
Abstract
Glutathione S-transferase T1 (GSTT1) is implicated in the inactivation of procarcinogens that contribute to cancer progression. However, studies investigating the association between GSTT1 polymorphism and bladder cancer (BC) risk have reported conflicting results; therefore, a meta-analysis was conducted. Fifty studies with 10,805 cases and 13,332 controls were recruited. The overall odds ratio for the GSTT1 null genotype was 1.1502 (95% CI=1.0384–1.2741). When stratified by ethnicity, significantly increased risk was only found for Caucasians. In Asians subgroup, interestingly, decreased BC risks were found in the Korean and Japanese populations but not in the Chinese population. When stratified by control sources, a slightly elevated risk was found in population-based but not in hospital-based studies. Besides, smoking was not found to modify the association between the GSTT1 null genotype and BC risk. When combined with the GSTM1 null genotype, a remarkably increased risk was found for BC. In general, our results suggest that the GSTT1 null genotype is associated with an increased risk of BC. Smoking did not modify the association between the GSTT1 null genotype and BC risk. Furthermore, a strong association was observed between the combination of GSTT1 null and GSTM1 null genotype and risk of BC. Further epidemiological studies will be needed to confirm our findings.
Introduction
The glutathione S-transferases (GSTs) are multigene family-related isozymes that detoxify reactive chemical species, such as polycyclic aromatic hydrocarbon epoxides present in tobacco smoke, to excretable hydrophilic metabolites (Hayes and Pulford, 1995). GSTs are expressed in many tissues and serve as a protection against cytotoxic and potentially carcinogenic chemicals (Eaton and Bammler, 1999). Individual genetic differences may influence the activity level of GSTs and susceptibility to cancer, particularly in cases of higher exposure to toxic and carcinogenic agents (Rebbeck, 1997; Strange and Fryer, 1999). Currently, GSTs include seven classes of isoenzymes: μ, π, θ, α, κ, σ, and ξ. Several GSTs are polymorphic that contain one or more homodimer or heterodimer forms and these polymorphisms may be relevant in carcinogenesis (Pemble et al., 1994). Allelic variations have been identified in four of these families: α, μ, π, and θ (Strange et al., 2000). Among them, most extensively studied in humans are the polymorphisms of Glutathione S-transferase T1 (GSTT1; θ) and GSTM1 (μ). Both of them have been identified deletions that can cause null alleles. It was reported that people with the GSTT1 null genotype may have abolished enzyme activities and decreased ability to detoxify the common environmental or dietary agents, especially 1,3-butadiene and ethylene oxide, which produce chromosomal damage (Pemble et al., 1994; Wiencke et al., 1995). In contrast to GSTT1, the GSTM1 null genotype shows lower capacity to detoxify certain carcinogens (Harada et al., 1992; Nakajima et al., 1995). Therefore, individuals with GSTT1 null and GSTM1 null genotypes might be at an increased risk of developing cancer (Rebbeck, 1997). However, inconsistent results have been reported in various reports studying the potential role of the GSTT1 genotype in individual susceptibility to BC. Some studies exhibited nonsignificant increased risk of BC with the GSTT1 null genotype (García-Closas et al., 2005; Zhao et al., 2007; Yuan et al., 2008; Cantor et al., 2010; Moore et al., 2011), while some other studies showed significantly enhanced risk of BC with the GSTT1 null genotype (Sanyal et al., 2004; Srivastava et al., 2004; Saad et al., 2005; Sobti et al., 2005; Altayli et al., 2009; Henríquez-Hernández et al., 2011).
To clarify the effect of GSTT1 polymorphism on the risk of developing BC, we collected all the eligible published data until October 2011 and used meta-analysis with subgroup analysis to evaluate the association between the GSTT1 null genotype and BC risk.
Materials and Methods
Publication search
PubMed, Google Scholar, and China National Knowledge Infrastructure were searched (updated to 2011/10/11) using the combination of the following key words: “glutathione S-transferase T1” or “GSTT1,” “bladder” or “urothelial,” “cancer” or “carcinoma” or “neoplasm,” without any restriction on language. Reference lists of reviews and retrieved articles were also searched by hand. We did not consider abstracts or unpublished studies. Any disagreement was resolved by discussion between the authors.
