRNA levels was done, where Group I comprised of C. trachomatis–positive fertile women and Group II comprised of C. trachomatis–positive infertile women. “a” represents C. trachomatis EB's; “b” represents C. trachomatis EB's+azithromycin; “c” represents C. trachomatis EB's+doxycycline. All cytokines were normalized against corresponding levels of endogenous β-actin. The graph show results as fold change represented by bars. Bars represent mean±SEM for all experiments. * represents p<0.05 as compared to “a” in Group I. ♦ represents p<0.05 as compared to “a” in Group II. EB, elementary body; RT-PCR, reverse transcription-polymerase chain reaction.
In Group B, a significant decrease in mRNA expression levels of IL-1β, IL-6, IL-8, IL-10, and TNF-α was observed in Group III and Group IV in presence of azithromycin, whereas no decrease in mRNA expression levels was observed in both Group III and Group IV in the presence of doxycycline (Fig. 2).
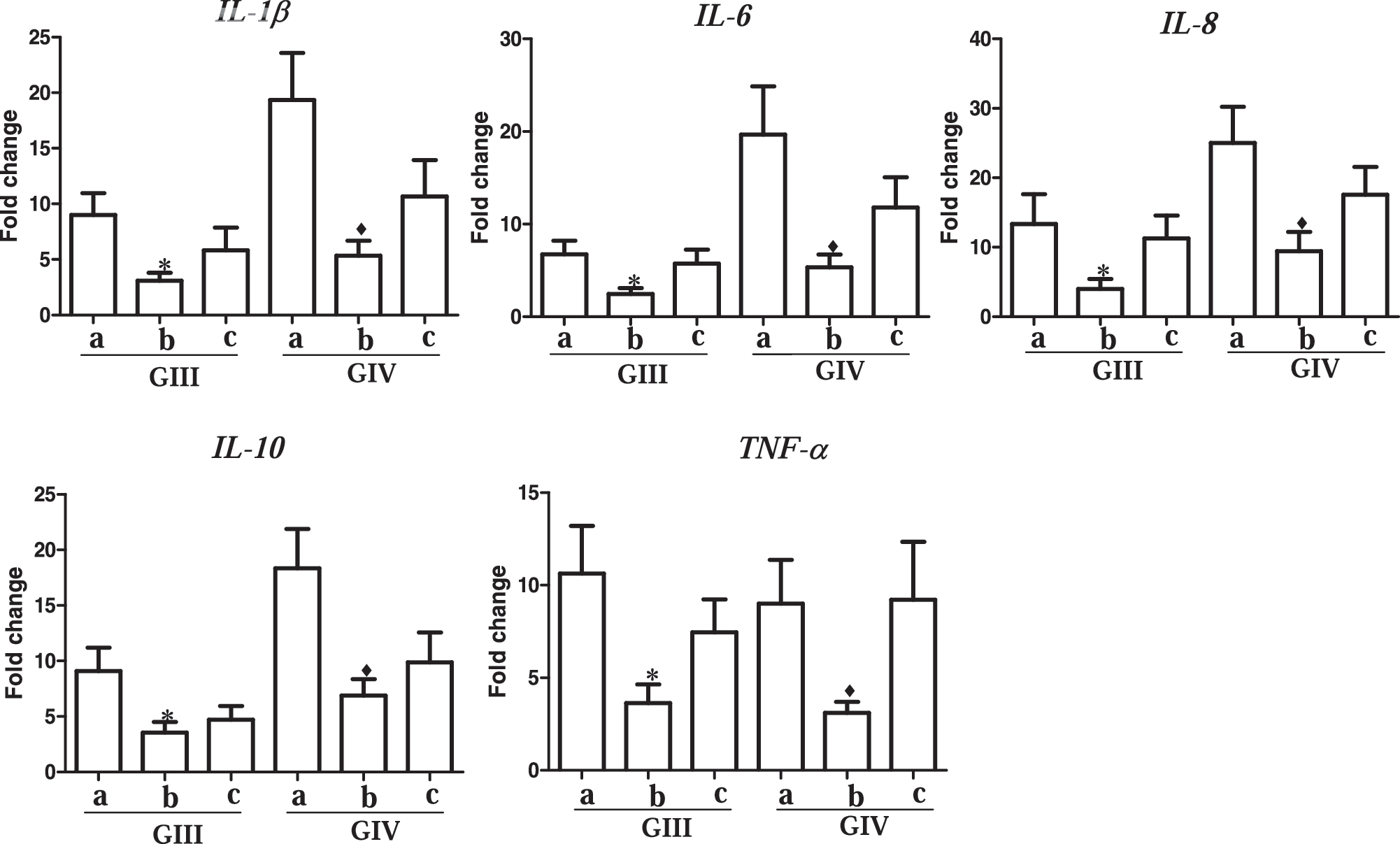
Estimation of mRNA expression of cytokines upon C. trachomatis EBs stimulation in the presence and absence of azithromycin and doxycycline in cervical cells obtained from women with recurrent infection. Real-time RT-PCR analysis of mRNA levels was done, where Group III comprised of C. trachomatis–positive fertile women and Group IV comprised of C. trachomatis–positive infertile women. “a” represents C. trachomatis EB's; “b” represents C. trachomatis EB's+azithromycin; “c” represents C. trachomatis EB's+doxycycline. All cytokines were normalized against corresponding levels of endogenous β-actin. The graph show results as fold change represented by bars. Bars represent mean±SEM for all experiments. * represents p<0.05 as compared to “a” in Group III. ♦ represents p<0.05 as compared to “a” in Group IV.
