
Abstract
Generalized aggressive periodontitis (GAP) is a subgroup of periodontal diseases among 20–35 years age group adults. Several studies have reported the association of interleukin-1β gene polymorphism with periodontal diseases among different populations. The present study aimed at investigating the presence of IL-1β polymorphism in GAP patients in Iran. Further, the presence of IL-1β +3954 gene polymorphism was evaluated in the GAP patients (n=26) and healthy individuals (n=26). All three genotypes (A1A1 [56%], A1A2 [28%], and A2A2 [16%]) were observed in healthy individuals, whereas only A1A1 (38.5%) and A2A2 (61.5%) were the genotypes observed in the patients. There was a significant positive association between distribution of IL-1β genotypes and the risk of periodontitis disease (p=0.017). Further, there was a significant positive association between probing pocket depth and IL-1β genotypes of patients (p=0.014). However, no meaningful correlation between genotype-clinical attachment loss and genotype bleeding on probing with the risk of GAP (p=0.418, p=0.819, respectively) was found. In conclusion, findings of the present study demonstrate a positive association between IL-1β gene polymorphism and risk of periodontitis disease.
Introduction
Results of several studies conducted by different research groups on different groups of patients have proved that genetic background can have a strong influence on susceptibility to periodontitis disease (Gonzalez et al., 2003; Brett et al., 2005; Droździk et al., 2006). Therefore, there have been several attempts to characterize genetic factors implicated in the progression of periodontal diseases and to evaluate a possible association between candidate genes and the severity of the disease (Li et al., 2004; Megha and Shaila, 2012). Genes that play an important role in the immune pathology of periodontal disease such as cytokine genes are the main candidates for the analysis of polymorphisms as well as possible associations with GAP (Galbraith et al., 1999). In recent years, several studies have demonstrated that periodontitis is associated with an elevated level of inflammatory cytokines (Galbraith et al., 1999). Cytokines as the main mediator of the immune system play a significant role in many biological activities, such as proliferation, development, homeostasis, gene regulation, repair, and inflammation (Guzeldemir et al., 2008). One of the well-studied cytokines whose variants are associated with periodontal disease occurrence is interleukin-1 genotype (Gonzalez et al., 2003). IL-1 genes family with two distinct but functionally similar types, IL-1α, IL-1β, are located in a cluster on the long arm of human chromosome 2q13 (Nicklin et al., 1994). IL-1β as an important mediator of immune system as well as a central pro-inflammatory cytokine has key roles in the pathogenesis of periodontal diseases (Nicklin et al., 1994; Kowalski et al., 2006).
Although the association between polymorphisms of the candidate genes with GAP in different ethnicities has been widely investigated (Li et al., 2004; Droździk et al., 2006; Guzeldemir et al., 2008; Prakash and Victor, 2010), there has been no published data on the possible association between the polymorphism of IL-1β and GAP among Iranian populations. Therefore, the present study aimed at investigating IL-1β +3954 genotype distribution and its association with periodontal disease among samples of GAP patients in Iran.
Materials and Methods
Enzyme and reagents
High-purity DNA extraction kit was purchased from Roche. Taq I as a restriction enzyme, agarose, and polymerase chain reaction (PCR) materials were purchased from Fermentas. The other chemicals and reagents were of analytical grade from Merck. Forward and reverse primers were synthesized from Symbion. All of the solutions were prepared in double-distilled water.
