
Abstract
This meta-analysis aims to evaluate the relationships between serum vascular endothelial growth factor (VEGF) level and radiosensitivity in patients with nonsmall cell lung cancer (NSCLC) among Asians. We searched CISCOM, CINAHL, Web of Science, PubMed, Google Scholar, EBSCO, Cochrane Library, and CBM databases from their inception through October 1, 2013. Meta-analysis was performed using the STATA 12.0 software. Fourteen clinical studies were included in this meta-analysis, including five case–control studies and nine cohort studies. Our meta-analysis results revealed that levels of serum VEGF in NSCLC patients were higher than that of healthy controls. There was a significant difference in serum VEGF levels between before and after radiotherapy in NSCLC patients. Further, we found significant differences in serum VEGF levels between effective and noneffective clinical response groups pre- and postradiotherapy. Serum VEGF levels showed no significant associations with tumor–node–metastasis (TNM) stage and histologic grade in NSCLC patients. NSCLC patients with positive VEGF expression had shorter overall survival than those with negative VEGF expression. Our meta-analysis suggests that serum VEGF level may be a useful biomarker in predicting radiosensitivity and prognosis of NSCLC patients among Asians.
Introduction
L
It is well established that the balance between apoptosis and tumor cell proliferation in invasive tumors depends on the ability of tumors to induce neovascularization to provide oxygen and nutrition for the malignant tumor cells (Bremnes et al., 2006). Generally, neovascularization promotes the progression of tumor by delivering nutrients and oxygen necessary for tumor cells to grow, facilitating the penetration of tumor cells through vessel walls and eventually leading to metastasis to distant organs, and secreting cytokines and growth factors from endothelial cells that stimulate tumor cells (Choi et al., 2001; Jones and Thompson, 2009). Therefore, angiogenesis is necessary for the growth and invasion of primary tumor and is also an essential step in tumor metastasis (Weis and Cheresh, 2011). An increasing number of angiogenic cytokines released by tumor cells have been identified over the years, including fibroblast growth factor, VEGF, transforming growth factor-α, platelet-derived endothelial cell growth factor, and hepatocyte growth factor (Senger, 2010; Carmeliet and Jain, 2011). Among these angiogenic factors, VEGF is a potent and commonly circulating vascular angiogenic peptide (D'Andrea et al., 2010).
VEGF, a member of the platelet-derived growth factor family, is a highly specific mitogen in vascular endothelial cells, which have been implicated in endothelial cell proliferation and migration, and plays crucial roles in modulating host response and tumor invasion, metastasis, and prognosis (Saharinen et al., 2011; Freeman et al., 2012). Consequently, VEGFs are considered to be prime regulators of both physiological and pathological angiogenesis in malignancy and function significantly in the regulation of tumor angiogenesis and development (Niers et al., 2011; Sina et al., 2011; Weis and Cheresh, 2011). VEGF expression has been demonstrated in a large variety of human malignancies including breast, liver, colorectal, bladder, and ovarian cancer (Tsutsui et al., 2010; Formica et al., 2011; Ji et al., 2012). Besides, in NSCLC, VEGF expression has been reported in over 50% of cases (de Boer et al., 2011). Meanwhile, high VEGF expression and angiogenic activity was noted in ∼30–40% of NSCLC (Yilmaz et al., 2007). High levels of serum VEGF induces the formation of neovascularization, allowing the tumor cells to infiltrate into the lymphatic vessels and neovascularization, and acceleration of distant metastases, and thence forming a vicious cycle (Thangarajah et al., 2009). There was mounting evidence that neoangiogenesis and blood VEGF levels in NSCLC patients may be negative prognostic indicators for survival (Carrillo-de Santa Pau et al., 2010; Salgia, 2011). Consistently, it has been shown that tumor angiogenesis and tumor growth was suppressed if VEGF signal transduction is inhibited (Ferrara, 2010). Such inhibition of the VEGF signaling may also prevent metastases because of reduced contact between tumor cells and the capillaries (Saharinen et al., 2011). Moreover, for majority of the radiotherapy-treated patients with advanced NSCLC, researchers observed a significant decrease in circulating VEGF in responders, while nonresponders showed increasing levels (Bremnes et al., 2006; Farhat et al., 2012). Clearly, it indicated that circulating levels of VEGF may be used in planning therapy, evaluating treatment effect, monitoring patients for relapse post-therapy in the future, and subsequently improve the sensitivity and accuracy of diagnosis in NSCLC remarkably (Zhou et al., 2009). However, there were only few studies focused on the levels of VEGF in sera of lung cancer patients and its effect on diagnostic sensitivity (Kaya et al., 2004; Steffensen et al., 2010). Many previous studies have indicated that high expression of serum VEGF may reduce radiotherapy sensitivity of NSCLC, but contradictory results were also reported (Zhang et al., 2008; Gu et al., 2011, 2013; Di et al., 2012). Given the conflicting evidence on this issue, we conducted a meta-analysis of all available studies to provide insights into the relationships between serum VEGF level and radiosensitivity in NSCLC patients.
Materials and Methods
Search strategy
We searched CISCOM, CINAHL, Web of Science, PubMed, Google Scholar, EBSCO, Cochrane Library, and CBM databases from their inception through October 1, 2013. The following keywords and MeSH terms were used: (“vascular endothelial growth factors” or “vascular endothelial growth factor” or “VEGF” or “vascular permeability factor” or “VPF”) and (“non-small-cell lung carcinoma” or “non-small cell lung carcinomas” or “non-small cell lung cancer” or “non small cell lung cancer” or “non-small-cell lung cancer” or “NSCLC”) and (“radiotherapy” or “chemoradiotherapy” or “RT” or “radiosensitivity”). We also performed a manual search of the reference lists to find other potential articles.
