
Abstract
Thrombospondin-1 plays an important role in cancer development and progression. This study investigated if a correlation exists between single-nucleotide polymorphisms (SNPs) in the Thrombospondin-1 gene (THBS1) and gastric cancer. We conducted a case–control study on a randomly recruited population of 283 patients and 283 healthy individuals from the city of Fuzhou in Southeast China. Individuals were genotyped for four SNPs (rs1478604 A>G, rs2228261 C>T, rs2292305 T>C, and rs3743125 C>T) in THBS1 using matrix-assisted laser desorption/ionization time-of-flight mass spectrometry. THBS1 genotypic distributions between the case and control groups were tested for correlations with cancer development. Comparisons between the case and control groups showed no significant differences in the genotypic distributions of rs1478604 A>G, rs2228261 C>T, and rs3743125 C>T. However, we found a statistically significant association between homozygous CC of THBS1 rs2292305 T>C and development of highly differentiated carcinoma (HDC). The rs1478604 A>G variant was found to be associated with invasion and lymph node metastasis in gastric cancer. After logistic regression and stratification analysis, rs1478604 A>G was more strongly associated with lymph node metastasis in HDC gastric cancer. The power to detect an effect for rs1478604 A>G in HDC was 90%. These findings indicate that the THBS1 rs1478604 A>G variant is linked with differential risks for gastric cancer nodal metastasis. These results support further investigation of THBS1 as a potential therapeutic target in gastric cancer.
Introduction
Thrombospondin-1 (THBS1) is a large multifunctional matrix glycoprotein that has potent anti-angiogenesis activity. It is believed to be involved in regulation of cell adhesion, proliferation, and mobility (Sargiannidou et al., 2001; Lawler, 2002). In vitro and in vivo studies have shown that THBS1 plays an important role in cancer development and progression (Hawighorst et al., 2002; Kazerounian et al., 2008). THBS1 expression in gastric cancer is associated with vascular endothelial growth factor, microvessel density, and transforming growth factor beta expression, and is also an independent prognostic factor for better survival in advanced gastric cancer patients (Nakao et al., 2011). However, genetic evidence for its role in cancer is lacking.
THBS1 is 16.39 kb gene located on chromosome 15q15. In recent years, several studies have shown that THBS1-associated single-nucleotide polymorphisms (SNPs) are correlated with a wide range of diseases (Hannah et al., 2003; Stenina et al., 2004, 2007; Valdes et al., 2005; Zwicker et al., 2006; Sfar et al., 2009). Several studies have investigated whether an association between THBS1 SNPs and a risk of developing cancer exists, (i.e., prostate cancer and colorectal cancer), but the results have been inconsistent (Sfar et al., 2007, 2009; Forsti et al., 2010); its association, if any, with the development and clinicopathological features of gastric cancer is not known. We conducted a case–control study to evaluate if a correlation exists between THBS1 SNPs and risk of gastric cancer in a Southeast Chinese population. The results show that THBS1 rs1478604 A>G within the 5-untranslated region (UTR) of the gene is associated with lymph node metastasis of gastric cancer in a Southeast Chinese Population.
Materials and Methods
Study population
The study population consisted of 283 primary gastric cancer patients and 283 cancer-free people. All subjects were genetically unrelated ethnic Han Chinese and came from the city of Fuzhou and the surrounding regions in Fujian Province in Southeast China. The case population was drawn from archived patients who had been diagnosed with primary incident gastric cancer and were recruited between July 2004 and August 2008 at the Fujian Provincial Cancer Hospital and the Affiliated Hospitals of Fujian Medical University. No patients had received chemotherapy or immunotherapy before surgery. The diagnosis for each case was histopathologically confirmed and clinicopathological data were obtained after histopathological examination. Histological classification of gastric cancer was evaluated according to Lauren's criteria (Lauren, 1965). Patients were staged according to the tumor-node-metastasis (TNM) staging system of the American Joint Commission on Cancer (AJCC). 283 cancer-free controls were randomly selected from a pool of healthy volunteers that had been declared healthy after a routine medical check and did not have a history of personal or familial malignancy or other serious diseases during the same period. The control subjects were gender (1:1) and age (±5 years) matched to the cancer cases. The study was approved by the Institutional Review Board of Fujian Medical University or the Fujian Provincial Tumor Hospital. Informed consent was obtained from each participant.