Inclusion and exclusion criteria
For the meta-analysis, the following inclusion criteria were followed: (1) clear objective in the relation between GSTT1 polymorphism and BC; (2) sufficient published data about the size of the sample, odds ratio (OR), and their 95% confidence interval (CI); (3) when more than one articles were identified for the same study population or with overlapping data, we included the most recent one or the one with the most complete data. The exclusion criteria were (1) incomplete data, (2) no control, and (3) duplicate studies.
Data extraction
Data were carefully and independently extracted from all eligible publications by two of the authors according to the inclusion criteria. For conflicting evaluations, an agreement was reached following a discussion. All extracted data were included in Table 1. Different ethnicities were categorized as Caucasian, Asian, African, and mixed. Study designs were stratified to population-based studies and hospital-based studies.
Null/present.
GSTT1, glutathione S-transferase T1; PB, population-based controls; HB, hospital-based controls.
Statistical analysis
The strength of association between the GSTT1 null polymorphism and BC risk were measured by ORs with 95% CI. The statistical significance of the pooled ORs was examined by Z test, and P (two-tailed)<0.05 was considered statistically significant. Heterogeneity among studies was checked by the I 2 test (Higgins et al., 2003). Fixed-effects model (the Mantel–Haenszel method) was used when there was no heterogeneity (I 2 <50%) (Mantel and Haenszel, 1959). Otherwise, the random-effects model (the DerSimonian and Laird method) was used (DerSimonian and Laird, 1986). Subgroup analysis was performed by ethnicity, study design, smoking status, and the combination of the GSTM1 null genotype. Sensitivity analysis was performed by omitting each study in turn to assess the stability of results. As publication bias was always concerned in meta-analysis, the funnel plot was drawn to examine publication bias, and the degree of asymmetry was tested by Egger's test (p<0.05 was significant publication bias) (Egger et al., 1997). The statistical analysis was performed with MIX statistical software (Version 1.7 for windows).
