
Abstract
The DNA repair gene Ku70 plays a key role in the DNA double-strand breaks (DSBs) repair system. Defects in DSBs repair capacity can lead to genomic instability. We hypothesized that the Ku70 A-31G polymorphism (rs132770) was associated with the risk of renal cell carcinoma (RCC). In a hospital-based case–control study of 620 RCC patients and 623 cancer-free controls frequency matched by age and sex, we genotyped the functional polymorphism Ku70 A-31G (rs132770). Thirty-eight normal renal tissue samples with different genotypes were tested to estimate the Ku70 mRNA expression by real-time quantitative reverse transcription. Compared with the GG genotype, the GA and GA/AA genotypes had a significantly decreased risk of RCC [adjusted odds ratio (OR)=0.62, 95% confidence interval (CI)=0.44–0.87 for GA, and OR=0.62, 95% CI=0.45–0.86 for GA/AA]. The in vivo experiments with normal renal tissues revealed that a statistically significantly higher Ku70 mRNA expression was identified in samples with GA/AA genotypes compared with those with GG genotypes (p=0.001). These results suggested that the Ku70 A-31G polymorphism is involved in the etiology of RCC and, thus, may be a marker for genetic susceptibility to RCC in the Chinese populations.
Introduction
The human DNA repair system protects the genome from various insults caused by endogenous and environmental agents (Sugimura et al., 2006), and mutations or defects in the DNA repairing system are thought to be essential for tumorigenesis (Vogelstein et al., 2002; Miller et al., 2006). Therefore, mutations of DNA repair genes might have an important role in RCC carcinogenesis. Double-strand breaks (DSBs) are repaired by the DSBs repair system (Yu et al., 1999; Wood et al., 2001), which consists of two subpathways, a homologous recombination (HR), and nonhomologous end-joining (NHEJ) (Khanna and Jackson, 2001). In humans, NHEJ is the predominant repair system. To date, several proteins involved in the NHEJ pathway have been identified; namely, the ligase IV and its associated protein the X-ray cross-complementing group 4 (XRCC4); three components of the DNA-dependent protein kinase complex, Ku70, Ku80, and the DNA-dependent protein kinase; and the catalytic subunit (DNA-PKcs) (Jackson, 2002). Genetic variations in NHEJ genes influence DNA repair capacity and confer the predisposition to several cancers, including skin cancer (Han et al., 2004), breast cancer (Bau et al., 2004; Bau et al., 2007; Willems et al., 2008), gastric cancer (Chiu et al., 2008a), oral cancer (Chiu et al., 2008b), bladder cancer (Wang et al., 2008a), and renal cell carcinoma (Hirata et al., 2006).
Genetic polymorphisms in DSB repair genes have been shown as conferring predisposition to many different types of cancers, and Hirata et al. (2006) have investigated the association between some polymorphisms of DNA repair genes and the risk for RCC, such as XRCC1, XPC, ERCC1, XRCC3, and XRCC7. However, no study has yet confirmed the association between the polymorphisms of Ku70, which is the most important gene in the human DNA repair system, and the risk of RCC. Some epidemiological studies have investigated the association between the Ku70 polymorphisms and the risk for different types of cancers, including gastric cancer (Yang et al., 2011), oral cancer (Chiu et al., 2008b), and breast cancer (Fu et al., 2003). We found that there are only two Single-Nucleotide Polymorphisms (SNPs) (rs132770 and rs2267437) in the functional area of the Ku70 gene, the Chinese population is reported in the HapMap database, and the minor allele frequency (MAF) >0.05. In those epidemiological studies, only Fu et al. (2003) found that the significant polymorphism in Ku70 is rs2267437 in breast cancer; all the other studies had negative results, but the limited sample size (254 primary breast cancer patients) could not provide enough power of the result. Besides that, polymorphism rs132770 is closer than polymorphism rs2267437 to the location of translation starting, so we hypothesized that polymorphism rs132770 might have a stronger role in the Ku70 gene transcriptional regulation. To test this hypothesis, our present study was designed to investigate the association of the Ku70 A-31G polymorphism with the risk of RCC in our ongoing hospital-based case–control study conducted on a Chinese population. In addition, we investigated the association of the Ku70 mRNA expression with RCC risk in vivo by reversed transcriptase–polymerase chain reaction (RT-PCR) to assess the potential functional effect of Ku70 A-31G polymorphism on RCC risk. To the best of our knowledge, this is the first study that evaluates the association between the Ku70 A-31G polymorphism and the susceptibility to RCC or explores the potential function of this polymorphism in RCC.