SNP selection
Tag SNPs were selected using the SNP tagger from the HapMap Phase II data. Polymorphisms were selected by searching the Han Chinese data available from the HapMap Project (International HapMap Consortium, 2003) using the Tagger program (de Bakker et al., 2006). About 207 SNPs were identified in the THBS1 gene region (16.39 kb on chromosome 15 spanning the THBS1 coding region, introns, plus upstream/downstream UTRs), based on sequencing 45 individuals of Han Chinese descent in China. Six tagging SNPs (tagSNPs) were chosen for genotyping, based on three criteria: SNP minor allele frequency >5% genotype correlation; an r 2 threshold of 0.80 in each bin grouped by the linkage disequilibrium (LD)-select algorithm (Carlson et al., 2004); and potential functional significance. When multiple possible tagSNPs were available for a given bin, SNPs were selected in the following order according to their location in THBS1: coding region, 5′-or 3′- UTR region and intronic region. Of the six tagSNPs identified, two were not included in this analysis; rs2236741 was excluded after it showed no variation in early genotyping results and rs2292304 was excluded as a result of assay failure. The four remaining tagSNPs include rs1478604 A>G in the 5′-UTR; rs2228261 C>T in exon 9; rs2292305 T>C THBS1 A523T in exon 10; and rs3743125 C>T in the 3′-UTR.
Matrix-assisted laser desorption/ionization time-of-flight mass spectrometry genotyping
Venous blood samples (5 mL) were collected from each of the case controls. Genomic DNA was extracted from the cell pellets obtained from whole blood using the Blood Genomic DNA Extraction kit (TaKaRa) and stored at −20°C until genotypic analysis was conducted. DNA from gastric cancer patients was isolated from paraffin-embedded normal stomach tissue adjacent to the tumor site (distance >5 cm). DNA was isolated using standard proteinase K-phenol/chloroform ethanol extraction methods. DNA concentrations were measured using ultraviolet spectrophotometry (Eppendorf Biophotometer) at 260 nm. DNA quality was determined by the A260/A280 ratio.
The selected THBS1 SNPs were genotyped using matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS; Sequenom); analyses were done according to Justenhoven et al. (2004). The polymerase chain reaction (PCR) primers used for this experiment are shown in Supplementary Table S1 (Supplementary Data are available online at