Results
Study characteristics
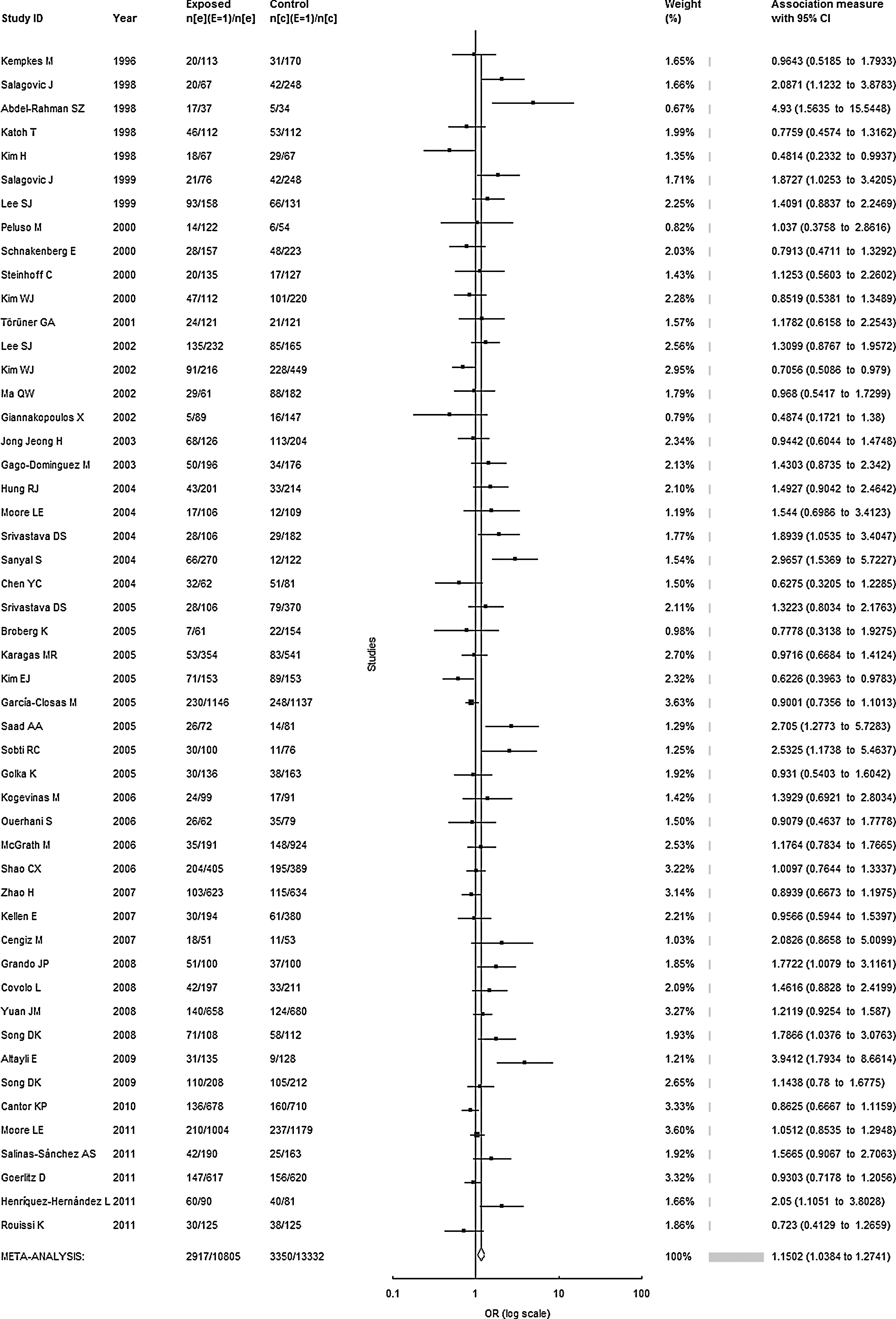
We obtained 63 relevant articles that examined the GSTT1 polymorphism and BC risk after searching and screening with our eligibility criteria. After data extraction, we excluded 11 articles without sufficient information needed for OR calculation. Four articles were overlapped (Georgiou et al., 2000; Giannakopoulos et al., 2002; Rouissi et al., 2009; Rouissi et al., 2011) and only two were retained considering the criteria mentioned above (Giannakopoulos et al., 2002; Rouissi et al., 2011). Hence, 50 studies including 10,805 cases and 13,332 controls were involved in this meta-analysis (Table 1). Out of the 50 studies, 48 were case–control studies, 1 was nested case–control (McGrath et al., 2006) study, and 1 was cross-sectional study (Salinas-Sánchez et al., 2011). In all eligible studies, there were 31 studies of Caucasians, 12 studies of Asians, 2 studies of Africans, and 5 of mixed populations. Among these researches, 28 of them were population-based and 22 were hospital-based researches (due to a small sample size of the nested case–control study, we categorized it into hospital-based subgroup). History of smoking was verified in 18 studies. In addition, 12 studies reported the combination of GSTT1 and GSTM1 genotypes in BC patients and controls.
Overall analysis
Table 2 summarizes the results of the GSTT1 null genotype and BC risk. Overall, we found a significant association between the GSTT1 null genotype and the risk of BC (OR=1.1502, 95% CI=1.0384–1.2741, p=0.0073, I 2=55.62%, Fig. 1) based on all the studies. Due to the significant heterogeneity of these studies, random-effects model was conducted.
Meta-analysis of Glutathione S-transferase T1 gene polymorphism and bladder cancer risk.
OR, odds ratio; CI, confidence interval.
Including mixed population and Africans.
Both GSTT1 and GSTM1 null genotypes versus both GSTT1 and GSTM1 present genotypes.