Sample collection
All procedures of the study were approved by the Ethics Committee of Gazvin University of Medical Sciences (Iran). Individuals who contributed to this research signed an informed consent in accordance with the principles of the Helsinki II declarations. All subjects were informed about their disease and the aim and procedures of the research. Evaluation of each participant was based on their own and family medical and dental history. Diagnosis of periodontal disease was according to the clinical and radiographic parameters, including bleeding on probing (BOP), probing pocket depth (PD), and clinical attachment loss (CAL). Exclusion criteria of the study were any history of human immunodeficiency virus and hepatitis infection, diabetes, usage of anti-inflammatory and anti-immune system drugs, pregnancy or lactation, and smoking. GAP was defined by interproximal attached loss, affecting at least three teeth that could be either first molars or incisors (Moreira et al., 2007; Guzeldemir et al., 2008; Khocht et al., 2011). Periodontal probe (Hu-Friedy PCP-UNC 15; Hu-Friedy) was used to measure the clinical parameters. The sample size of the study was defined based on the genotype frequency data of Drozdzik et al. (2006) and Guzeldemir et al. (2008). Therefore, with the distribution frequency of 30% (for A1A1 genotype) for the control group and 68% (A1A1 genotype) for the GAP group, as well as 80% power and an alpha value of 0.05, a sample size of 24 was calculated for each study group (n=24). There were a total of 26 unrelated patients suffering from periodontitis, which consisted of 87% women and 13% men. All subjects were from the School of Dentistry, Gazvin University of Medical Sciences (Gazvin, Iran). The control group consisted of 25 healthy volunteers. All patients and control subjects were free of general and genetic diseases.
DNA extraction
From each subject, venues blood sample containing 10 mL was collected using venipuncture and added into tubes containing ethylenediaminetetraacetic acid. Then, genomic DNA was extracted from whole blood samples using high-purity DNA extraction kit. Extracted DNA was verified by electrophoresis on 1% agarose gel (Kahrizi et al., 2007; Mirmoayedi et al., 2012). The concentration and purity of DNA were assessed with a Cecil UV-VIS spectrophotometer with 260/280 measurement ratio and at the wavelength of 260 and 280 nm, respectively (Mostafaie and Yari, 2011; Yari and Kahrizi, 2011).
PCR and analysis of IL-1β genotype
A 3 μL volume of extracted DNA was used as a template for PCR. A 182 bp fragment was amplified with the following primer pair (Guzeldemir et al., 2008): 5′ TCAGGTGTCCTCGAAGAAATCAAA3′and 5′GCTTTTTTGCTGTGAGTCCCG 3′. PCR was performed using Master Cycler Gradient-Eppendorf with 20 pmol of each primer, 3 μL of extracted DNA, 200 μM dNTPs, 1.5 mM magnesium chloride, 1 U Taq polymerase, and 2.5 μL of 10×PCR buffer with 25 μL final volume. The PCR thermal cycling parameters were 1 cycle at 94°C for 5 min, followed by 35 cycles at 94°C for 30 s, 53°C for 45 s, and 72°C for 75 s; then, the final cycle was continued for 10 min at 72°C as the last extension. The resulting PCR products were monitored using electrophoresis on 1% agarose gel containing ethidium bromide, and the predicted size of amplified DNA was confirmed using 100-bp molecular weight markers (Mostafaie and Yari, 2011; Rahimi et al., 2011). The PCR-restriction fragment length polymorphism (RFLP) was carried out using 2 U of Taq I at 65°C for 15 h. The homozygous genotype (A1A1) produces two fragments of 97 and 85 bp lengths, the homozygous genotype (A2A2) produces a fragment with 182 bp, while the heterozygous genotype (A1A2) produces three fragments of 182, 97, and 85 bp lengths that were diagnosed on 2% gel agarose.
Statistical analysis
The significant difference of the frequency of heterozygosity and homozygosity for genotypes between the GAP and control groups was evaluated by the Chi-square test. Quantitative parameters were expressed as means±standard deviation. Odds ratios were calculated to estimate the relative risk of disease, and 95% confidence intervals were measured by logistic regression in the statistical package of SPSS (version 18 for Windows). A two-tailed Student's t test analysis was used to compare the quantitative results. Statistical significance was set at the p<0.05 level. Statistical analyses of obtained results were performed using the SPSS (Rahimi et al., 2011).