Materials and Methods
Study subjects
This case–control study included 620 incident patients with RCC and 623 control subjects. All subjects in our study were Han Chinese with no biological relationship. All the patients were newly diagnosed and had histopathologically confirmed incident RCC without previous history of other cancers or previous chemotherapy or radiotherapy and were consecutively recruited into an ongoing study from July 2006 at The First Affiliated Hospital of Nanjing Medical University, Nanjing, China (Zhu et al., 2010). The cancer-free control subjects were genetically unrelated to the RCC patients and had no individual history of cancer. The controls were recruited from healthy subjects who were seeking health care in the outpatient departments at the hospital. All controls were of appropriate age and sex for frequency matching with the RCC patients, and they gave their informed consent. Exclusion criteria for the controls were significant mental impairment or blood transfusion within the past few months. Controls were also excluded if they had symptoms suggestive of RCC, such as hematuria. Before recruitment, a standard questionnaire was administered by trained interviewers to obtain information on demographic data and related factors through face-to-face interviews. Each patient donated 5 mL venous blood after providing a written informed consent. The response rate for both case and control subjects was >85%. The study was approved by the institutional review board of the Nanjing Medical University.
Genotyping
Total genomic DNA was isolated from leucocytes of peripheral blood by proteinase K digestion and phenol/chloroform extraction. Genotyping of the polymorphism was performed by the MGB TaqMan probe assay from Applied Biosystems Inc. (Foster City, CA). The sequences of primer and probe for each SNP are available on request. According to the manufacturer's instructions, amplifications were performed in the 384-well ABI 7900HT Real-Time PCR System (Applied Biosystems). After the completion of the amplification, the fluorescence intensity in each well of the plate was read and analyzed with SDS 2.3 automated software. Four blank controls were included in each plate to ensure accuracy of the genotyping. About 10% of the samples were randomly selected for repeated assays, and the results were 100% concordant.
Analysis of Ku70 mRNA expression
To further evaluate the correlation between the Ku70 mRNA expression and the A-31G polymorphism, 38 surgically removed normal renal tissue samples adjacent to tumors with different genotypes were subjected to extraction of the total RNA using Trizol Reagent (Invitrogen, Carlsbad, CA) according to the manufacturer's protocol. The total RNA was measured by real-time quantitative RT-PCR (ABI Prism® 7300HT real-time quantitative PCR instrument). GAPDH was used as an internal quantitative control. The detailed methods for real-time qRT-PCR were previously described (Wang et al., 2008b). The primers used for the amplification of Ku70 mRNA were 5′-CGA TAA TGA AGG TTC TGG AAG-3′ (forward) and 5′-CTG GAA GTG CTT GGT GAG - 3′ (reverse), and the primers for GAPDH were 5′-GAA ATC CCA TCA CCA TCT TCC AGG-3′ (forward) and 5′-GAG CCC CAG CCT TCT CCA TG - 3′ (reverse). Fold changes were normalized by the levels of GAPDH expression, and each assay was done in triplicate.
