
Abstract
Polymorphisms of the DNA repair gene X-ray repair cross-complementing protein 1 (XRCC1) Arg194Trp, Arg280His, and Arg399Gln have been shown to alter the DNA repair activity and to be associated with genetic susceptibility to several types of cancer. We indentified genotypes of 944 surgically resected gastric cancer (GC) patients by the SNaPshot method to investigate the association of these polymorphisms with clinical progression and outcomes of GC in a Chinese population. The XRCC1 codon 280 His carriers (Arg/His+His/His) held a significantly lower risk of distant metastasis in the dominant model (Pearson chi-square test P=0.019). A weak association of these cases with reduced risk of lymph node metastasis was also found (Pearson chi-square test P=0.051). Individuals carrying at least one Trp allele of XRCC1 codon 194 had an increased risk of death compared with those with Arg/Arg homozygotes in diffuse-type GC (adjusted hazard ratio=1.34, 95% confidence interval=1.05–1.71). Our findings demonstrated that the genetic variant Arg280His in XRCC1 may contribute to cancer progression and that XRCC1 Arg194Trp variants may act as a favorable prognostic indicator of resected GC, particularly among the diffuse-type GC. Larger studies are needed to verify our results in different populations.
Introduction
Oxidative stress-induced DNA base damage caused by endogenous and exogenous sources involves in human carcinogenesis (Kryston et al., 2011). Repair of these base lesions occurs primarily by base excision repair (BER) pathway (Hazra et al., 2007), and increasing evidence has shown that defects in human BER proteins are implicated in the development of malignant tumors (Tudek, 2007). XRCC1 protein, acts as a scaffold protein, can recognize DNA breaks, bind the DNA and recruit other partners in BER pathway to mediate repair in a coordinated fashion (Kubota et al., 1996; Taylor et al., 1998; Campalans et al., 2005). Its deficiency in mice induces embryonic lethality, further highlighting the crucial importance of this protein (Hoeijmakers, 2001). Low XRCC1 expression has also been reported, respectively, in patients with pancreatic cancer and GC (Crnogorac-Jurcevic et al., 2002; Wang et al., 2012). Currently, increasing molecular epidemiologic studies indicate that single-nucleotide polymorphisms (SNPs) of XRCC1 were correlated with the risk of various cancers, including GC (Chen et al., 2012), whereas few studies were conducted to explore implications of these genetic variations on tumor biological behavior or survival time (Huang et al., 2009; Tahara et al., 2011; Shim et al., 2010). The XRCC1 gene is located on chromosome 19q13.2–13.3 with 33 kbp in length (
Materials and Methods
Study population
A retrospective cohort of 944 histopathologically confirmed GC patients who underwent a surgical resection at the Yixing People's Hospital (Yixing, Jiangsu Province, China) between 1999 and 2006, were eligible for the present study. Formalin-fixed and paraffin-embedded blocks of these patients were collected from the department of pathology of this hospital. None have received neoadjuvant radiochemotherapy or postoperative radiotherapy, and not all of them had received adjuvant chemotherapy. At the time of the last follow-up in March 2009, the maximum survival time was 119.0 months and the median survival time was 70.0 months. From the medical records of patients, we obtained detailed demographic and clinicopathological information, which are summarized in Table 1. The end point was overall survival (OS) that was defined as the time between the first day of surgery and the last follow-up or the date of death. Death dates were confirmed via review of death certificates of inpatient and outpatient records or obtained from patients' families through follow-up telephone calls. Patients still alive on the last follow-up date were censored on that date. All participating subjects provided written informed consent on the use of paraffin specimens for gene polymorphism analyses, and the study was approved by the Institutional Research Board at Nanjing Medical University (Nanjing, China).
Four patients with gastrointestinal stromal tumor and lymphoma were excluded.
The information about the depth of invasion was not available for two patients; invaded depth of tumor was classified according to the criteria of AJCC 7th.
Lymph nodes were staged according to tumor node metastasis classification of the 7th edition of AJCC in which the number of lymph nodes with a metastasis of 1–2, 3–6, and ≥7 were classified as N1, N2, and N3, respectively.
Mean survival time was presented when the median survival time could not be measured.
MST, median survival time; HR, hazard ratio; CI, confidence interval; AJCC, American Joint Commission on Cancer.
Significant results are highlighted in bold-ital font.