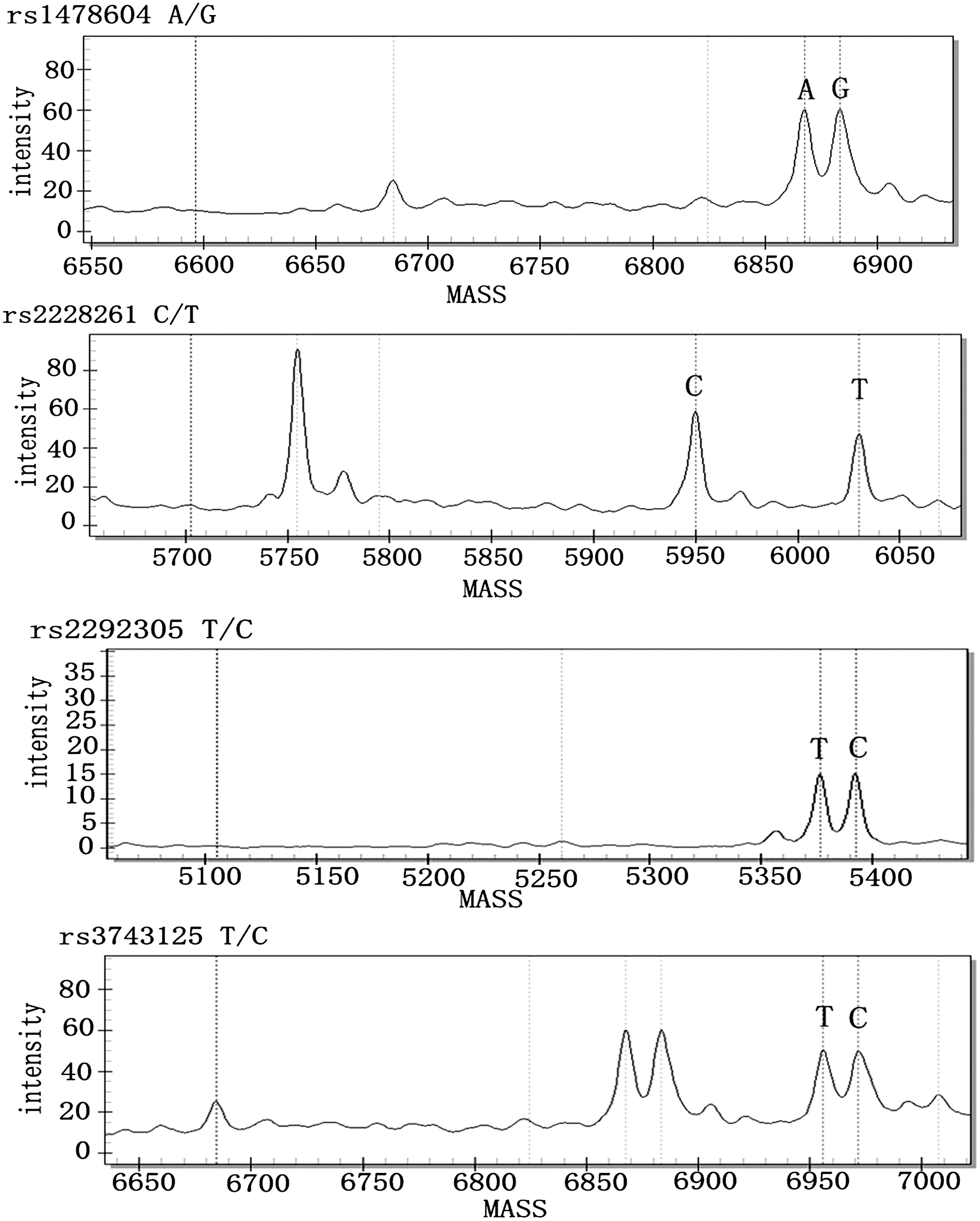
Matrix-assisted laser desorption/ionization time-of-flight mass spectrometry analysis for THBS1 SNPs. SNPs, single-nucleotide polymorphisms.
Genotyping was done in a blinded fashion and the patient and normal control samples were assayed in batches with a negative control consisting of a reaction containing no DNA. A random sample containing 10% of the reaction volume was tested in duplicate by different researchers. Genotyping reproducibility was 100%.
Statistical analyses
Univariate analysis was done using a χ 2 test (or Fisher's exact test when required). These tests included evaluation of the association of genotypic distributions with the development of gastric cancer and with clinicopathological features, including, sex, tumor size, and the status of the lymph node metastasis. The analysis of differences in the features expressed by ordinal variables (e.g., age, differentiation or depth of invasion) was done using the Wilcoxon rank sum test χ 2 test for trend. Multivariate analyses, including testing for the association of THBS-1 genotypes with metastasis, were estimated using logistic regression (forward likelihood ratio, unconditional) or by stratification (overall odds ratio [OR], as estimated by the Mantel-Haenszel method; p for the difference in ORs between strata was calculated using Woolf's χ 2 test). Several clinicopathological variables were also dichotomized to avoid the loss of statistical power in the logistical regressions. All statistical analyses and computation of ORs and 95% confidence intervals (95% CI) were conducted using the Statistical Package for the Social Sciences (version 11.5.0). Estimates of linkage disequilibrium (r 2 and D′) between controls and case sample SNPs were defined using SHEsis software (Li et al., 2009). Haplotypes were estimated using the Expectation Maximization algorithm. Haplotype association with gastric cancer was tested using SHEsis. Rare haplotypes (<3%) were excluded from the analysis (Li et al., 2009). After running the G* Power program (Faul et al., 2007), we estimated a power of at least 0.74 for the whole sample (H0 set at 0.05 and an error rate set at 0.01) and obtained an OR of >2.0.