Ethnic origin
In the subgroup analysis by ethnicity, it was suggested that presence of the GSTT1 null genotype significantly increases the risk of BC in Caucasians (OR=1.3176, 95% CI=1.1452–1.5159, p=0.0001, I 2 =58.31%). However, no dramatically increased risk was found for Asians or the other populations, which include Africans and mixed populations (Asians: OR=0.9161, 95% CI=0.8077–1.039, p=0.1723, I 2 =47.26%; other populations: OR=1.0404, 95% CI=0.8841–1.2242, p=0.6335, I 2 =27.84%). Furthermore, when stratified by country, no remarkably enhanced risk of BC with the GSTT1 null genotype was acquired in the Chinese population (OR=1.0691, 95% CI=0.8865–1.2893, p=0.4843, I 2 =35.9%). On the other hand, interestingly, it was shown that there is probably a protective effect of the GSTT1 null genotype to BC in the Korean and Japanese populations (OR=0.8061, 95% CI=0.6798–0.956, p=0.0132, I 2 =39.37%).
Control sources
When stratified by control sources, slightly elevated risk was found in population-based controls (OR=1.1438, 95% CI=1.002–1.3056, p=0.0466, I 2 =55.22%), but not in hospital-based controls (OR=1.1617, 95% CI=0.983–1.3728, p=0.0786, I 2 =58.08%).
Smoking status (smokers and nonsmokers)
Considering that smoking is an important risk factor of BC (Knight et al., 2002), further analysis according to smoking status was performed. From the data available in 18 of 50 studies, it was showed that there was no enhanced risk for smokers or nonsmokers with the GSTT1 null genotype (smokers: OR=1.0812, 95% CI=0.9619–1.2154, p=0.1907, I 2 =29.94%; nonsmokers: OR=1.1037, 95% CI=0.9271–1.3138, p=0.2674, I 2 =13.12%). In addition, smoking was not found to alter the association between the GSTT1 null genotype and BC risk (OR=1.0231, 95% CI=0.869–1.2044, p=0.7843, I 2 =31.11%).
Combination of genotypes
Twelve of 50 studies reported the combination of GSTT1 and GSTM1 genotypes in BC patients and controls. Contrasting the data of controls suggested a remarkable increase in the risk of BC for people with both GSTT1 null and GSTM1 null genotypes compared to those with both GSTT1 present and GSTM1 present genotypes (OR=1.7168, 95% CI=1.4386–2.049, p<0.0001, I 2 =49.43%).
Sensitivity analyses
The sensitivity analysis was tested for all subjects and subgroups by removing a single study each time. The corresponding pooled ORs were not materially altered in all subjects and the most subgroups except population-based controls (data not shown). The sensitivity analysis results revealed an uncertainty of population-based subgroup, indicating that the result of this subgroup must be interpreted with caution.
Publication bias
Funnel plot and Egger's test were used to assess the publication bias. The shape of the funnel plot (Fig. 2) seemed to be approximately symmetrical, but the symmetrical degrees were not content. Therefore, Egger's test was applied to provide statistical evidence of funnel plot symmetry, and the results showed that the publication bias might exist (p=0.0026).