Genotyping
The genomic DNA was extracted from paraffin-embedded tumor bearing tissue using proteinase K digestion, followed by isopropanol extraction and ethanol precipitation (Wang et al., 2011). Genotyping of samples was conducted by the SNaPshot method (Applied Biosystems), which consists of multiplexed polymerase chain reaction (PCR) and multiplexed single-base extension reactions, followed by capillary electrophoresis. Primer sequences for these variants are available upon request. The PCR multiplexes were carried out in 10 μL final volume, including 5 μL SNaPshot Multiplex Kit (Applied Biosystems), 2 μL purified PCR product, 1 μL compound of the extension primer, 2 μL high purity water. The SNaPshot products were separated using capillary electrophoresis on an ABI 3130xl genetic analyzer (Applied Biosystems) and the data was analyzed by GeneMapper Analysis Software version 4 (Applied Biosystems). Assessment of genotypes was carried out independently by two investigators blinded to the survival end points. About 10% of randomly selected DNA samples were analyzed at least twice, and the results were 100% concordant.
Statistical analysis
Associations of genetic variants and clinicopathological features with the OS were estimated using Kaplan–Meier method and comparisons between different groups of patients were performed with the log-rank test. Univariate or multivariate Cox proportional hazard models was used to estimate the crude hazard ratio (HR), adjusted HR and their 95% confidence interval (CI). Moreover, Cox stepwise regression analysis was conducted to estimate the independent impacts of the polymorphisms or clinicopathological features on the OS, after adjusting for other covariates. The independent-sample Student's t-test was used for comparison of age at time of surgery, while four-by-four tables were used to analyze the association between the genetic variants and other clinicopathological features. If all the theoretical frequencies in one table were ≥5, then the analysis was performed by using Pearson chi-square test. If there was at least one <5, then the two-sided Fisher exact test was chosen. All analyses were carried out by SPSS software 16 (SPSS Inc.) and a two-sided P-value of 0.05 was adopted for all the statistical analyses. The linkage disequilibrium (LD) of XRCC1 gene SNPs were assessed using the SHEsis software platform online (Li et al., 2009). The extent of LD was estimated by r 2, which can range from 0 (random coinheritance of alleles) to 1 (complete LD). Values<0.33 suggest absence of strong LD (Ardlie et al., 2002).
Results
Association between clinicopathological characteristics and OS
We made a statistical analysis of contributions of clinicopathological features to GC survival in a population of 944 patients. All individuals suffered from surgical resections. There were 727 men (77%) and 217 women (23%) and the median age was 62 years ranging from 28 to 83 years. The patient characteristics and clinical features of the tumor are summarized in Table 1. Clinicopathological characteristics, including tumor size, histological types, T category, N category, distant metastasis as well as TNM stage were significantly correlated with OS (log-rank P<0.05). Further, as the penetration grade and TNM stage increased, the risk of death for GC showed a significant increase in a dose-response manner, respectively (for depth of tumor invasion, log-rank P<0.001; for TNM stage, log-rank P<0.001).
Association analyses of Arg194Trp, Arg280His, and Arg399Gln SNPs with clinicopathological features
Genotyping was successfully carried out in 911 subjects for Arg194Trp SNP, 928 subjects for Arg280His SNP, and 943 subjects for Arg399Gln SNP, respectively. The distribution of genotypes in the population was consistent with Hardy–Weinberg equilibrium (P=0.93 for Arg194Trp SNP, P=0.86 for Arg280His SNP, and P=0.13 for Arg399Gln SNP), while LD did not exist between alleles of the three loci with the following r 2 values: Arg194Trp/Arg280His=0.142; Arg194Trp/Arg399Gln=0.053; and Arg280His/Arg399Gln=0.037. No significant associations were observed between XRCC1 codon 194 and 399 polymorphisms and the clinicopathological features (data not shown). However, as shown in Table 2, the XRCC1 codon 280 His carriers (Arg/His+His/His) held a significantly lower risk of distant metastasis in the dominant model (log-rank P=0.019). A weak association of these cases with reduced risk of lymph node metastasis was also found (log-rank P=0.051).
There was at least one table of which the theoretical frequency was <5, and the two-sided Fisher exact test was used.
SD, standard deviation; Arg, arginine; Trp, tryptophan.
Significant results are highlighted in bold-ital font.