Results
General characteristics of the subjects enrolled in the study
A total of 283 gastric cancer patients and 283 healthy controls were enrolled into the study. All of the subjects were ethnic Han Chinese. Demographic and other specific characteristics of the cases and controls are presented in Supplementary Table S2. The case group included 102 highly differentiated carcinomas (HDC) (comprising 2 well- and 100 moderately-differentiated cases) and 181 low-differentiated carcinomas (LDC) (comprising 22 moderately-poorly differentiated, 127 poorly-differentiated adenocarcinomas, and 32 diffuse type carcinomas). Neither cases nor controls showed statistically significant differences with regard to sex and age. Tumor stage was determined according to the TNM staging system of the AJCC. Sixty-two (22%), 79 (28%), and 121 (43%), were in stage I, II, and III, respectively. Only 21% or 7% of the patients were in stage IV. The histological grade of gastric cancer, as determined according to Lauren's criteria (Lauren, 1965), was the intestinal type in 124 or 44% of cases, whereas the diffuse-type was present in 159 (56%) of patients.
Association of THBS1 polymorphisms with development of gastric cancer
About 283 patients with gastric cancer and 283 controls were THBS1 genotyped at positions rs1478604 A>G, rs2228261 C>T, rs2292305 T>C, and rs3743125 C>T. Allelic frequencies were calculated and their genotypic distributions tested for Hardy-Weinberg equilibrium. No significant deviations were detected (p=0.77, 0.62, 0.99, and 0.73, respectively). Comparisons between the case and control groups showed no significant differences in the genotypic distributions (Supplementary Table S3), indicating that the polymorphisms were not associated with the development of gastric cancer. However, comparisons between patients with HDC gastric cancer and the control group showed that homozygous CC (rs2292305 T>C) was associated with the development of HDC gastric cancer (odd ratios [ORadjusted] of 2.6, 95% CI of 1.3–5.1, p of 0.02; Table 1, row 3). In contrast, no association between homozygous CC (rs2292305 T>C) and LDC gastric cancer was detected (p=0.97; Table 1, row 4).
Adjusted by age and gender.
OR, odds ratio; CI, confidence interval; HDC, highly differentiated carcinoma; LDC, low-differentiated carcinoma.
Association of THBS1 SNPs with clinicopathologic features of gastric cancer
We looked for associations between the genotypic distributions of THBS1 SNPs and the overall clinicopathological features of the disease. No associations between the rs2228261 C>T and rs3743125 C>T genotypic distribution with the overall clinicopathological features of the patient group were observed (Supplementary Tables S4 and S5).
Association of the rs2292305 T>C genotypic distribution with the overall clinicopathological features of this patient group is presented in Table 2. The frequency of homozygous CC of rs2292305 T>C was significantly different between the HDC and LDC groups (20% vs. 10%, respectively). After adjustment for the patients' gender and age, the risk of developing HDC gastric cancer in those homozygous for CC at position rs2292305 T>C was higher than in those carrying a T allele (CT or TT genotype) (p adjusted=0.03, ORadjusted 2.2, 95% CI of 1.1–4.5). This could indicate that the rs2292305 T>C genotype is only associated with differentiation of gastric cancer.
p-value calculated by comparing CC+CT with TT.
p-value calculated by comparing CT+TT with CC.
Size was determined by measuring the maximum diameter of the tumor.
Within serosa: depth of tumor invasion includes the mucosa, submucosal, and muscularis. Serosa and beyond: depth of tumor invasion includes the serosa and area over the serosa.
Criteria used to determine the stage of gastric cancer differentiation:
HDC represents well-differentiated and moderately well-differentiated stages. LDC represents poorly differentiated stages.
p-Value calculated by comparing CT+TT with CC.
OR was adjusted by age and gender; the adjusted OR and p-values were calculated by comparing CT+TT with CC.
