
Abstract
Dopamine D1 receptor (DRD1) gene is associated with the pathogenesis of myocardial infarction (MI) in aspects of plaque rupture, platelet aggregation, and neutrophil-mediated injury of cardiac myocytes. Thus, the study was designed to explore whether the A-48G polymorphism of the DRD1 gene was associated with MI. The genotype of the DRD1A-48G polymorphism was determined by polymerase chain reaction in the 602 Han Chinese participants, 255 MI patients and 347 controls without MI. A significant association was found between the A-48G polymorphism of DRD1 and MI (genotype model: χ 2=13.2, unadjusted p=0.001; χ 2=13.9, adjusted p=0.0002; dominant model: adjusted OR 2.05, 95%CI 1.40–3.00, p=0.0002; recessive model: adjusted OR 2.34, 95%CI 1.01–5.39, p=0.047). The G allele was a risk-increased allele for MI (unadjusted OR 1.83, 95%CI 1.34–2.50, p=0.0001; adjusted OR 1.94, 95%CI 1.40–2.68, p=0.00007). Thus, the study demonstrated the significant association between A-48G polymorphism of the DRD1 gene and MI.
Introduction
Vascular matrix metalloproteinases (MMPs) degrade extracellular matrix and lead to the breakdown of the fibrous cap in atherosclerotic plaque (Newby, 2005). Macrophage-derived foam cells release reactive oxygen species (ROS), which leads to increased vascular MMP activity and plaque instability (Rajagopalan et al., 1996; Newby, 2008). ROS also leads to endothelial dysfunction and increases the risk of MI by impairing endothelium-dependent vasodilation (Schlinzig et al., 2001). Antioxidants have been demonstrated to significantly improve endothelial function (Engler et al., 2003), and dopamine as a potent antioxidant potently inhibits any increase of oxidative stress through specifically activating vascular D1-like receptors (Yasunari et al., 2000). MI could also be precipitated by the activation of platelet whose activity is strongly influenced by circulating catecholamines (Anfossi and Trovati, 1996). The activation of DRD1 on chromaffin cells results in the secretion of great amount of catecholamines in a short time (Artalejo et al., 1990), which potentiates platelet activity and initiates thrombus formation. Catecholamines could also be secreted in a short time by chromaffin cells under emotional stress and lead to stress-induced cardiomyopathy (Lyon et al., 2007).
Neutrophils also have direct cytotoxic effects for cardiac myocytes in the pathogenesis of MI by releasing ROS and other toxic products (Frangogiannis et al., 2002). The mechanism of neutrophils' cytotoxic effect is the adhesion of neutrophils to coronary endothelium that is induced by the chemoattractive effect of IL-8 (Frangogiannis et al., 2002). Dopamine prevents the interaction between neutrophils and endothelium by potently inhibiting neutrophil chemotaxis and downregulating adhesion molecules (Sookhai et al., 2000).
Previous studies mainly focus on DRD1 that is expressed in renal tissues with the function of inhibiting reabsorption of water and sodium. A-48G polymorphism of the DRD1 gene, which is located at −48 bp of the 5′ untranslated region (UTR), increases the risk of primary hypertension in Japanese subjects (Sato et al., 2000). Until now, no report has been found to establish the relationship between DRD1 A-48G polymorphism (rs4532) and MI. Thus, we explored the association between A-48G polymorphism in the 5′-UTR of the DRD1 gene and the risk of MI.
Methods
Study subjects
This study had approval from the Ethics Committee of West China Hospital, Sichuan University (Chengdu, China). All participants voluntarily signed a written informed consent form. This case-control study included 602 unrelated Han Chinese patients (465 men and 137 women) from the Department of Cardiology, West China Hospital. We consecutively recruited patients from September 2007 to January 2011 who were diagnosed with MI by typical symptoms and signs of MI, electrocardiographic changes, and increased serum level of creatine kinase, aspartate aminotransferase, lactate dehydrogenase, and cardiac troponin I. The diagnosis of MI was further confirmed by performing coronary angiography detecting at least one stenosis of major coronary arteries (Thygesen et al., 2007). The control subjects were recruited from persons who had at least one of the conventional risk factors for coronary artery disease (CAD), including smoking, dyslipidemia, hypertension, and diabetes mellitus (DM). All the controls had no history of CAD, no present symptoms or signs of myocardial ischemia—such as chest pain, shoulder or arm pain—and no coronary lesion >50% diameter stenosis confirmed by coronary angiography. Their electrocardiograms and enzymes indicators for MI were normal. We excluded patients who had any history of hepatic failure, uremia, or severe infectious diseases within 2 weeks or had history of other unrelated chronic diseases, or allergy to intravenous contrast material.