Results
Twenty-six GAP patients and 25 healthy individuals participated in this study. The control group, 64% men and 36% women (mean age of about 23±2.5 years), were free from periodontitis signs. Further, the GAP group consisted of 87% women and 13% men with the mean age of 21±3.4 years. In patients, the mean of PD was 4.1±1.8 mm (7>PD>1.7); among them, 46.2% had PD <4 mm, 34.6% had 4–6 mm, and 19.2% had >6 mm. Mean CAL was 5.3±1.22 mm (8>CAL>3.8); 46.2% had 25–50 mm, 26.9% had 50–75 mm, and 26.9% had >75 mm. In addition, the mean of BOP was 52.9%±21.6% (30>BOP>85); 46.2% had 25%–50%, 26.9% had 50%–70%, and 26.9% had >70%. In the control group, mean CAL, BOP, and PD were 1.2±0.05 mm, 13.22%±6.89%, and 1.82±0.16 mm, respectively. DNA was extracted by DNA extraction kit as previously mentioned, and quality of extracted DNA was evaluated by gel electrophoresis (result not shown). To investigate the gene polymorphism, PCR-RFLP was carried out. Figure 1A shows the gel electrophoresis of PCR product of IL-1β with a 182 bp fragment. After gene amplification for its verification, gel electrophoresis of the digested PCR with TaqI was done (Fig. 1B). In the GAP group, the frequencies of A1A1 and A2A2 genotypes were 38.5% and 61.5%, respectively. However, none of the patients presented A1A2 genotype. In healthy individuals as the control group, the frequencies of A1A1, A2A2, and A1A2 genotypes were 56%, 16%, and 28%, respectively (Table 1). Therefore, all three IL-1β genotypes were found in the healthy individuals; however in the GAP cases, only A1A1 and A2A2 genotypes were presented. The analysis of results showed a significant positive correlation between the distribution of IL-1β genotypes and the risk of periodontitis disease (P=0.017). Further, there is a positive association between PD and IL-1β genotypes of patients (P=0.014). In the heterozygous genotype with PD 4–6 mm there was a higher frequency with 34.6%. However, no positive association was found between genotype-CAL (P=0.418) and genotype-BOP (P=0.819).