Statistical analysis
Differences in the distributions of demographic characteristics, selected variables, and frequencies of genotypes of the Ku70 A-31G polymorphism between the cases and controls were evaluated using the Student's t-test (for continuous variables) and χ
2-test (for categorical variables). The Hardy–Weinberg equilibrium (HWE) was assessed using a goodness-of-fit χ
2-test. The associations between the Ku70 A-31G polymorphism and RCC risk were estimated by computing odds ratios (ORs) and their 95% confidence intervals (CIs) from an unconditional logistic regression analysis with the adjustment for possible confounders. The statistical power was calculated by using the PS software (
Results
Characteristics of the study population
Basic characteristics of the study subjects are summarized in Table 1. There were no differences between the cases and controls with regard to age, sex, body mass index (BMI), drinking status, and family history of cancer (all p>0.05). However, there were more subjects with smoking status (36.8%), hypertension (36.8%), and diabetes (13.4%) among the cases than among the controls (31.5%, 28.1%, and 5.8%, respectively), and these differences were found to be statistically significant (p=0.048 for smoking status, p=0.001 for hypertension, and p<0.001 for diabetes). The majority of patients (83.5%) had the conventional clear cell carcinoma. Eighteen patients (2.9%) had papillary carcinoma, and forty patients (6.5%) had chromophobe carcinoma. In addition, there were 44 (7.1%) unclassified RCC patients. Approximately 63.6% of the patients were in stage I, and 18.6%, 6.8%, and 11.0% of the patients were found to be in stages II, III, and IV, respectively. The nuclear grades from I to IV were 18.6%, 47.9%, 24.8%, and 8.7%, respectively.
T-test for age and BMI distributions between cases and controls; Two-sided χ 2-test for other selected variables distribution between cases and controls.
BMI, body mass index.
Association between the Ku70 A-31G polymorphism and RCC risk
The genotype and allele distributions of the Ku70 A-31G polymorphism in the cases and controls are shown in Table 2. The observed genotype frequencies for this polymorphism were in HWE in the controls (p=0.111). The MAF of the polymorphism was consistent with that reported in the HapMap database. As shown in Table 2, the frequencies of the GG, GA, and AA genotypes were 88.7%, 10.3%, and 1.0%, respectively, among the cases, and 82.5%, 16.1%, and 1.4%, respectively, among the controls. After adjusting for possible confounding factors (age, sex, smoking status, drinking status, hypertension, and diabetes), subjects with the GA or GA/AA genotypes were found to have a decreased risk of RCC (adjusted OR=0.62, 95% CI=0.44–0.87 for CG, and 0.62, 0.45–0.86 for CG/GG; P trend =0.003), relative to those with the GG homozygote, and individuals with the A allele had a decreased risk of RCC, relative to those carrying the G allele (p=0.002). These data indicated that individuals carrying variant A alleles may have a lower risk of RCC.
Two-sided χ 2-test for either genotype distributions or allele frequencies between the cases and controls.
Adjusted for age, sex, smoking status, drinking status, hypertension, and diabetes in logistic regression model.
OR, odds ratio; CI, confidence interval.
We further evaluated the effect of the Ku70 A-31G polymorphism on RCC risk stratified by age, BMI, sex, smoking status, drinking status, clinical stage, and tumor grade. As presented in Table 3, we found that this significant protective effect of the rs132770 variant against RCC risk was more pronounced among male patients (adjusted OR=0.49, 95% CI=0.32–0.75, p=0.064 for heterogeneity test), and smokers (0.43, 0.25–0.77, 0.086).
Adjusted for age, sex, smoking status, drinking status, hypertension, and diabetes in logistic regression model.
p for heterogeneity.
Association of the Ku70 A-31G polymorphism with expression levels of the Ku70 mRNA
We collected 38 surgically removed normal renal tissue samples adjacent to tumors. These were obtained from the untreated RCC patients with different genotypes of the Ku70 A-31G polymorphisms, and the frequency distributions of the GG, GA, and AA genotypes were 28, 8, and 2, respectively. The effects of these three genotypes on the transcriptional activity or mRNA levels were evaluated by real-time quantitative RT-PCR (Fig. 1). The two samples with the AA genotype were added to the samples of the GA genotype for analysis, and statistically significantly higher levels of Ku70 mRNA expression were identified in samples from patients with GA/AA genotypes than from those with GG genotypes (p=0.001).