Discussion
Epidemiological and animal model studies suggest that sequelae of genital chlamydial infection are more associated with second or subsequent infections than to initial infection (Beatty et al., 1994; Hillis et al., 1997; Van Voorhis et al., 1997). In our study, we have observed that continuous treatment of azithromycin for 2–3 months in infertile women with recurrent infection is better for the treatment of C. trachomatis infection, whereas no such effect was observed with doxycycline treatment. Tuffrey et al. (1994) had suggested that in the mouse model of chlamydial salpingitis, azithromycin treatment prevents chlamydial-induced infertility by reducing ultrastructural damage to the epithelium of the oviduct lumen. Further, Patton et al. (2005) had shown azithromycin to be more effective than doxycycline in treating C. trachomatis infection and the prevention of immunopathological upper reproductive tract damage in a macaque model of PID. In an in vitro study Reveneau et al. had suggested that azithromycin would be efficacious against persistent chlamydial infection. In contrast, doxycycline may not be as effective in treating persistent infection (Reveneau et al., 2005). Katz et al. (1991) had compared treatment for 7 days of tetracycline (500 mg) four times daily with a 21-day regimen in C. trachomatis–infected patients and suggested that a longer regimen may not be more efficacious. We further evaluated the MIC values for the isolates obtained from doxycycline treatment failure cases and found all eight isolates were susceptible to doxycycline. Dean et al. (2000) also reported that isolates from persistently infected women were susceptible to antibiotics in vitro but were not treated clinically. This suggests that doxycycline was not effective in vivo for recurrent C. trachomatis infection in chronic condition such as infertility. Overall, it suggests that azithromycin treatment may be more efficacious as compared to doxycycline for recurrent C. trachomatis infection in women with complications such as infertility.
In the present study we have also observed that azithromycin inhibits cytokines (IL-1β, IL-6, IL-8, IL-10, and TNF-α) in EB-stimulated cells obtained from both fertile and infertile women having primary or recurrent C. trachomatis infection. However, in the presence of doxycycline inhibition of cytokines (IL-1β and IL-6) were only observed in stimulated cells from fertile women with primary C. trachomatis infection. Genital infection with C. trachomatis and the resulting cytokine environment largely determines the outcome of infection and disease (Stephens, 2003). IL-1 has been suggested to act as the initiator of fallopian tube destruction during C. trachomatis infection (Hvid et al., 2007). Previous study suggests that IL-6 levels were increased in silent tubal C. trachomatis infections (Li and Liang, 2000). Elevated IL-6 production has been reported in the fallopian tubes of macaques after repeated infection with C. trachomatis (Van Voorhis et al., 1997). Bianchi et al. (1997) had shown increased level of IL-8 after C. trachomatis infection in U937 cells and suggested that IL-8 may play an important role in the inflammatory reaction to chlamydial infection. Others also reported elevated levels of IL-8 during C. trachomatis infection (Rasmussen et al., 1997; Buchholz and Stephens, 2006). IL-10 has been shown to be unfavorable for the protective immunity and control of Chlamydia infection (Yang et al., 1999). In addition, the production of IL-10 has been associated with severe pathological conditions in C. trachomatis infection (Reddy et al., 2004; Srivastava et al., 2008). Darville et al. had shown that in the mouse genital tract, infertility associated with endometriosis has been shown to be related to the production of TNF-α (Darville et al., 2000). TNF-α was found to be produced in response to chlamydial infection by the human fallopian tube (Ault et al., 1996). Gervassi et al. (2004) had shown that C. trachomatis infection in dendritic cells upregulates IL-1β, IL-6, IL-8, and TNF-α. Further, it has been shown that an elevated level of IL-1β, IL-6, IL-10, and IL-8 by C. trachomatis in cervical cells is associated with pathological conditions like fertility disorder (Agrawal et al., 2009). Macrolide antibiotics are used in the treatment of infections caused by many different