Association of the rs1478604 A>G genotypic distribution together with the overall clinicopathological features of this patient group is shown in Table 3. When comparisons between the depth of invasion were made in the patients, the risk of invasion beyond the serosa in individuals with a G allele (AG or GG genotype) was higher than in individuals carrying the AA genotype (p adjusted=0.004, ORadjusted 2.69, 95% CI of 1.4–5.3). In addition, when comparisons were made within the group that had lymph node metastasis, the risk of metastasis was higher in those carrying a G allele (AG or GG genotype) than those carrying the AA genotype (p adjusted=0.018, ORadjusted 1.90, 95% CI of 1.1–3.3). This could indicate that rs1478604 A>G is only associated with invasion and lymph node metastasis in gastric cancer.
p-Value calculated by comparing AA+AG with GG.
p-Value calculated by comparing AG+GG with AA.
Size was determined by measuring the maximum diameter of the tumor.
Within serosa: depth of the tumor invasion includes mucosa, submucosal, and muscularis. Serosa and beyond: depth of tumor invasion includes serosa and area over the serosa.
p-Value calculated by comparing AG+GG with AA.
OR was adjusted by age and gender; adjusted OR and p-values were calculated by comparing AG+GG with AA.
The criteria used to determine the stage of gastric cancer differentiation: HDC represents well-differentiated and moderately well-differentiated stages. LDC represents poorly differentiated stages.
p-value calculated by comparing AG+GG with AA.
OR was adjusted by age and gender; the adjusted OR and p-values were calculated by comparing AG+GG with AA.
To confirm the results of the logistic regression modeling and analysis of the interaction between factors, we applied stratification to analyze the association of the four THBS1 polymorphisms with the clinicopathological characteristics of the disease. In these tests we used the histological type as the stratification factor. The results are summarized in Table 4. We found that association of the four polymorphisms in THBS1 with lymph node metastasis differed between the two strata. In cases with HDC gastric cancer, after adjustment for the patients' gender and age, all of the following haplotypes were associated with a significantly elevated risk of lymph node metastasis; THBS1 rs1478604 A>G the AG+GG variant genotype, rs2228261 C>T CT +TT variant genotypes, rs2292305 T>C CT+TT variant genotypes, and rs3743125 C>T CT+TT variant genotypes [ORadjusted=4.2 (1.7–10.2), p adjusted=0.001; ORadjusted=2.4, p adjusted=0.04; ORadjusted=2.5, p adjusted=0.04; ORadjusted=2.7, p adjusted=0.02, respectively]. In contrast, in LDC gastric cancer cases, the effect of the four THBS1 polymorphisms on lymph node metastasis was barely detectable (ORadjusted=1.2, p=0.69; ORadjusted=0.73, p adjusted=0.39; ORadjusted=0.84, p adjusted=0.63; ORadjusted=0.79, p adjusted=0.51).
Adjusted by age and gender.
LN, lymph node.
To more accurately evaluate the strength of association of the four polymorphisms with lymph node metastasis in HDC gastric cancer, we examined linkage disequilibrium LD in the case data using SHEsis software to calculate r 2 and D′. Figure 2a shows the pair-wise linkage disequilibrium patterns for the THBS1 gene. We detected an LD between rs1478604 and rs2228261, rs2292305, rs3743125, respectively (D′=0.70, r 2=0.51; D′=0.89, r 2=0.59; D′=0.84, r 2=0.58). We also observed pair-wise LD between rs2292305 and rs2228261 (D′=0.91, r 2=0.63), rs2228261 and rs3743125 (D′=0.86, r 2=0.61), as well as rs2292305 and rs3743125 (D′=0.99, r 2=0.94). The results showed that all SNPs were located in one haplotype block and the genetic variants were in linkage disequilibrium with each other. Figure 2b shows the p-value and OR obtained for rs1478604 A>G, which was higher than rs2228261 C>T, rs2292305 T>C, and rs3743125 C>T (Fig. 2b), indicating that rs1478604 A>G is more strongly associated with lymph node metastasis in HDC gastric cancer.