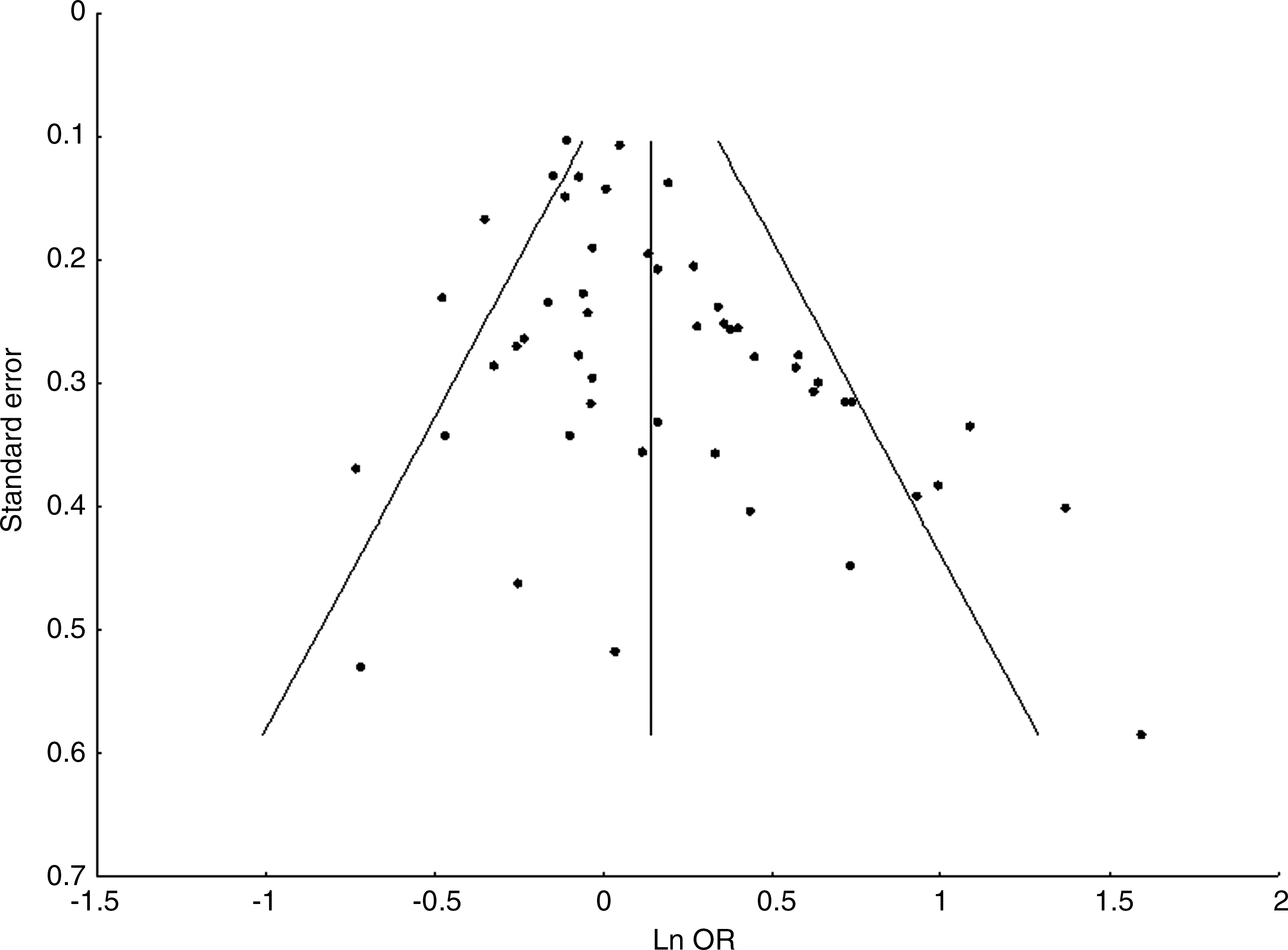
Funnel plot of the published studies considered in the meta-analysis.
Discussion
At present, it is accepted that the carcinogenesis of BC is a multifactorial and multistep process, and one major possible mechanism is molecular alteration. Interindividual variations in the molecular, genetic, and cellular mechanisms of detoxification system such as polymorphisms of the GSTs family could potentially affect the susceptibility to BC (Franekova et al., 2008). The GST family contains multiple enzymes that can detoxify reactive chemical materials. Several GSTs are polymorphic, which may be related to the risk of carcinogenesis (Pemble et al., 1994). In 1996, Kempkes et al. first reported the association between the GSTT1 null genotype and the risk of BC among Germans. Following this initial report, many studies had investigated the association between polymorphism of GSTT1 and the susceptibility of BC during the past decades, but the findings were inconsistent and controversial. Therefore, we undertook the present meta-analysis aiming to derive an estimate of the BC risk associated with the GSTT1 null genotype. As a powerful statistical method, meta-analysis enabled us to pool the results of individual studies and to obtain a more accurate estimate for investigations (Ioannidis et al., 2001; Munafò, 2004). Although, one meta-analysis (Zeng et al., 2010) showed that GSTT1 null status was associated with a modest increase in the risk of BC, many recent studies have investigated the association between the GSTT1 null genotype and BC risk over the last 2 years. As a result, an updated meta-analysis is needed.