Assessment of other covariates
Complete clinical history of all subjects was recorded, including age, sex, smoking, dyslipidemia, hypertension, DM, and coronary artery calcium (CAC). Patients who smoked 10 or more cigarettes per day were considered habitual smokers. Hypertension was defined by the mean of three independent measures of blood pressure >140/90 mm Hg or the previous use of antihypertensive drugs regardless of their present blood pressure. We determined DM by a fasting blood glucose level >7.0 mM or a blood glucose level at 2 h after oral glucose challenge >11.1 mM or the use of insulin or other hypoglycemic agents regardless of their present blood glucose level. Blood lipid levels included high-density lipoprotein cholesterol, cholesterol, total plasma cholesterol, triglyceride, and low-density lipoprotein cholesterol. Dyslipidemia was defined by the abnormal blood lipid levels or previous use of antidyslipidemia agents. All the blood samples were collected after an at least 8-h fasting. We also recorded the diagnosis of CAC made by cardiac fluoroscopy during coronary angiography.
Determination of genotypes
Genomic DNA was extracted by resin DNA purification kits (Beijing SBS Genetech Co., Ltd., Beijing, China) within 1 month. We examined the A-48G polymorphism of the DRD1 gene by a polymerase chain reaction (PCR) method. The forward primer was 5 GGCTTTCTGGTGCCCAAGACAGTG 3 and the reverse primer was 5 AGCACAGACCAGCGTGTTCCCCA 3. The PCR conditions were as follows: an initial denaturation step at 94°C for 5 min, followed by 35 cycles of denaturation at 94°C for 30 s, annealing for 30 s at 63°C, and elongation for 30 s at 72°C, with a final extension of 5 min at 72°C. Products of PCR amplification were 405-bp length fragments. PCR products were further digested with 1 U of DdeI at 37°C overnight following recommendations of Bio Labs, Inc. Fragments were separated in a 1.5% agarose gel and visualized by ethidium bromide staining. Results of genotyping were 3 fragments (146, 42, and 217 bp) for AA, 2 fragments (146 and 259 bp) for GG, and 4 fragments (146, 42, 217, and 259 bp) for AG (Fig. 1). The results of genotyping for DRD1 A-48G polymorphism were confirmed by direct gene sequence (Fig. 2).
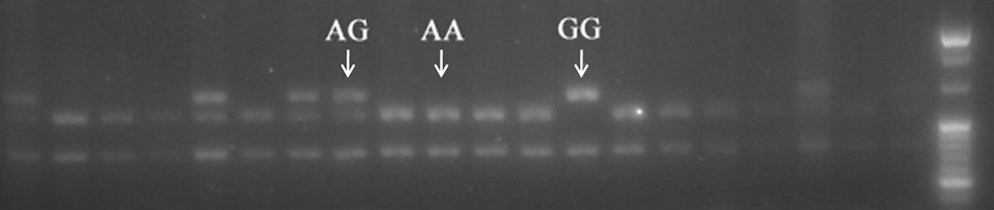
The polymerase chain reaction products were digested with DdeI and run on a 1.5% agarose gel. There are 3 DNA fragments of 259, 217, and 146 bp for AG; 2 DNA fragments of 217 and 146 bp for AA; 2 DNA fragments of 259 and 146 bp for GG.