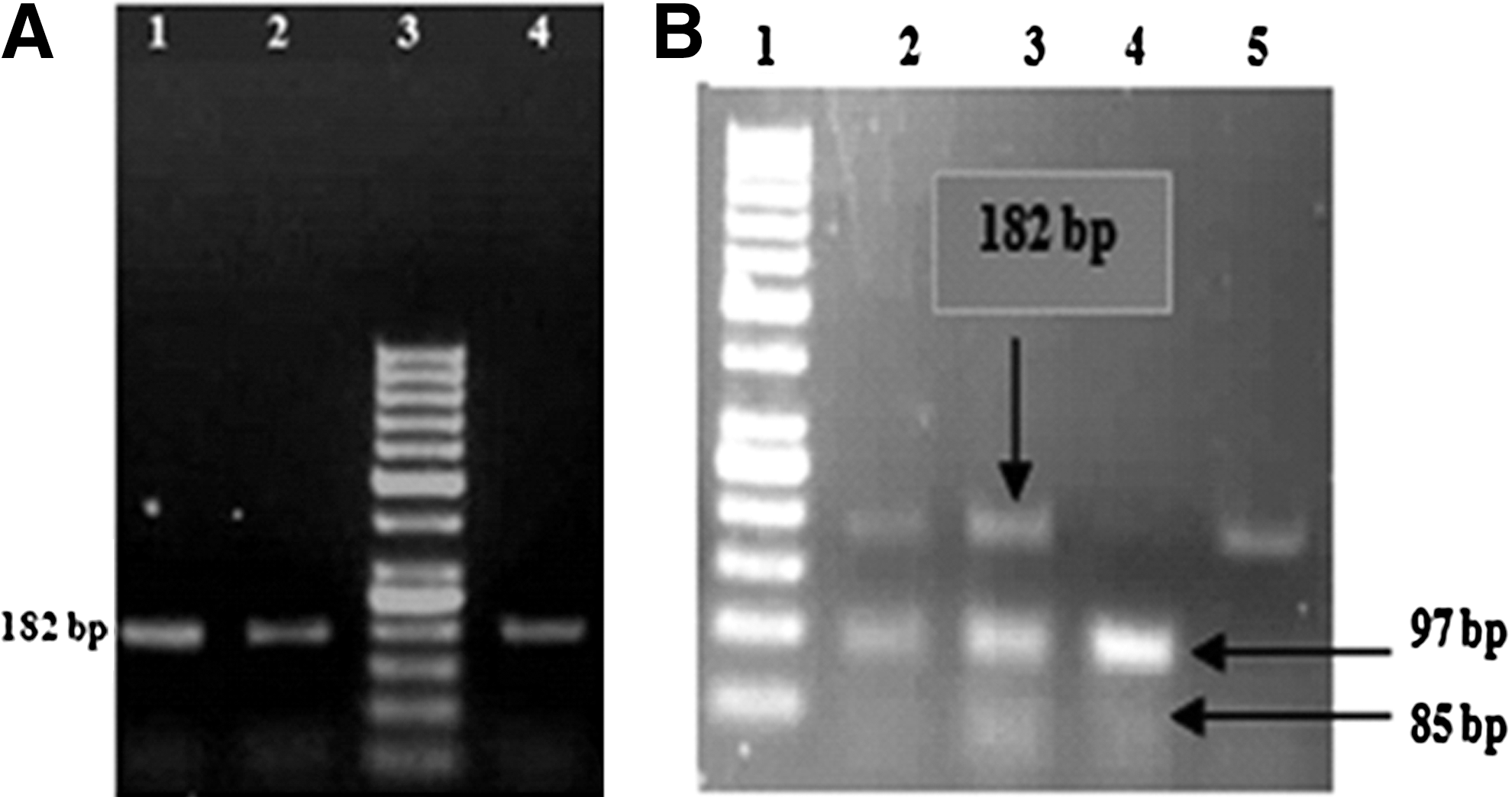
Agarose gel (2%) electrophoresis for amplified IL1A gene by PCR and digested product by Taq I restriction enzyme; 1A; from left to right, lane 1 shows 50 bp DNA molecular markers, lanes 2 and 3 show a 182 bp for PCR product band in patients group, lane 4 shows a 182 bp for PCR product band in healthy group. Figure 1B; lane 1 shows 50 bp DNA molecular weight markers; lanes 2 and 3 show the resulting product of 182 bp+ 97 bp and 85 bp (heterozygous); lane 4, 97 bp+85 bp (homozygous allele 1); lane 5, 182 bp (homozygous allele 2).
GAP, generalized aggressive periodontitis.
Discussion
GAP is a subgroup of periodontal diseases with local or global prevalence. It is a complex disease attacking adults in the age group of 20–35 years old with the damage of the first incisive and molar alveolar bone (Droździk et al., 2006; Sandra Sari and Suryono, 2009). Although the microbial and other environmental factors are essential for the initiation and development of the periodontal disease, several well-documented studies have demonstrated that genetic background seems to have a significant influence on the susceptibility and progression of periodontal disease in different ethnic groups (Galbraith et al., 1999; Gonzalez et al., 2003; Brett et al., 2005; Wagner et al., 2007; Kiani et al., 2009; Archana et al., 2012). Therefore, different studies have been conducted to evaluate the possible association between the polymorphism and genetic backgrounds of candidate genes with periodontitis diseases (Li et al., 2004; Kiani et al., 2009; Archana et al., 2012).