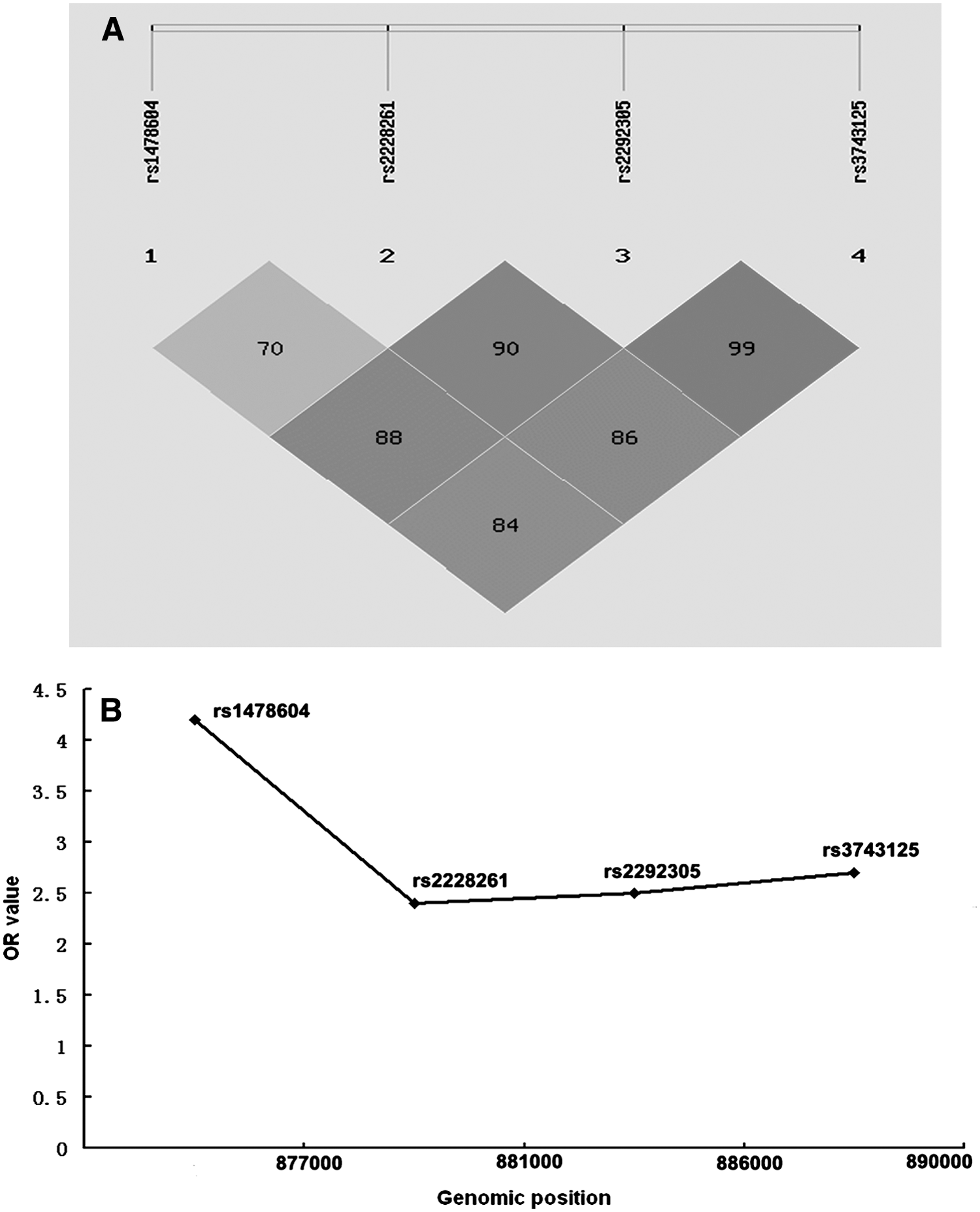
Fine mapping of the THBS1 gene cluster and SNPs associated with metastasis of GC in the HDC group.
Association of THBS1 haplotypes and gastric cancer risk
The haplotypes of the existing four THBS1 SNPs were constructed using SHEsis software. Four major haplotypes (>3% in the control group) were found in both cancer cases and controls. The distributions of the different haplotypes in each group are shown in Supplementary Table S6. No association was found between any of the THBS1 haplotypes and risk of gastric cancer after adjusting for age and gender.
