
Abstract
The multidrug resistance gene (MDR1) plays an important role in the transport of a wide range of drugs and elimination of xenobiotics from the body. Identification of polymorphisms and haplotypes in the MDR1 gene might not only help understand pharmacokinetics and pharmacodynamics of drugs, but also can help in the prediction of drug responses, toxicity, and side effects, especially, in the era of personalized medicine. We have analyzed the genotypic and haplotypic frequencies of the three most common single-nucleotide polymorphisms in the MDR1 gene in a sample of 100 unrelated healthy Moroccan subjects by polymerase chain reaction–restrictive fragment length polymorphism. The observed genotype frequencies were 43% for 1236CC, 49% for 1236CT, and 8% for 1236TT in exon 12; 49% for 2677GG, 47% for 2677GT, and 4% for 2677TT in exon 21; 39% for 3435CC, 51% 3435CT for 3435TT, and 10% for 3435TT in exon 26, respectively. We found that all polymorphisms were in Hardy–Weinberg equilibrium. Moderate linkage disequilibrium (LD) was observed between the three polymorphisms, the strongest LD in our study has been observed between C1236T and G2677T (D'=0.76; r 2=0.45). We identified eight haplotypes, the most frequent were 1236C-2677G-3435C (53%), 1236T-2677T-3435T (21%), and 1236C-2677G-3435T (10%), respectively. Our findings might facilitate future studies on pharmacokinetics of P-glycoprotein substrate drugs and interindividual variability to drugs in Moroccan patients.
Introduction
Materials and Methods
Subjects