Association analyses of Arg194Trp, Arg280His, and Arg399Gln SNPs with OS
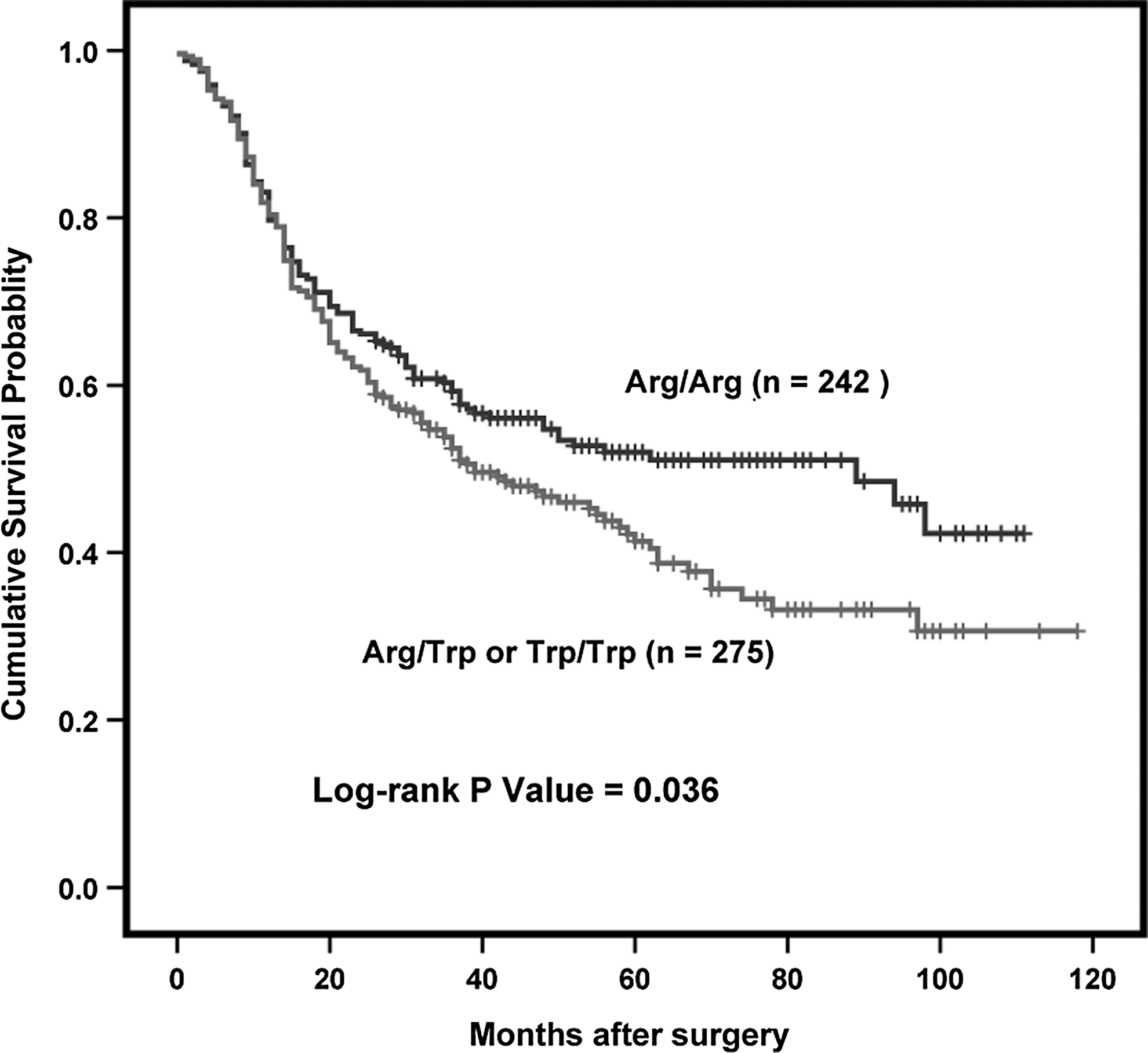
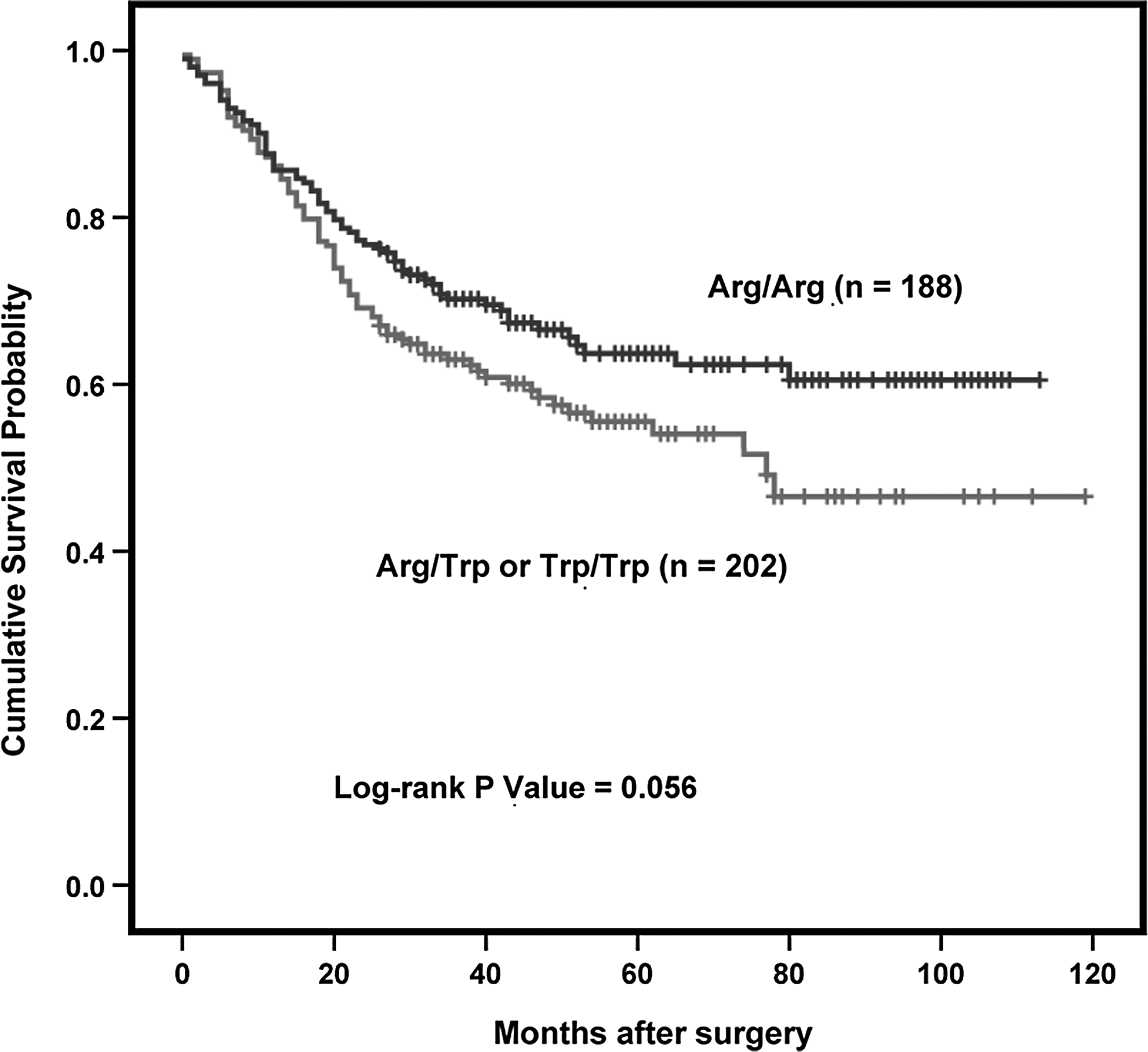
The survival analysis using Cox proportional hazard models showed that Arg194Trp, Arg280His, and Arg399Gln polymorphisms in XRCC1 gene were not correlated with the OS of all GC patients in any genetic models. Then, we further evaluated the association by subgroup analysis of anatomic location, histological types. As a result, no significant association of Arg280His and Arg399Gln polymorphisms with OS was found in the stratified analyses. Arg194Trp polymorphism was associated with poor prognosis among diffuse-type GC patients in a dominant model (log-rank P=0.036; Table 3 and Fig. 1), although no significant difference was observed among intestinal-type GC patients (log-rank P=0.056; Table 3 and Fig. 2). Cox stepwise regression analysis was conducted to evaluate the independent effect of clinicopathological variables and Arg194Trp polymorphism on the OS of the patients with diffuse-type GC. As shown in Table 4, two variables (lymph node metastasis and Arg/Trp polymorphism) were included in the regression model by stepwise selection of the categorical variables. Further, when age and sex were included in the final model, the Arg/Trp polymorphism was shown to be an independent poor prognostic factor for diffuse-type GC with a 36% increased risk of death (adjusted HR=1.36, 95%CI=1.06–1.73, P=0.02).