Discussion
The THBS family comprises five proteins involved in the type of tissue remodeling associated with embryonic development, wound healing, synaptogenesis, and neoplasia (Kazerounian et al., 2008). Recent studies have revealed that the expression levels of THBS1, THBS2, and THBS4 are associated with tumor development and progression (Kazerounian et al., 2008; Bai et al., 2009; Chijiwa et al., 2009; Greco et al., 2010; Forster et al., 2011). At the same time, SNPs associated with these genes play an important role in myocardial infarction, coronary artery disease, and premature cardiovascular disease (Stenina et al., 2005, 2007; Koch et al., 2008). Recently, association between THBS1 rs2228262 and risk of prostate cancer has been reported (Sfar et al., 2007, 2009). However, no association has been found between THBS1 rs1478604 A>G and susceptibility to colorectal cancer or its clinical outcome (Sfar et al., 2007, 2009; Forsti et al., 2010). In China, gastric cancer was the most common cancer during the early 1990s (Yang, 2006). Fujian, located in Southeast China, is one of the high-risk areas for gastric cancer (Cai et al., 2003; Wong et al., 2004; Yang, 2006; Zhou et al., 2010). In this study, we investigated whether an association exists between rs1478604, rs2228261, rs2292305, rs3743125 and the development and progression of gastric cancer. Previous studies have shown that elevated THBS1 expression levels are associated with an overall increased incidence of gastric cancer, and overexpression of THBS1 has been reported in a large percentage of gastric cancers (range 38%–85%) (Albo et al., 2002; Zhang et al., 2003; Kim et al., 2006; Lazar et al., 2006; Miyamoto et al., 2007; Kiyono et al., 2009). However, in this study, THBS1 SNPs were not found to be associated with an increased incidence of gastric cancer overall, but an increased incidence of HDC gastric cancer found to be associated with the homozygous CC variant of rs2292305 T>C. In addition, we found no evidence of an under-representation of the homozygous CC THBS1 rs2292305 variant (ORadjusted=1.1 vs. 2.6) in LDC compared with HDC. Thus, it seems that carrying the homozygous CC variant of THBS1 rs2292305 might increase susceptibility to HDC gastric cancer, by not converting more of the LDC type to the HDC type. Analysis of the data also showed a statistically significant association between the homozygous CC of rs2292305 T>C variant and a higher differentiation status (p adjusted=0.03, ORadjusted 2.2, 95% CI of 1.1–4.5) (Table 2). However, it is important to note that the sample size only had a 67.4% and 74.7% power of detecting an OR of 2.6 for the HDC gastric cancer group and the control group and an OR of 2.2 for the HDC and LDC groups for the presence of THBS1 rs2292305 T>C, respectively. A power calculation to determine the sample size required for genetic association studies is essential; thus, such limited statistical power was unlikely to ensure the observed association between THBS1 rs2292305 T>C and gastric cancer. To provide the more a definitive conclusion, larger studies are now needed to validate these observations.
The major finding from this work is that rs1478604 A>G is associated with lymph node metastasis, especially in HDC gastric cancer (Table 4). The evidence for this is as follows: (a) only rs1478604 A>G is associated with lymph node metastasis of gastric cancer in the study group (p adjusted=0.018, ORadjusted 1.90, 95% CI of 1.1–3.3); (b) the four THBS1 SNPs studied here are located in one haplotype block and rs1478604 is in linkage disequilibrium with the other three SNPs. In fact, these SNPs form part of a common haplotype. In HDC, the p-value and OR obtained for rs1478604 A>G is higher than rs2228261 C>T, rs2292305 T>C, and rs3743125 C>T. It is highly probable, therefore, that of the four SNPs in question, the one with the real association with tumor metastasis is rs1478604 in HDC (which is located in the regulatory region of the THBS1 gene); (c) Our study had high enough power (90%) to detect the effect of the rs1478604 A>G SNP with an estimated relative risk of 4.2 in the metastasis group and non-metastasis group in HDC (Altman, 1991), whereas the power for detecting rs2228261 C>T, rs2292305 T>C, and rs3743125 C>T was only 65,2%, 67.5%, and 76.8%, respectively. Crucially, our data suggest, therefore, that the THBS1 rs1478604 A>G variant used in this study might prove a novel predictor of lymph node metastasis in HDC gastric cancer.