In the present study, we critically reviewed and included 50 studies (10,805 cases of BC and 13,332 controls) about the GSTT1 genotype and BC risk. Therefore, it makes a more detailed and powerful evaluation than the prior meta-analysis, which included studies up to August 2008 (33 studies including 6,986 cases of BC and 9,166 controls). Our meta-analysis showed significant associations between the GSTT1 null genotype and BC risk in all subjects (OR=1.1502, 95% CI=1.0384–1.2741, p=0.0073, I 2 =55.62%), which was consistent with the previous meta-analysis. Furthermore, it is now widely accepted that different distribution of various ethnicities between cases and controls may be a source of confounding when pooling studies (Garte, 1998), so we stratified the data based on ethnicities. Our results revealed that a remarkable increase in risks of BC with the GSTT1 null genotype existed for Caucasians but not for Asians or other populations (include mixed population and Africans). These results are possibly due to that the GSTT1 polymorphism shows distinct frequencies among different ethnic groups. In human populations, the frequency of GSTT1 null is 13%–26% and 36%–52% in Caucasian and Asian individuals, respectively (Garte et al., 2001). In addition, when stratified by country, no dramatically higher risk of BC was detected with the GSTT1 null genotype in the Chinese population, and this result was consistent with the result of Asians. However, a totally different result showed that there was a probable protective effect of the GSTT1 null genotype to BC in the Korean and Japanese populations. Our findings are supported by the results of Kim EJ et al. (2005) and Kim WJ et al. (2002). Both of their results proved a decreased risk of BC with the GSTT1 null genotype. However, the complete difference observed may possible due to chance, as the studies with small sample size might have insufficient statistical power or generated a fluctuated risk estimate (Wacholder et al., 2004). So, the results for Asians, some Asian countries, and other populations should be interpreted cautiously and further investigation ought to be performed.
Currently, it is conceivable that the GSTT1 gene could influence the susceptibility to noncancer diseases, such as asthma (Saadat et al., 2004) and cardiovascular disease (Doney et al., 2005); therefore, its genotype frequency possibly differs between the population-based and hospital-based controls. Moreover, conclusions of systematic reviews usually depend on control selection procedures (Benhamou et al., 2002). Hence, the results for studies of population-based and hospital-based controls might be dissimilar. In our study, a slightly elevated risk was showed in population-based controls, but no significant risk was observed in hospital-based ones. Nevertheless, the sensitivity analysis results exhibited an uncertainty in population-based studies. Therefore, we should treat the result carefully and further studies based on population design are necessary to confirm the association.
It has been known that smoking is an important risk factor for BC (Knight et al., 2002), and GSTs are involved in the metabolism of various carcinogens presenting in cigarette smoke, so further analysis regarding smoking status was carried out. Intriguingly, the results of present meta-analysis showed no significant increase in risks of BC for smokers and nonsmokers with the GSTT1 null genotype, and, besides, smoking was not shown to be a modifying factor of the association between the GSTT1 null genotype and BC risk. The possible reason could be that the GSTs are various enzymes responsible for the detoxification of mutagenic electrophiles (van der Hel et al., 2003), so even though only one gene carried a single-nucleotide polymorphism, the activity of all GSTs is unlikely to change significantly.
Among GST family, the polymorphism of GSTM1 with the risk of BC was also extensively studied in humans. Several meta-analyses (Johns and Houlston, 2000; Engel et al., 2002; Jiang et al., 2011; Zhang et al., 2011) suggested that the GSTM1 null genotype is associated with a higher incidence of BC. In our study, 12 of 50 studies examined the combination of GSTT1 null and GSTM1 null genotypes and the result proved a remarkable association between the combinations of them with BC risk. This observation revealed that gene–gene interactions probably partially contribute to genetic susceptibility for BC. Besides, the GSTP1 was also comprehensively studied in the GSTs family, and two single-nucleotide polymorphisms (SNP) of GSTP1 have been described. Between them, which researched the most was the A-to-G substitution at base pair 313 at codon 105 resulting in an amino acid difference, from isoleucine to valine (Zimniak et al., 1994). In 2007, a meta-analysis (Kellen et al., 2007) including 16 studies showed that the GSTP1 Ile 105Val polymorphism seems to be associated with a modest increase in the risk of BC (OR=1.44, 95% CI=1.17–1.77, p<0.001). Afterward, there are seven new researches about this polymorphism with BC, so we updated the result. Without doubt, our updated result still suggested a dramatic increase in risk of BC with presence of GSTP1 Ile 105Val polymorphism (OR=1.25, 95% CI=1.06–1.46, p=0.007).