Overall survival (OS) curve in relation to XRCC1 Arg194Trp polymorphism in patients with diffuse-type gastric cancer (GC). Figure 2 represents the Kaplan–Meier survival curve in relation to the effect of XRCC1 194Trp variant on OS of the patients with diffuse-type GC. Patients with Arg/Trp or Trp/Trp genotypes was at higher risk of death, compared with those with Arg/Arg homozygote. P-value is 0.036, suggesting that significant differences were observed among diffuse-type GC.
Overall survival (OS) curve in relation to XRCC1 Arg194Trp polymorphism in patients with intestinal-type gastric cancer (GC). Figure 1 represents the Kaplan–Meier survival curve in relation to the effect of XRCC1 194Trp variant on OS of the patients with intestinal-type GC. Patients with Arg/Trp or Trp/Trp genotypes trended to have better survival than those with Arg/Arg homozygote, but the P-value of log-rank test did not receive statistical significance.
Multivariate Cox proportional hazard models was adopted to estimate the HR adjusted for age, sex, and TNM stage.
Significant results are highlighted in bold-ital font.
Age was included as a continuous variable in the Cox stepwise regression analysis.
SE, standard error.
Significant results are highlighted in bold-ital font.
Discussion
In our study, we have investigated the associations of three SNPs (Arg194Trp, Arg280His, and Arg399Gln) of XRCC1 gene with clinicopathological features and OS in a large population of patients with surgically resected gastric carcinoma. The XRCC1 codon 280 His carriers (Arg/His+His/His) held a significantly lower risk of distant metastasis in the dominant model. Moreover, these cases tend to have a reduced risk of lymph node metastasis. Although neither of these variants was found to be correlated with outcomes in all GC patients, our study demonstrated a significant association of Arg194Trp SNP with a decreased OS of diffuse-type GC in a dominant model.
XRCC1 protein, having no known enzymatic activity, functions as a scaffold protein that provides a platform upon which the necessary repair complexes can form, and plays regulative and coordinative role in consecutive stages of the BER pathway (Marsin et al., 2003). The role of XRCC1 has been mainly attributed to its interactions with a series of repair enzymes known to involve in BER and single-strand break repair machinery, including AP endonuclease-1 (APE1) (Vidal et al., 2001), DNA polymerase β (Kubota et al., 1996), DNA ligase III (Taylor et al., 1998), poly(ADP-ribose) polymerase 1 (PARP-1) (Murielle et al., 1998), PARP-2 (Schreiber et al., 2002), proliferating cell nuclear antigen (PCNA) (Fan et al., 2004), human oxoguanine glycosylase 1 (Marsin et al., 2003), as well as, nei endonuclease VIII-like 1 protein 2, N-methylpurine-DNA glycosylase, and neutral trehalase (Campalans et al., 2005). While PARP-1 and PARP-2 as well as APE1 and several glycosylases have been demonstrated to interact with deletions of XRCC1 that encompass Arg399 (Murielle et al., 1998; Vidal et al., 2001; Schreiber et al., 2002; Marsin et al., 2003; Campalans et al., 2005; Mansour et al., 2010), the functional significances of Arg280 and Arg194 are mainly attributable to their location within protein-binding domains that interact with PCNA, APE1, and glycosylases (Vidal et al., 2001; Marsin et al., 2003; Fan et al., 2004; Campalans et al., 2005; Mansour et al., 2010). Considering the importance of these repair proteins and their interactions with XRCC1 for a complete DNA damage repair process, it is proposed reasonably that noted three nonsynonymous mutations occurring within related protein-binding domains of XRCC1 gene, may change the protein structure, subsequently influence its activity (or affinity) to bind to other abovementioned partners, which in turn lead to the alterations of its communication with other enzymes as well as altered DNA repair capacity. Based on these evidences, we speculated that three SNPs may play an advance role in cancer carcinogenesis and development. Regrettably, in the current study, no significant association of 399Gln SNP with clinical progression and outcomes was observed. While patients harboring at least one variant allele (Arg/His+His/His) were found to be less likely to present distant metastasis than homozygous genotypes (Arg/Arg), 194Trp allele carriers conferred a poor survival for diffuse-type GC. For Arg280His SNP, Takanami et al. (2005) reported that Chinese hamster ovary EM9 cell lines transfected with XRCC1 280His alleles expressed the variant protein that was defective in its efficient localization to a damaged site in the chromosome and thereby reduced the cellular BER efficiency, which suggested that this SNP could identified as a risk factor for cancer development. Nevertheless, our finding that 280His carriers had less potential to metastasize seems to be inconsistent with the previous observation. It is conceivable that many