Previous studies have shown that THBS-1 is one of the most potent anti-angiogenic proteins (Canfield and Schor, 1995; Carpizo and Iruela-Arispe, 2000; Hawighorst et al., 2002). THBS-1 blocks endothelial cell (EC) proliferation and causes EC apoptosis by interacting with CD36 (Kazerounian et al., 2008). Negative correlations between cancer invasiveness, angiogenesis, and THBS1 have been confirmed in multiple studies from different researchers (Sargiannidou et al., 2001; Lawler, 2002). Recently, we have demonstrated that overexpression of THBS1 in gastric cancer tissue myofibroblasts promotes tumor cell metastasis (data not show). In the present study, we demonstrated that THBS1 rs1478604 A>G is significantly associated with lymph node metastasis in gastric cancer, especially HDC gastric cancer (Table 4). The rs1478604 A>G SNP is located in the 5′-UTR of THBS1, a region commonly implicated in translational regulation. Protein synthesis is often regulated at the initiation of translation stage, making it a critical step in the process. Regulation is mediated via cis-regulatory elements, which are located in the 5′- and 3′-UTRs (UTRs) and also by trans-acting factors. Breakdown in this regulation machinery can perturb cellular metabolism, leading to various physiological abnormalities. For example, mutations in the 5′-UTR often lead to impaired protein synthesis through loss of fine regulation (Signori et al., 2001; Pickering and Willis, 2005; Chatterjee and Pal, 2009). Recent reports showed that polymorphisms within the 5′-UTR were associated with a higher susceptibility to cancer (Lu et al., 2007; Hsieh et al., 2008; Qiu et al., 2010). Taking all of these findings together, we hypothesize that rs1478604 A>G may exert its effects by regulating the overall expression levels of the THBS-1 protein. Clearly, this hypothesis requires further investigation.
The present study has several limitations. First, the restricted sample size of our study limits the possibility to fully explore the effects of the genotypes; therefore, the results should be confirmed with a larger study. Second, data about the genotypes and history of environmental exposure in the subjects were not available; thus, it was not possible to explore gene–environment interactions. Although our results will need to be confirmed in a larger study, the work presented here implies that genetic polymorphism in THBS-1 may play important role in the development of gastric cancer.
Conclusion
In summary, the present study has demonstrated for the first time that THBS1 rs1478604 A>G is significantly associated with lymph node metastasis of gastric cancer, particularly the HDC type. In cases with HDC gastric cancer, our study had 90% power to detect an effect with an estimated relative risk of 4.2 in both the nonlymph node metastasis and the lymph node metastasis groups (under the dominant genetic model). Our data have not only confirmed the important role that THBS1 plays in lymph node metastasis in gastric cancer, but also provide additional information needed for genetic risk evaluation. Importantly, the data provide new insight into the biochemical properties of THBS-1. Further investigation of the role of this protein in cancer development and progression may be critical for its therapeutic application.
Footnotes
Acknowledgments
This work was supported by a scientific research grant from the Ministry of Health P.R. China (WKJ2008-2-43), the Key Program Fund of Fujian Medical University (09ZD020), and a Professorial Research grant from Fujian Medical University (JS060001). We thank all patients and control subjects for providing samples. We are grateful for the collaboration received from the participating hospitals and their staff.
Author Contribution
X.-D.L. participated in the design of the study, handled samples, performed SNP genotyping and analysis, and drafted the article; S.-Q.C. collected samples and performed SNP genotyping; Y.-L.Q. and J.-W.Z. extracted genomic DNA and collected clinical data; Y.T. participated in the design of the study and data analysis and funded the study; J.-Y.L. conceived the study, analyzed the data, and funded the study. The above authors have read, edited, and approved the final version of the article.
Disclosure Statement
The authors declare that they have no competing interests.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.