In recent years, the application of the genome-wide association study (GWAS) in cancer-related studies has exploded. Until now, there are seven GWAS about BC (Kiemeney et al., 2008; Golka et al., 2009; Rafnar et al., 2009; Wu et al., 2009; Kiemeney et al., 2010; Rothman et al., 2010; Rafnar et al., 2011), and two of them (Golka et al., 2009; Rothman et al., 2010) confirmed the association between the GSTM1 null genotype with BC risk, respectively, which is consistent with the former meta-analyses. However, the GSTT1 and GSTP1 polymorphisms with BC risk were not observed in these GWAS. The reasons of this phenomenon are possibly as follows: (1) as more than half of all common SNPs have at least 10 neighboring SNPs with an r 2>0.8, it is difficult to establish whether an identified variant is truly causal (International HapMap Consortium, 2005); the top scoring hits could just be correlated markers to other common variants or rare or structural variants (Ioannidis et al., 2009); (2) objects of the two GWAS were only including European descents, so the results may need to be confirmed in other independent populations, and then some new but emerging information would be found; (3) the requirements for large sample size typically for multiple validation stages and the high genotyping cost probably restrict the prediction accuracy of the GWAS results. However, besides the already confirmed loci, it was estimated that there would be an additional two dozen BC susceptibility SNPs of similar risks and frequencies to be identified (Park et al., 2010; Rothman et al., 2010).
Although the previous meta-analysis has investigated GSTT1 polymorphism and BC risk, our study was more stringent and comprehensive. First, more up-to-date studies (50 studies) were recruited to provide statistically significant results. Second, we performed in detail to check into the association among different ethnic groups and suggested that the role of the GSTT1 null genotype on BC susceptibility totally differed between Caucasians and some Asian countries (Korea and Japan). Third, our result revealed a strong association between BC risk and the combination of GSTT1 null with GSTM1 null genotypes.
Some limitations of this meta-analysis should be acknowledged. First of all, only published studies were included; therefore, the publication bias may have occurred. The result of Egger's test provided statistical evidence of that. It is known that positive results usually have a greater probability of being published, and such bias may occur when studies with null or unexpected results, which in most instances, leading to their not being published or included in the meta-analysis. Second, heterogeneity among the studies was extreme and the reasons could be the study design, the source of controls, the differences of genetic backgrounds, and the environment existed among different ethnicities. Third, the sensitivity analysis showed that the result of population-based controls was unstable, so we should explain it prudently. Fourth, the overall outcomes were based on individual unadjusted OR, while a more precise evaluation need to be adjusted by other potentially suspected factors. Finally, meta-analysis remains as retrospective research that is subject to the methodological deficiencies of the included studies. We tried to develop a detailed protocol before initiating the study, and then performed a meticulous and explicit method for study researching, selection, data extraction, and data analysis to minimize the likelihood of bias.
Conclusion
Our meta-analysis suggested that the GSTT1 null genotype is associated with an enhanced risk of BC. Specifically, an increased BC risk with the GSTT1 null genotype was observed among Caucasians, but a decreased risk was revealed among some Asian countries (especially in Korea and Japan). No significant gene–smoking interaction was detected for the GSTT1 null genotype with BC risk. In addition, our results showed a strong association between BC risk and the combination of GSTT1 null with GSTM1 null genotypes. However, further well-designed, high-quality epidemiological studies with larger populations in the future will be needed to confirm our findings.
Footnotes
Disclosure Statement
No competing financial interests exist.