Four milliliters of peripheral venous blood have been collected in the EDTA tube at the laboratory of genetic and molecular diseases, Faculty of Medicine, the Hassan II University in Casablanca on a total of 100 unrelated healthy participants (68 females and 32 males). The subjects were composed of Arabs (71%, n=71) and Berbers (29%, n=29) with a mean age of 31.78±12.94 years (range 18–77 years). The study was approved by the local Ethics Committee, and each participant agreed and signed informed consent.
Genotyping of MDR1 polymorphisms
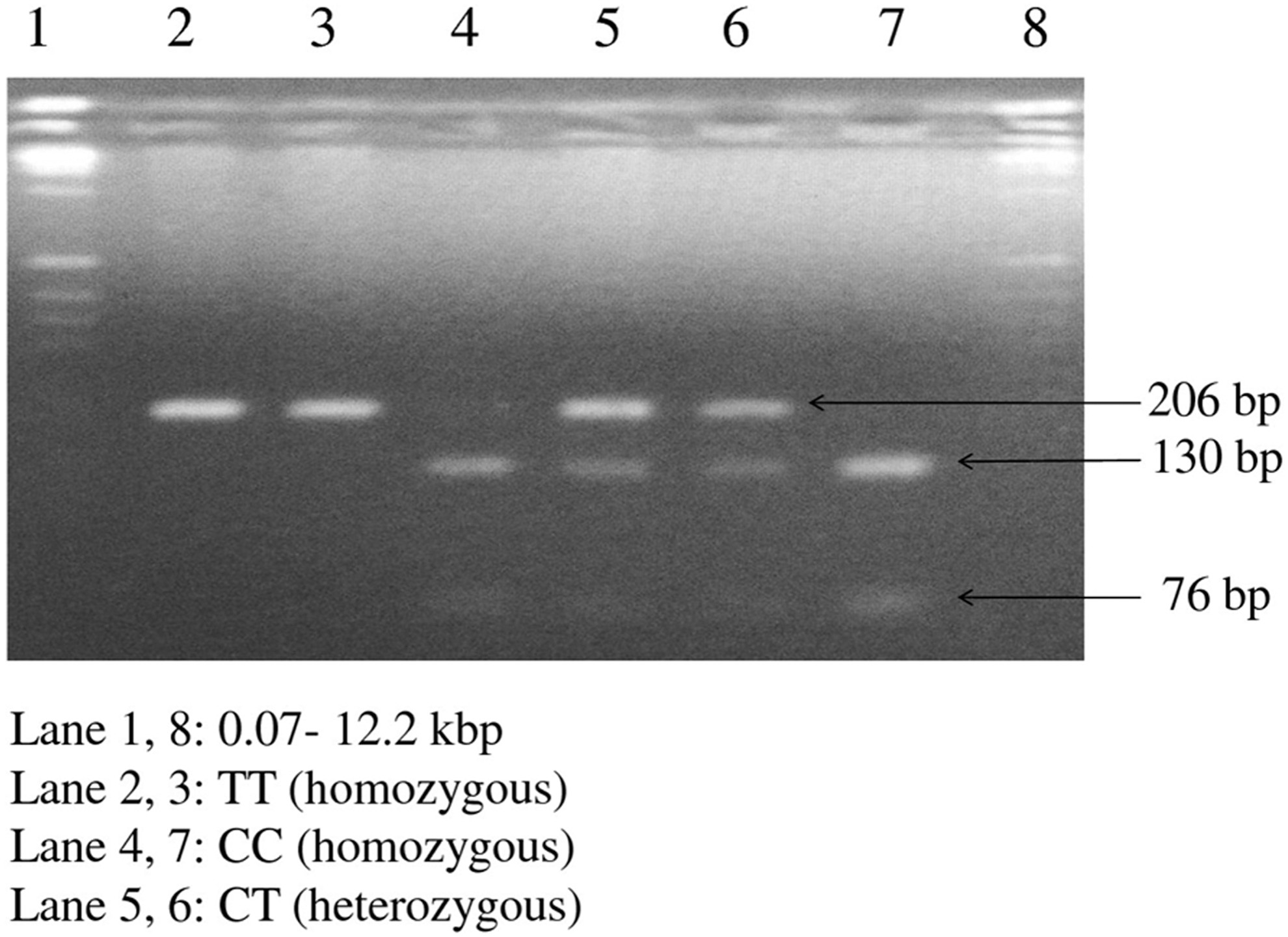
Genomic DNA was extracted from whole blood by the salting-out method previously described by Miller and Polesky (1988). The genotyping of the three SNPs was done by polymerase chain reaction–restrictive fragment length polymorphism (PCR-RFLP). The mixture consisted of 100 ng of DNA, 1×of 5×GoTaq Flexi Buffer (Promega), 1.25 mM MgCl2, 0.2 mM of each dNTP, 0.625 μM of each primer, 0.5 U Go Taq DNA polymerase (Promega) completed with sterile water to 25 μL. The primers used for C1236T (exon 12), G2677T/A (exon 21), and C3435T (exon 26) summarized in Table 1 were previously published by Cascorbi et al. (2001) and Tanabe et al. (2001). The PCR amplification was performed with an initial denaturation at 94°C for 5 min followed by 35 cycles of three steps: denaturation at 95°C for 90 s, annealing at 55°C for 60 s, extension at 72°C for 90 s, and a final extension at 72°C for 7 min. Negative controls (tube without DNA) were included in all reactions. PCR products were run on a 1% agarose gel (expected sizes are summarized in Table 1); the digestion was carried out with 10 units of restriction enzymes HaeIII, BanI, BsrI, and MboI for 16 h. The digestion products were analyzed on a 3% agarose gel stained with 0.5 μg/mL ethidium bromide (Figs. 2, 3, and 4). The enzymatic restriction conditions and digestion product sizes are summarized in Table 1.