pathogens. There is evidence that macrolides can affect the host response to infection by mechanisms that are unrelated to their antimicrobial properties (Labro, 1998; Giamarellos-Bourboulis, 2008; Shinkai et al., 2008; Ribeiro et al., 2009). Macrolides have been shown to inhibit the production of pro-inflammatory cytokines, such as IL-6, IL-8, and TNF-α, by cultured human bronchial epithelial cells (Khair et al., 1995; Kawasaki et al., 1998) and in whole blood (Schultz et al., 1998). Azithromycin has been demonstrated to affect to various degrees production of IL-1β, IL-6, IL-10, and TNF-α by human monocytes (Khan et al., 1999). We recently reported that azithromycin treatment inhibits inflammatory cytokines and chemokines in epithelial cells from infertile women with recurrent C. trachomatis infection (Srivastava et al., 2011). Suzuki et al. showed that pretreating cultured human nasal epithelial cells with macrolides inhibits IL-8 secretion. They observed that the inhibitory effect of IL-8 secretion was more effective against lipopolysaccharide (LPS)-induced secretion than against constitutive secretion; this suggests that macrolides suppress excessive production of IL-8 (Suzuki et al., 1997). Similar findings showing inhibition of cytokines by azithromycin treatment have been reported by others for other cells types (Ikegaya et al., 2009; Meyer et al., 2009).
Tetracyclines have also been shown to have other biological actions independent of their antimicrobial effects (Golub et al., 1998; Griffin et al., 2011). Tetracyclines modulate cytokine secretion by Porphyromonas gingivalis LPS-stimulated whole blood (Cazalis et al., 2009). In addition, doxycycline was shown to inhibit the production of IL-1β in LPS-treated corneal epithelial cultures (Solomon et al., 2000). Doxycycline reduces LPS-induced inflammatory mediator secretion, including IL-1β and IL-6 in macrophage and ex vivo human whole blood models (Cazalis et al., 2008). Doxycycline also suppresses IL-6 during C. trachomatis infection (Ikeda-Dantsuji et al., 2007). Similarly, we have also observed that azithromycin and doxycycline inhibit cytokine production and expression. Cytokines are known targets of macrolides and, in our study, azithromycin inhibits TNF-α, IL-8, IL-1β, IL-6, and IL-10 (all associated with Chlamydia-induced pathological conditions). In the presence of doxycycline, we found that IL-1β and IL-6 (secretion and expression) were decreased only in cells stimulated with EBs from fertile women with primary infection. Hence, in pathological conditions such as infertility or recurrent infection, where exaggerated inflammatory responses have been reported, the ability of azithromycin to inhibit cytokine production may make it a better therapeutic choice compared to doxycycline. Our study indicates that azithromycin possess immunomodulatory activity and inhibits cytokines and thus control inflammatory mediators induced by C. trachomatis at the site of infection.
The intent of the study provides some perspective on the treatment of chlamydial infection in chronic condition such as infertility. This study suggests that azithromycin treatment with broader immunomodulatory effects may be preferable to doxycycline for the treatment of recurrent C. trachomatis infection associated with infertility. However, as a limitation of the study we would like to mention that long term follow-up studies are required to evaluate if azithromycin with its antibacterial property as well as its immunomodulatory property of inhibiting cytokines (associated with pathological condition) will help in cure of infertility (i.e., leading to pregnancy) in C. trachomatis–infected women. Our findings could have important implications in the management of human chlamydial infections.
Footnotes
Acknowledgments
We thank Mrs. Madhu Badhwar, Mrs. Asha Rani, and Mrs. Rosamma Thomas for providing technical assistance. This study was supported by a grant from the Indian Council of Medical Research, India. We also acknowledge the Indian Council of Medical Research for providing financial assistance to Pragya Srivastava, Hem Chandra Jha, Harsh Vardhan, and Rajneesh Jha in the form of a research fellowship. University Grants Commission, India, is acknowledged for providing research fellowship to Apurb Rashmi Bhengraj.
Disclosure Statement
No competing financial interests exist.