Since tissue destruction in periodontal disease is mostly because of self-inflammatory responses; cytokines as central mediators of this process are of great importance and have been recognized as a target of correlation analysis with the disease (Droździk et al., 2006; Khocht et al., 2011). Gene regulation in the IL-1 gene family, with such high frequencies of polymorphisms in the expression of either of its subtypes, would result in different levels of susceptibility to the disease between individuals (Li et al., 2004; Prakash and Victor, 2010). Based on documents in literature, IL-1α and -1β as two very considerable proinflammatory cytokines are considered most functional to the investigation of the association between the IL-1 gene polymorphism and periodontitis disease (Parkhill et al., 2000; Guzeldemir et al., 2008). The first study on the association between IL-1α (−889) and IL-1β (+3953) polymorphisms with periodontal diseases was reported by Kornman et al. (1997), who reported a positive association between the severity of periodontitis disease and composite genotypes of IL-1α and -1β. Following this, Walker et al. (2000) showed that the A1A1 genotype for IL-1β was carried by >99% of the control population and by 100% of the localized juvenile periodontitis group in African-American individuals. Gonzales et al. (2003) found that the A1A1 genotype for both IL-1α and IL-1β genes was the most common genotype in European Caucasians and Central American Hispanics populations. Drozdzik et al. (2006) showed that the prevalence of the A1A1 genotype of IL-1β was higher in the aggressive periodontitis and CP disease between periodontitis patients with either chronic or aggressive periodontitis and the controls in Polish population. However, no significant association was found. Consistent with these findings, Guzeldemir et al. (2008) reported that A1A1 was the highest prevalent genotype for IL-1β in localized aggressive periodontitis patients. Quappe et al. (2004) reported a significant association between aggressive periodontitis (AP) disease and being of the A2A2 genotypes in the Chilean population. In the Indian population, Gayathri et al. (2011) found that for cases and controls, the IL-1β (A2A2) genotype had a very low frequency of 2% and 1%, respectively. Therefore, based on the results of previous studies, the A2A2 genotype of IL-1β is associated with aggressive periodontitis and CP disease. The results of the present study showed that the frequency of the A2A2 genotype for IL-1β (+3954) was 61.5% in the GAP s group; however, in the control group, the frequency of the A1A1 genotype was higher than the A2A2 genotype. Similarly, Quappe et al. (2004) found that the A2A2 genotype of IL-1β was more common in AgP patients in the Chilean population. Therefore, based on our results along with the literature findings reported from various populations, frequency of IL-1β genotypes is different among ethnic groups (Moreira et al., 2007). Therefore, the polymorphic genotypes of the IL-1β gene may directly modify the cytokine synthesis to individuals' responses for bacteria stimuli and then influence the pathogenesis of periodontitis disease (Masamatti et al., 2012).
In the reported studies, GAP disease was more common in women compared with men, which is in agreement with the results of our study, where 87% of the patients were women. In accordance with our study, in a study of the Turkish population, Guzeldemir et al. (2008) reported that the 29 out of the 31 patients were women. The reasons for the high frequency of female GAP patients could be explained by the following reasons: hormonal alteration through menstrual cycle, pregnancy and also earlier age of puberty. Salvi et al. (2000) and Prakash and Victor (2010) found an association between the genetic polymorphism and the risk of GAP in smokers, and suggested that the effect of this risk factor is powerful even in individuals who are not genetically susceptible to the disease (Prakash and Victor, 2010). Therefore, to eliminate the effect of this risk factor, one of the exclusion criteria for sample collection was having a history of smoking in subjects.
In conclusion, the results of this pilot study showed that there was a significant positive correlation between the distribution of the IL-1β gene genotypes and periodontitis disease (P=0.017). In addition, our results show that the IL-1β genotype is an important risk factor that is associated with GAP in the Iranian population. However, further studies with a larger sample size are required to confirm these results. The present study is the first published study on the association between the IL-1β gene polymorphism and the risk of periodontitis disease in samples of the Iranian population. This study can be used as a basis for studying polymorphisms of other important genes in correlation to periodontitis disease.
Footnotes
Acknowledgments
The authors thank Professor Zohreh Rahimi, faculty member of Kermanshah University of Medical Sciences, and Miss Fatemeh Norooznezhad (M.Sc. student in Kermanshah University of Medical Sciences) for their useful comments in the preparation of the final revision of this article.
Disclosure Statement
No competing financial interests exist.