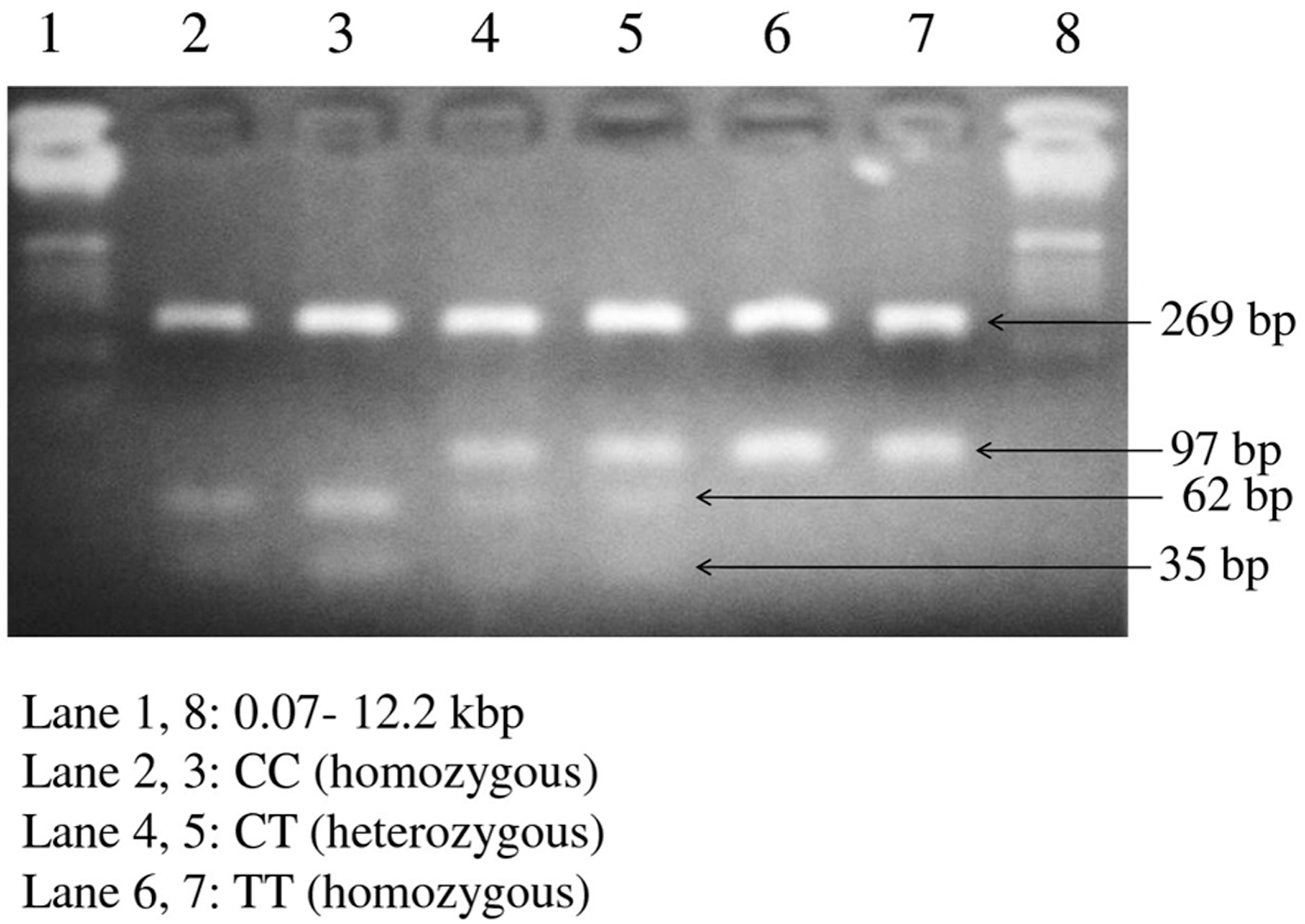
Different profiles of MDR1 gene polymorphism in exon 12 (C1236T) on a 3% agarose gel.

Different profiles of MDR1 gene polymorphism in exon 21 (G2677T) on a 3% agarose gel.
Different profiles of MDR1 gene polymorphism in exon 26 (C3435T) on a 3% agarose gel.
Wild-type homozygote.
Wild/variant heterozygote.
Homozygote mutant variant.
T°, digestion temperature; PCR-RFLP, polymerase chain reaction–restrictive fragment length polymorphism; SNP, single-nucleotide polymorphisms.
Statistical analysis
The statistical package SPSS version 16 (SPSS, Inc.) has been used to estimate possible combinations between different genotypes. SNPAnalyzer 2.0 was used to determine the allelic and genotypic frequencies as well as for the Hardy–Weinberg equilibrium test. A p value less than 0.05 was considered as significant. Expectation maximum algorithm from the same SNPAnalyzer 2.0 was used to identify haplotypes and establish their frequencies and finally to do LD analysis between SNPs (Yoo et al., 2008).