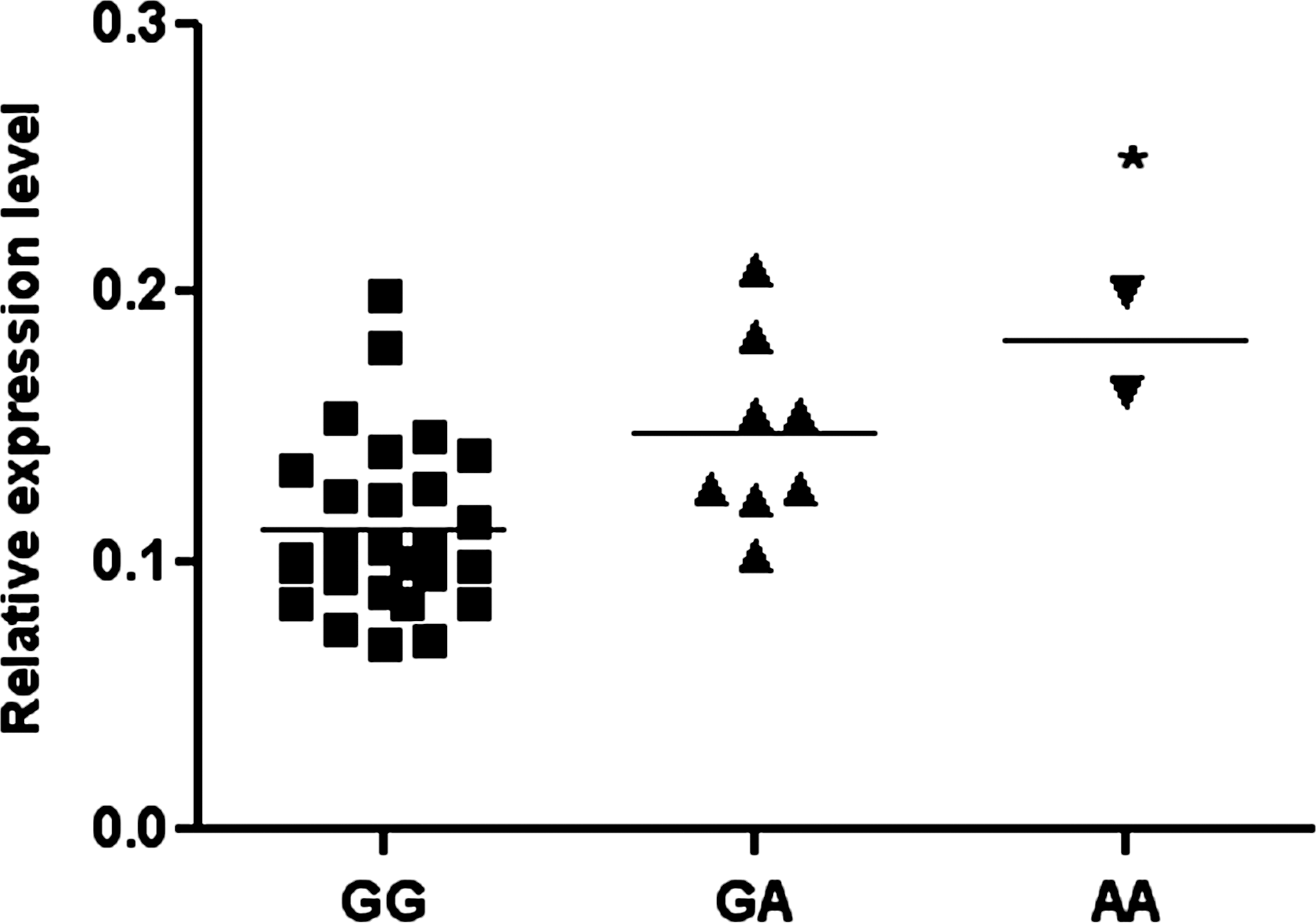
Analysis of Ku70 mRNA expression levels in three groups of normal renal tissue samples with mean values (horizontal lines, mean values). *p<0.05 relative to GG and GA/AA genotypes.