other genetic and nongenetic factors involve in cancer carcinogenesis and development. The discrepancy between our finding and the previous study may be due to gene–gene and gene–environment interactions. Yin et al. (2007) reported that overall genotype and allele distributions of the XRCC1 Arg280His in patients with lung cancer were not significantly different from those in controls, but nonsmokers carrying genotypes of Arg/His or His/His had a significantly decreased risk of lung cancer. However, the results of a case–control study showed a significant association of the variant allele of XRCC1 Arg280His SNP with increased risk of gastric cardiac adenocarcinoma among smokers but not nonsmokers (Yan et al., 2009). These results further indicated that the polymorphisms of XRCC1 gene, together with other nongenetic factors, might contribute to the development and clinical progression of the cancer. Clearly, more functional studies are needed to clarify this issue and reconcile the different pieces of evidence. For Arg194Trp SNP, we speculated previously that the 194Trp may confer a negative effect on tumorigenesis. On the contrary, Wang et al. (2003) reported that individuals carrying one or two variant Trp alleles exhibited significantly fewer chromosomal breaks than those with Arg/Arg genotype due to the lower mutagen sensitivity of Trp allele, suggesting a protective role of this genetic mutation. Molecular epidemiologic studies on the contribution of this polymorphism to cancer susceptibility also showed conflicting results (Hung et al., 2005; Chen et al., 2012). In our study, XRCC1 194Trp genetic variant conferred a poor survival for diffuse-type GC, which is inconsistent with the abovementioned protective effect of this allele (Wang et al., 2003). Although the exact biological mechanisms of the alteration of the XRCC1 protein function due to specific gene variant remains unclear, the potential explanation of our finding is that individuals with Trp allele who had lower values of mutagen-induced chromosomal breaks would exhibit higher chemoresistance to genotoxic anticancer drugs, resulting in an inferior survival.
In the present study, XRCC1 Arg194Trp SNP was significantly correlated with poor survival of diffuse-type GC, but not intestinal-type GC. Lauren (1965) classified the great majority of GCs into two major types, the intestinal and the diffuse, based on tumor histology. Besides being histopathologically different, accumulating evidence suggests that the two types appear to differ with regard to their epidemiological, aetiological, and biological characteristics (Crew and Neugut, 2006; Zheng et al., 2007), suggesting that they should be treated with two distinct diseases and the indiscriminate combination of the two types may mask or underestimate the authentic associations. Our finding also fit with recently published meta-analysis, which indicated that XRCC1 Arg/Trp polymorphism contributes to susceptibility to GC (Chen et al., 2012). Therefore, it is unlikely that this association occurred by chance.
It has been widely accepted that Helicobacter pylori infection, causing DNA damage in gastric epithelial cells by producing reactive oxygen or nitrogen species, plays an important role in gastric carcinogenesis (Obst et al., 2000). Further, some investigators have focused on exploring the association of H. pylori infection status with the prognosis of GC, but their observations were inconsistent and required further confirmation in a larger multiethnic study (Meimarakis et al., 2006; Qiu et al., 2010). However, in our study, not all patients were detected H. pylori infection status, so we could not investigate the potential combined impact of H. pylori status and XRCC1 gene polymorphisms on the clinical outcomes of GC patients who underwent surgery due to lack of the relevant information.
Conclusion
Our findings showed that XRCC1 codon 280 His carrier status is correlated with less aggressive biological behavior of GC, such as distant metastasis, and that XRCC1 Arg194Trp variants could be identified as an independent prognostic marker in diffuse-type GC. Testing for XRCC1 Arg194Trp SNP, combined with other prognostic factors, such as lymph node metastasis and TNM stage may allow identification of GC patients who are at high risk of poor survival and consequently require rigorous postoperative follow-up. Larger multiethnical and multicenter studies are needed to validate our findings.
Footnotes
Acknowledgments
The work was partially supported by the National Natural Science Foundation of China (81071641, 30872084, and 30972444, 81201570, 81102089, and 81230068), Jiangsu Provincial 12th Five-Year Program on Developing Health by Technology and Education Project, and the Priority Academic Program Development of Jiangsu Higher Education Institutions (Public Health and Preventive Medicine).
Author Disclosure Statement
No competing financial interests exist.