Results
In this study, 100 healthy individuals have participated, allelic and genotypic frequencies of C1236T, G2677T, and C3435T of the MDR1 gene are summarized in Table 2. The observed genotype frequencies were 43%, 49%, and 8% for 1236CC, 1236CT, and 1236TT in exon 12; 49%, 47%, and 4% for 2677GG, 2677GT, and 2677TT in exon 21, respectively. However, no variant of G2677A was observed. In exon 26, genotypic frequencies were 39% for 3435CC, 51% for 3435CT, and 10% for 3435TT, respectively. The observed allelic and genotypic frequencies did not deviate from those expected at Hardy–Weinberg equilibrium (Table 2). The relative frequencies of different combinations between the three SNPs are summarized in Table 3, we found out that 27%–35% of our subjects were wild type, 32%–35% were heterozygous, and 3%–4% were mutants when SNPs were considered in pairwise combinations. The LD between the three SNPs was moderate, the LD (D') and Pearson correlation coefficient (r 2) between C1236T and G2677T were 0.76 and 0.45; between C3435T and G2677T were 0.72 and 0.36; between C1236T and C3435T were 0.55 and 0.26 (Table 3). Of the 100 subjects, 8 haplotypes were observed; the three most common haplotypes were 1236C-2677G-3435C (53%), 1236T-2677T-3435T (21%), and 1236T-2677G-3435T (10%) (Fig. 1).
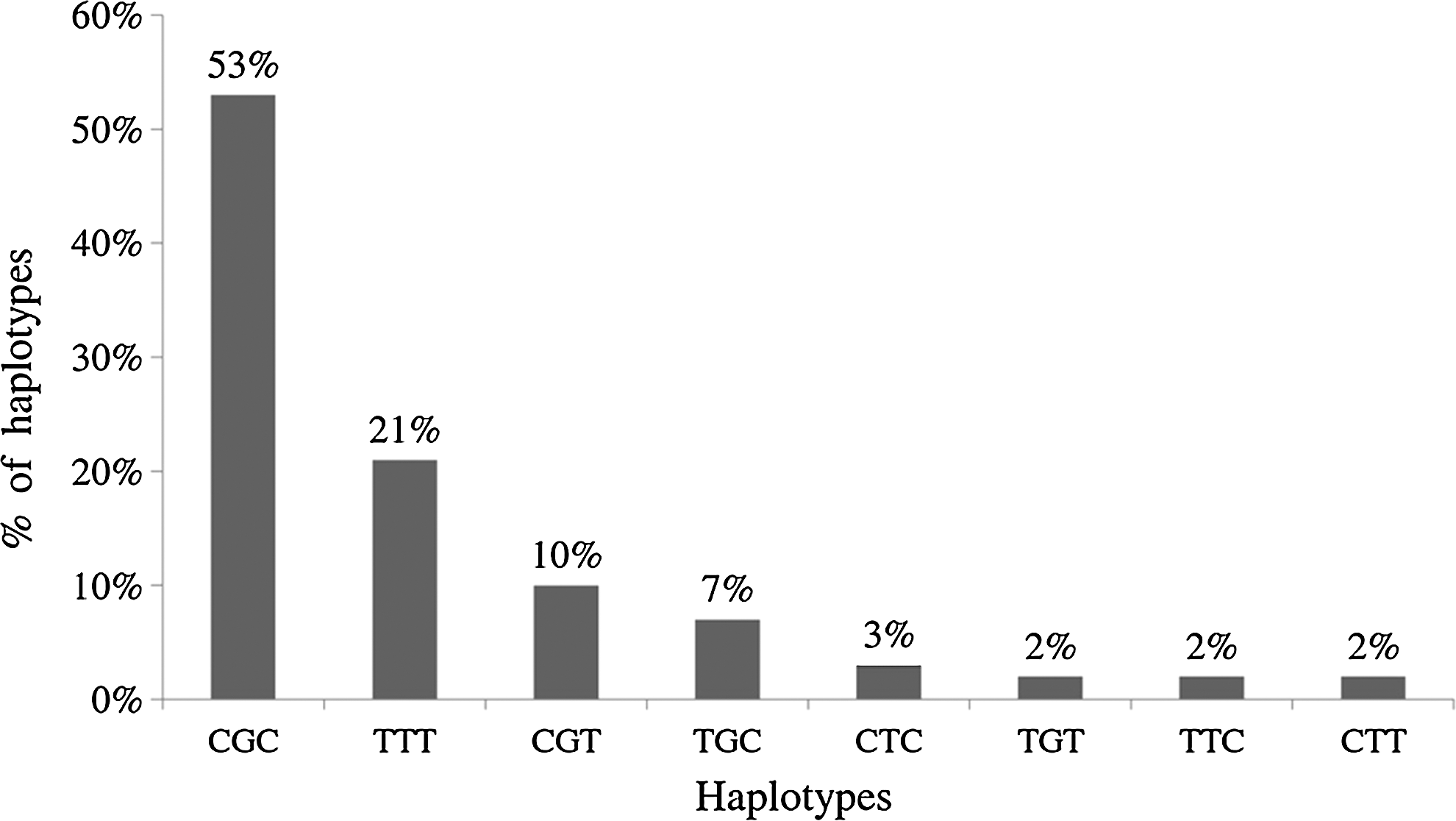
Haplotype distribution in the Moroccan population from exon 12 (C1236T), exon 21 (G2677T/A), and exon 26 (C3435T) of the MDR1 gene.