Discussion
In this ongoing hospital-based case–control study, we investigated the association of the Ku70 A-31G polymorphism and the risk of RCC in a Chinese population. We found that individuals with the A allele were associated with a decreased risk of RCC, and this significant protective effect against RCC risk was more evident for subgroups of male patients and ever smokers. To the best of our knowledge, this is the first study dealing with the association of the Ku70 A-31G polymorphism with RCC risk in a Chinese population. Our larger sample size relative to the previous research and concise data analysis strengthens the accuracy and reliability of our finding. Besides this, we first explore the potential function of this polymorphism in RCC. Our study could lay a solid theoretical foundation that explores the role of the DSBs repair system in the occurrence and development of renal cell carcinoma.
The human Ku70 gene forms a heterodimer complex with Ku80. However, Ku70 may perform functions independent of Ku80 (Wang et al., 1998). Ku70-knockout mice have small populations of mature T-lymphocytes, a significant incidence of thymic lymphomas, and an increased rate of fibroblast transformation, but the Ku80-knockout mice do not. The underlying mechanisms for this difference remain unknown till now (Featherstone and Jackson, 1999). Ku70 can translocate to the nucleus without forming a heterodimer complex with Ku80 following its own nuclear location signal (Koike et al., 1999; Koike et al., 2000). The defects in Ku70 may induce not only deficiencies in DSBs repair but also growth retardation, hypersensitivity to ionizing radiation, and severe combination immune deficiency due to severely impaired variable division joining (V[D]J) recombinations (Khanna and Jackson, 2001; Gu et al., 1997). However, small genetic variations in Ku70 such as polymorphisms might escape cell checkpoint surveillance. These variations can lead to suboptimal DNA repair, which would allow DNA damage to accumulate, and this could trigger tumor initiation (Fu et al., 2003). Therefore, genetic variants in the Ku70 gene are hypothesized to play a critical role in tumorigenesis. Some epidemiological studies have investigated the association between the Ku70 A-31G polymorphism and its risk for different types of cancers, including gastric cancer (Yang et al., 2011), oral cancer (Chiu et al., 2008b), and breast cancer (Fu et al., 2003). In those epidemiological studies, only Fu et al. (2003) found that the significant polymorphism in Ku70 is rs2267437 in breast cancer; all the other studies displayed negative results, but the limited sample size (254 primary breast cancer patients) could not provide enough power of the result. Besides this, polymorphism rs132770 is closer than polymorphism rs2267437 to the location of translation starting. We hypothesized that polymorphism rs132770 might play a stronger role in the Ku70 gene transcriptional regulation; so, we decided to investigate whether polymorphism rs132770 is associated with the risk for RCC. Although polymorphism rs132770 had no significant association in those epidemiological studies, our study found that the Ku70 A-31G polymorphism was associated with RCC risk. The discrepancy could be interpreted as suggesting that different mechanisms underlie the development of different tumors, and the Ku70 gene may play various roles in different tumorigenesis. In addition, our sample size has been greatly improved compared with previous studies, which increased the power of our result. In fact, Hirata et al. (2006) first reported that the SNPs of DNA repair genes were associated with an increased risk for RCC. Epidemiological studies have shown that many different environmental and/or occupational factors, such as chemical carcinogens, including polycyclic aromatic hydrocarbons, aromatic amines and N-nitroso compounds, some anticancer drugs, and reactive oxygen species (ROS), are responsible for the development of RCC (Clayson and Cooper, 1970; Chow et al., 2010). Furthermore, studies have revealed that ROS can induce DNA base damage, DNA single-strand breaks, and DSBs (Pryor et al., 1983). The DSBs may lead to genome instability, which, in turn, may enhance the development of cancer (Karran, 2000).