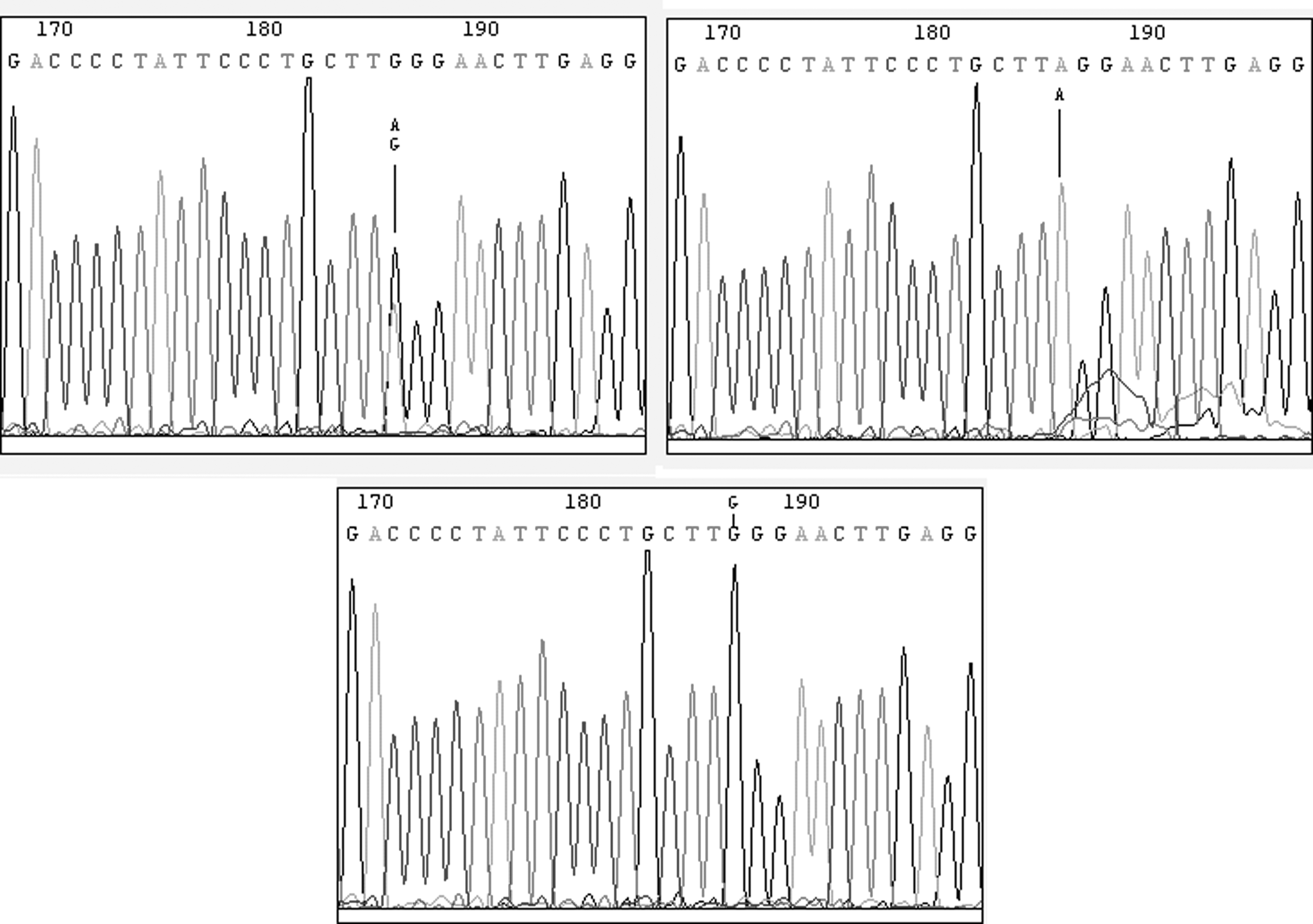
The G allele, A/G allele, and A allele were confirmed by sequencing.
Statistical analysis
Independent-samples t-test was conducted to compare quantitative variables, such as age. χ 2 test was used between groups for qualitative variables, allele frequencies, and Hardy–Weinberg equilibrium. Unconditional logistic regression, adjusted for age, sex, smoking, dyslipidemia, hypertension, and DM, was performed to calculate adjusted odds ratio (OR) and 95% confidential interval (CI) between groups in the analysis of allele frequencies and genotypes. Significance level of p-values was 0.05 in all statistical analysis. We used SPSS 13.0 (SPSS, Inc., Chicago, IL) for Windows (Microsoft Corp., Redmond, WA) in all statistical analysis.