χ 2, Chi-square (Hardy–Weinberg test with df=1); df, degree of freedom.
The bold values show the probability of an individual having the same type of genotype variant from two SNPs.
N, number of combinations; f, frequency of combinations; D', linkage disequilibrium; r 2, correlation coefficient.
Discussion
Research on genes involved in drug absorption, distribution, metabolism, and excretion helps understand the pharmacokinetics and pharmacodynamics of drugs. The polymorphisms in the MDR1 gene are increasingly explored today. Moreover, several studies have shown the importance of the three most common SNPs of the MDR1 gene in response to drugs (Ling-Na et al., 2011; Yan et al., 2011; Munshi, 2012; Vivona et al., 2012) and their involvement in the development of certain diseases (Cizmarikova et al., 2010; Sabahi et al., 2010; Khedri et al., 2011). The 2677G>T/A polymorphism in exon 21 leading to amino acid change was the first SNP described, this SNP changes the amino acid (Ala893Ser/Thr) (Mickley et al., 1998). Two years after Hoffmeyer et al. (2000) have described systematically 15 SNPs, including a silent SNP (3435C>T) in exon 26, which was found to influence protein expression and digoxin transportation. Currently, the number of SNPs identified in the MDR1 gene is more than 50 and 3 insertions/deletions (Brinkmann et al., 2001; Saito et al., 2002; Evans and McLeod, 2003; Schwab et al., 2003).
In the present study, the frequency of the wild-type 1236CC in exon 12 is greater than that observed among Caucasians and Asians, but less than that observed among Ghanaians. However, the frequency of 1236CT is comparable with that observed in other countries outside Serbia and Ghana. The frequency of the homozygous mutant 1236TT in our population is less than that observed among Caucasians and Asians except Ghanaians (Table 4). Even though this SNP (Gly412Gly) is a silent mutation, the 1236TT genotype has been linked with a reduced clearance of docetaxel (Bosch et al., 2006) and also in early response to prednisone (Wasilewska et al., 2007). It has been shown that patients with chronic myeloid leukemia carrying the 1236TT genotype respond better to imatinib (Dulucq et al., 2008). However, this silent mutation in some cases has no impact in drug metabolism as demonstrated by Zhang et al., (2008) in valacyclovir uptake. The results obtained in this study could contribute to identify the good responders and furthermore to predict the patients response to these drugs.
N, number of samples tested; Na, not assessed.
In exon 21, the frequency of the 2677GG genotype is higher than that observed in Caucasians and Asians, but lower compared with Ghanaians and African-Americans, while the frequency of heterozygous 2677GT is similar to that of Caucasians, Saudis, and Turks. However, the frequency of 2677TT remains significantly lower than that observed in Caucasians, Asians, and Saudis. We have not found any variant of A allele in the locus 2677, the failure to detect this variant could be explained by our sample size (100) and by the fact that this SNP seems to have a geographical distribution as it is the case in the Ghanaian population and African-Americans who are from Africa (Table 4). Pan et al., (2008) have noticed that patients with nonsmall cell lung cancer harboring the 2677GG genotype respond better to chemotherapy compared to other groups; a similar finding was obtained in patients with small cell lung cancer (Sohn et al., 2006). Therefore, the identification of this SNP, which leads to amino acid exchange, might be helpful in the classification of our patients with small or nonsmall lung cancer before chemotherapy.