The Ku70 A-31G polymorphism, which is mapped to the promoter region of Ku70, does not directly result in an amino-acid coding change; it is plausible to suspect that the alternative spicing, intervention, modification, determination, or involvement of this SNP influences the expression level or stability of the Ku70 protein (Chiu et al., 2008b). Therefore, we designed a functional experiment to investigate whether the A-31G polymorphism influences the expression levels of the Ku70 mRNA in vivo. We found that the A allele had increased the expression levels of the Ku70 mRNA by the result of real-time quantitative RT-PCR. This finding fully supported the hypothesis just described. The A allele might increase the expression levels of the Ku70 mRNA, which may lead to an increased expression of the Ku70 protein. The Ku70/Ku80 (Ku) heterodimer is the first protein that binds to the damaged DNA ends. When bound to the DSBs, Ku recruits and activates DNA-PKcs (Willems et al., 2009); so, its increased expression could also increase the ability to repair DNA, and this might ultimately reduce the incidence of tumors.
Furthermore, we found that the protective effect of the Ku70 variant genotype was more pronounced in smokers, but not in nonsmokers. Actually, cigarette smoking is the most consistently established causal risk factor for RCC (McLaughlin and Lipworth, 2000). It has been estimated to account for ∼20% of RCC (Lipworth et al., 2006). Smoking can lead to different levels of DNA damage (Lodovici and Bigagli, 2009); therefore, the role of the Ku70 variant genotype might be more obvious in the smoking population. We also observed that this decreased risk was more pronounced in men; although the exact molecular mechanisms underlying this risk are unknown, it is possible that individuals in this subgroup more likely were less exposed to some risk factors involved in the etiology of RCC (Chow et al., 2010). Our findings provide evidence that genetic variants may exert different effects on the pathogenesis of different smoking status and sex of RCC.
Some limitations may exist in the present study. First, our sample size is moderate, and we did not have detailed information on environmental factors, such as occupational exposures, diet, and physical activity; these may limit the statistical power of our study, especially for subgroup and interaction analyses. However, we had 80% power at a 0.05 significance level to detect an OR of 1.4 or greater and 0.7 or smaller with an exposure frequency of 30%, given the sample size of our current study. Besides that, we also had 80% power at a 0.05 level that detects the value of OR in Male and Smoker subgroups (data not shown). Second, since our study was a hospital-based study design, we could not rule out the possibility of the selection bias of subjects who may have been associated with a particular genotype. However, the agreement with HWE and a similar allele frequency of our controls to those reported in the East Asian populations suggested that the selection bias in terms of genotype distribution would not be substantial. Third, since there may be some differences in the levels of the Ku70 mRNA between both tumor and normal adjacent tissues, the expression levels of the Ku70 mRNA associated with the promoter A-31G polymorphism should be validated in both tumor tissues and normal adjacent tissues in future studies. In addition, only one SNP of Ku70 is chosen for genotypic and phenotypic investigations in our study; the other significant SNPs in RCC are waiting to be the subject of some other research. This is also a limitation of the present study.
In conclusion, our present study indicates that the functional Ku70 A-31G polymorphism is associated with a decreased risk of RCC in a Chinese population, and this novel functional Ku70 genetic variant may affect the expression levels of the Ku70 mRNA. Further functional studies and larger well-designed prospective studies are warranted.
Footnotes
Acknowledgments
This study was partly supported by the National Natural Science Foundation of China (30972444, 81102181, and 81102089), the Key Program of Natural Science Foundation of Jiangsu Province (BK2010080), the National Natural Science Foundation of Jiangsu Province (BK2011773), the Key Program for Basic Research of Jiangsu Provincial Department of Education (08KJA330001 and 11KJB330002), the Qin Lan Project of Jiangsu Provincial Department of Education, and the Priority Academic Program Development of Jiangsu Higher Education Institutions (Public Health and Preventive Medicine).
Disclosure Statement
The authors declare no conflicts of interest.