Results
Baseline clinical characteristics of all the 602 participants are shown in Table 1. Risk factors, such as male gender, DM, and smoking, were more frequently found in MI subjects, and high-density lipoprotein cholesterol was higher in non-MI subjects. The overall power of our study (602 cases) was 0.940, when the OR is 1.912 in the dominant model of the univariate χ 2 test. Allele frequencies were consistent with Hardy–Weinberg equilibrium (p>0.05) using χ 2 test.
Independent-samples t-test was used to compare continuous data, including age, WBC, platelets, total cholesterol, LDL-c, and HDL-c, and data were mean±standard deviation. Categorical data were assessed by χ 2 test between MI patients and controls. MI, myocardial infarction; LDL-c, low-density lipoprotein-cholesterol; HDL-c, high-density lipoprotein-cholesterol.
The genotype and allele frequencies of DRD1 A-48G polymorphism in MI patients and non-MI controls are shown in Table 2. Significant difference was found in genotypes between MI patients and controls without MI (χ 2=13.2, unadjusted p=0.001; χ 2=13.9, adjusted p=0.0002). The G allele was a risk-increased allele for MI (unadjusted OR 1.83, 95%CI 1.34–2.50, p=0.0001; adjusted OR 1.94, 95%CI 1.40–2.68, p=0.00007; Table 3). Significant association between MI patients and controls was also found both in dominant model (AG/GG to AA, unadjusted OR 1.91, 95%CI 1.33–2.75, p=0.0004; adjusted OR 2.05, 95%CI 1.40–3.00, p=0.0002) and recessive model (GG to AA/AG, unadjusted OR 2.26, 95%CI 1.01–5.06, p=0.043; adjusted OR 2.34, 95%CI 1.01–5.39, p=0.047; Table 3).
p-Values were analyzed by χ 2 test.
Unadjusted ORs and p-values were analyzed by χ 2 test. Adjusted ORs and p-values were analyzed by unconditional logistic regression, adjusting for age, sex, smoking, dyslipidemia, hypertension, and DM. CI, confidence interval; OR, odds ratio; DM, diabetes mellitus.
We also found a significant difference between DRD1 A-48G polymorphism and CAC (genotype model: χ 2=8.0, unadjusted p=0.018; recessive model: GG to AA/AG, adjusted OR 3.54, 95%CI 1.26–10.00, p=0.017). No association or associative trend was found between the polymorphism and hypertension (adjusted OR 0.84, 95%CI 0.62–1.14, p=0.26), DM, dyslipidemia, angiographically characterized coronary stenosis, or other phenotypes (data not shown).
Discussion
We report an association between DRD1 A-48G polymorphism and the risk of MI. The overexpression of MMPs positively correlates with the histological characteristics of atherosclerotic plaque and clinical syndromes (Newby, 2005). MMP-2 and MMP-9 are significantly upregulated in unstable plaque compared to normal vascular tissue (Newby, 2005). Syndromes of patients also increase in plaques with higher expression of MMPs (Newby, 2005). Overexpression of MMPs is due to the stimulation of ROS released by macrophage-derived foam cells in the atherosclerotic plaque (Rajagopalan et al., 1996; Newby, 2008). In advanced atherosclerotic plaque, ROS increases the expression and activity of MMPs, destroys extracellular matrix, and makes the plaque prone to rupture (Rajagopalan et al., 1996; Newby, 2005). In addition to promoting plaque rupture through inducing overexpression of MMPs, ROS could also directly destroy myocytes and inhibit cardiac function. Through triggering the production of cytokines, ROS induces leukocyte chemotaxis and increases the adhesion between neutrophils and endothelium, which further injures cardiac myocytes. In animal model of ischemia/reperfusion, the administration of antioxidants significantly decreases infarct size. Overexpression of superoxide dismutase (SOD1) in transgenic mice protects myocardium from postischemic injury (Frangogiannis et al., 2002). The activation of vascular D1-like receptors strongly inhibits any increase of oxidative stress (Yasunari et al., 2000), and the antioxidative effect of the D1-like receptor–mediated pathway could be used as a novel method to prevent the rupture of atherosclerotic plaque and to reduce the risk of MI.