In exon 26, the frequency of the wild-type 3435CC is higher than that observed in Caucasians and Asians, similar to that in Saudis and Egyptians, outstandingly lower than that observed in Ghanaians. The heterozygous (3435CT) frequency is similar to that observed in Egyptians, Asians, and Caucasians, except Indians, but higher to that observed in Ghanaians. The frequency of homozygous variant type (3435TT) is close to that observed in the Egyptian population, lower than that observed in Caucasians and Asians, but higher than that observed in the Ghanaian population (Table 4). The overdominance of the 3435CC genotype is reported in African people (Ghanaians, Kenyans), and it is supposed to be a positive consequence of natural selection protecting against gastrointestinal tract infections (Mickley et al., 1998; Schaeffeler et al., 2001). It is reported that the 3435CC genotype is associated with a better response to Vinorelbine-based chemotherapy in nonsmall lung cancer patients (Pan et al., 2008). As seen in our results, 39% of our population with nonsmall lung cancer could respond better than the other variants.
Several studies have found LD between C1236T, G2677T, and C3435T polymorphisms in the MDR1 gene (Hoffmeyer et al., 2000; Kim et al., 2001; Allabi et al., 2005; Zhang et al., 2008; Al-Mohizea et al., 2012). Indeed, our data show similar results with a moderate LD. It was shown that clustering MDR1 SNPs into haplotypes will contribute to a better estimation of the functional value of the MDR1 gene at a clinical level and understanding the contradictory studies on MDR1 gene expression (Kim et al., 2001). Thus, several studies have explored the clinical impact of the MDR1 gene haplotypes. Potocnik et al., (2008) have reported that patients harboring both the 1236TT and 2677TT genotypes were linked to a higher microsatellite instability in colorectal cancer compared to controls; as shown in Table 3, 4% of our population carry this haplotype. Therefore, screening this haplotype in our patients with colorectal cancer may help to identify the high microsatellite instability risk group. As shown in figure 1, the 1236C-2677G-3435C (CGC) haplotype in our study represents the most common with 53%. The frequency of this haplotype is higher than that observed in Caucasians, Asians, and Saudis, but lower than those observed in Ghanaians and African-Americans. Dulucq et al., (2008) have found that the CGC haplotype is associated with a poor molecular response to imatinib in chronic myeloid leukemia patients. Hence, the identification of this haplotype in our patients undergoing imatinib treatment will help predict the response to imatinib. The second most common haplotype represented by the 1236T-2677T-3435T (TTT) 21% is lower than those observed in Caucasians, Asians, and Saudis, but higher than observed among Ghanaians and African-Americans (Kim et al., 2001; Tang et al., 2002., Kudzi et al., 2010; Al-Mohizea et al., 2012). Woillard et al., (2010) have reported that patients who have benefited from grafts from a donor carrying the TTT haplotype are significantly exposed to graft loss compared to patients who have received their grafts from donors carrying the CGC haplotype. Therefore, the haplotypes determination of the MDR1 gene could facilitate the identification of suitable donors for patients undergoing renal transplant.
Our results suggest that the Moroccan population retains an intermediate position in the distribution of the 3 SNPs. This fact could be explained by the ethnic composition (Arabs and Berbers) and the historical influence of sub-Saharan Africa through the trans-Saharan commercial trade (Abitbol, 1980) with possible gene flow. Therefore, other studies are needed to establish the functional impact of these SNPs and haplotypes on the pharmacokinetics of drugs that are substrates of the MDR1 gene in Moroccan patients.
Conclusion
We have established the allelic, genotypic, and haplotypic frequencies of three major polymorphisms of the MDR1 gene from a sample of the Moroccan population. Overall, we have found that the distribution of the C1236T, G2677T, and C3435T SNPs conserves an intermediate position compared to Caucasians, Asians, and Sub-Saharan Africans. This determination of functional polymorphisms of the MDR1 gene in our healthy population could be a starting point to facilitate future research on pharmacokinetics and pharmacodynamics of drugs that are MDR1 substrates.
Footnotes
Acknowledgments
We authors thank the Hassan II Academy of Science and Technology for providing us with financial support for this study.
Disclosure Statement
No competing financial interests exist.