The formation of thrombus could also be precipitated by the aggregation of platelet (Hansson, 2005), which could be activated by circulating catecholamines or oxidative stress (Anfossi and Trovati, 1996). As a component of the sympathoadrenal system, DRD1 exists in chromaffin cells and its activation leads to rapid catecholamine secretion, which further potentiates the aggregating effects of platelets (Artalejo et al., 1990). The oversecretion of catecholamines could also directly injure cardiac myocytes (Lyon et al., 2007). In addition, dopamine receptors also exist in human platelets and influence platelet function (Ricci et al., 2001).
Neutrophils are involved in the pathogenesis of MI (Frangogiannis et al., 2002). In an animal model of ischemia/reperfusion, the accumulation of large-sized neutrophils in capillaries obstructs the blood perfusion to cardiac myocytes, and neutrophil depletion significantly decreases the infarct size (Frangogiannis et al., 2002). Except for the plugging effect of neutrophils in the microvasculature, recent studies mainly focus on the neutrophil-induced cytotoxicity for cardiac myocytes, which is mediated by release of ROS and proteolytic enzymes by neutrophils. Instead of circulating or free neutrophils, the effect is mediated by neutrophils that adhere to the endothelium of coronary arteries. During myocardial ischemia and reperfusion, cytokines induce cardiac myocytes to overexpress ICAM-1, making it possible for the Mac-1–expressing circulating neutrophils to adhere to the coronary endothelium. Neutrophil chemotaxis could be inhibited by antibodies to interleukin-8 (IL-8), and the specific ligand-receptor interaction is blocked by antibodies of ICAM-1, CD11b, and CD18 (Frangogiannis et al., 2002). Thus, in order to diminish the ischemic injury of cardiac myocytes, it is crucial to reduce the cytokines of inflammatory response and to inhibit the adhesion of neutrophils to endothelial cells. Dopamine significantly induces the apoptosis of neutrophils and diminishes their injury to cardiac myocytes (Frangogiannis et al., 2002). In addition, dopamine potently inhibits the neutrophil–endothelial interaction by downregulating the expression of both endothelial adhesion molecules (CD11b and CD18) of neutrophils, and receptors of endothelial cells (ICAM-1 and E-selectin) (Sookhai et al., 1999). It also shows antiinflammatory effect by attenuating the neutrophil chemotaxis mediated by IL-8 (Sookhai et al., 2000).
Although we found a significant association between this polymorphism and CAC, our study was initially designed to evaluate the association between this polymorphism and MI. Thus, the significant association between this polymorphism and CAC could merely be regarded as an occasional finding, and more accurate results require redesign of the entire study. However, the high OR value in the recessive model (adjusted OR 3.54, 95%CI 1.26–10.00, p=0.017) indicated the significance of performing further research to explore the association between DRD1 A-48G polymorphism and CAC.
Previous results are inconclusive and not uniform in the association between A-48G polymorphism of the DRD1 gene and hypertension (Kiryluk, 2009). After summarizing published articles about the association between this polymorphism and hypertension, Kiryluk concluded that the article of Fung et al. (2009) had the most convincing results that were correlated to population stratification and confirmed by a following cohort study. The results proved that hypertension was not associated with A-48G polymorphism of DRD1 gene in White individuals. The same conclusion is drawn from our study using Han Chinese subjects, which is helpful to clarify the association between this polymorphism and hypertension in multiethnic populations.
However, the study has shortcomings. DRD1 A-48G polymorphism was only analyzed in Han Chinese subjects, and multicentered cooperation would needed to achieve more widely applicable results of the association between DRD1 A-48G polymorphism and MI.
In conclusion, this case-control study demonstrated that G allele of DRD1 5′-UTR A-48G polymorphism was significantly associated with the increased risk of MI.
Footnotes
Acknowledgments
The authors thank the patients and their families for participation and cooperation. We also thank Shaodi Yan (M.D.), Lingai Pan (M.D.), and Hao Huang (M.D.) for collecting blood sample in the Department of Cardiology, West China Hospital, Sichuan University.
Disclosure Statement
There is no conflict of interest.