Selection criteria
In our meta-analysis, included studies must meet all the following criteria: (1) the associated study design must be a clinical cohort or case–control study; (2) the study must correlate to the relationships between serum VEGF level and radiosensitivity of NSCLC patients among Asians; (3) all patients diagnosed with NSCLC must be confirmed by histopathologic examinations; (4) the study must provide sufficient information about serum VEGF levels, patients' clinical responses, OS, and so on. If the study could not meet the inclusion criteria, it would be excluded. The most recent or the largest sample size publication was included when the authors published several studies using the same subjects.
Data extraction
Using a standardized form, relevant data were systematically extracted from all included studies by two researches. The standardized form included the following items: language of publication, article's publication year, the first author's surname, geographical location, design of study, sample size, source of the subjects, pathological subtype, detection method of serum VEGF, clinical response, and others. Staining for VEGF was assessed using a relatively simple, reproducible scoring method. The extent of the staining, defined as the percentage of positive stained areas of tumor cells in relation to the whole tissue area, is as follows: negative (<10%) and positive (≥10%). According to the Response Evaluation Criteria in Solid Tumors (RECIST) guideline (Eisenhauer et al., 2009), clinical response evaluation was categorized into four grades: (1) Complete response (CR): the complete disappearance of all measurable and evaluable disease, and with no new lesions and disease-related symptoms. (2) Partial response (PR): an at least 50% decrease in the sum of the product of the perpendicular diameters of measurable lesions from baseline, and with no development of new lesions. (3) Progressive disease (PD): an at least 50% increase (whichever is smaller) in measurable lesions; clear worsening from previous assessment of any evaluable disease; reappearance of any lesion that had disappeared; or appearance of any new lesion or site. (4) Stable disease (SD): the disease status for which both the measurable lesions were less than the criterion to meet PR, but also not sufficient to meet the criterion for PD.
Quality assessment
We evaluated the methodological quality of the included studies according to the Newcastle-Ottawa Scale (NOS) criteria (Little et al., 2009). The NOS criteria assessed three aspects: (1) subject selection: 0–4 scores; (2) comparability of subject: 0–2 scores; (3) clinical outcome: 0–3 scores. NOS score ranged from 0 to 9; and score ≥7 indicate a good quality.
Statistical analysis
We performed the meta-analysis using the STATA version 12.0 (STATA Corporation, College Station, TX) software. Crude standardized mean difference (SMD) and their 95% confidence intervals (CI) were estimated under a fixed or random effect model. The Z test was used to estimate the statistical significance of odds ratios. The Cochran's Q-statistic and I 2 test were used to evaluate potential heterogeneity between studies (Peters et al., 2006). If Q-test shows a p<0.05 or I 2 test exhibits >50%, which indicates significant heterogeneity, the random effects model was conducted; otherwise, the fixed effects model was used. Begger's funnel plots and Egger's linear regression test were conducted to investigate publication bias (Zintzaras and Ioannidis, 2005).
Results
Baseline characteristics of included studies
A total of 192 articles relevant to the searched keywords were initially identified. The titles and abstracts of all articles were reviewed and 133 were excluded; full texts and data integrity were then reviewed and another 45 articles were excluded. Finally, 14 clinical studies met our inclusion criteria for this meta-analysis, including 5 case–control studies and 9 cohort studies (Guo et al., 2002; Arinaga et al., 2003; Brattstrom et al., 2004; Iwasaki et al., 2004; Deng et al., 2005; Maekawa et al., 2007; Wang et al., 2008, 2012; Zhang et al., 2008, 2010; Huang, 2010; Ma et al., 2010; Meng et al., 2010; Zhao et al., 2010; Gu et al., 2011, 2013; Yang et al., 2011; Di et al., 2012). Publication years of the eligible studies ranged from 2002 to 2013. The selection process of eligible studies was shown in Figure 1. A total of 1747 subjects were involved in this meta-analysis, including 1602 NSCLC patients and 145 healthy controls. Peripheral blood samples were used in detecting serum VEGF. NOS scores of all included studies were ≥6. We summarized the study characteristics and methodological quality in Tables 1 and 2.

Flowchart shows study selection procedure. Fourteen clinical studies were included in this meta-analysis.
M, male; F, female; ELISA, enzyme-linked immunosorbent assay; NOS, Newcastle-Ottawa Scale.
RT, radiotherapy; HT, hyperthennia therapy; CT, chemotherapy; NR, not reported.
Quantitative data synthesis
Four studies referred to the difference in serum VEGF levels between NSCLC patients and healthy controls. The random effects model was conducted due to the potential existence of significant heterogeneity between studies (I 2=85.9%, p<0.001). Our meta-analysis results revealed that NSCLC patients had higher levels of serum VEGF than that of healthy controls (SMD=2.48, 95% CI=1.43 to 3.53, p<0.001) (Fig. 2). Subgroup analysis by NOS score also suggested that serum VEGF level of NSCLC patients was higher than that of healthy controls (NOS=6: SMD=1.66, 95% CI=0.63 to 2.69, p=0.002; NOS=7: SMD=2.74, 95% CI=1.42 to 4.05, p<0.001; respectively).
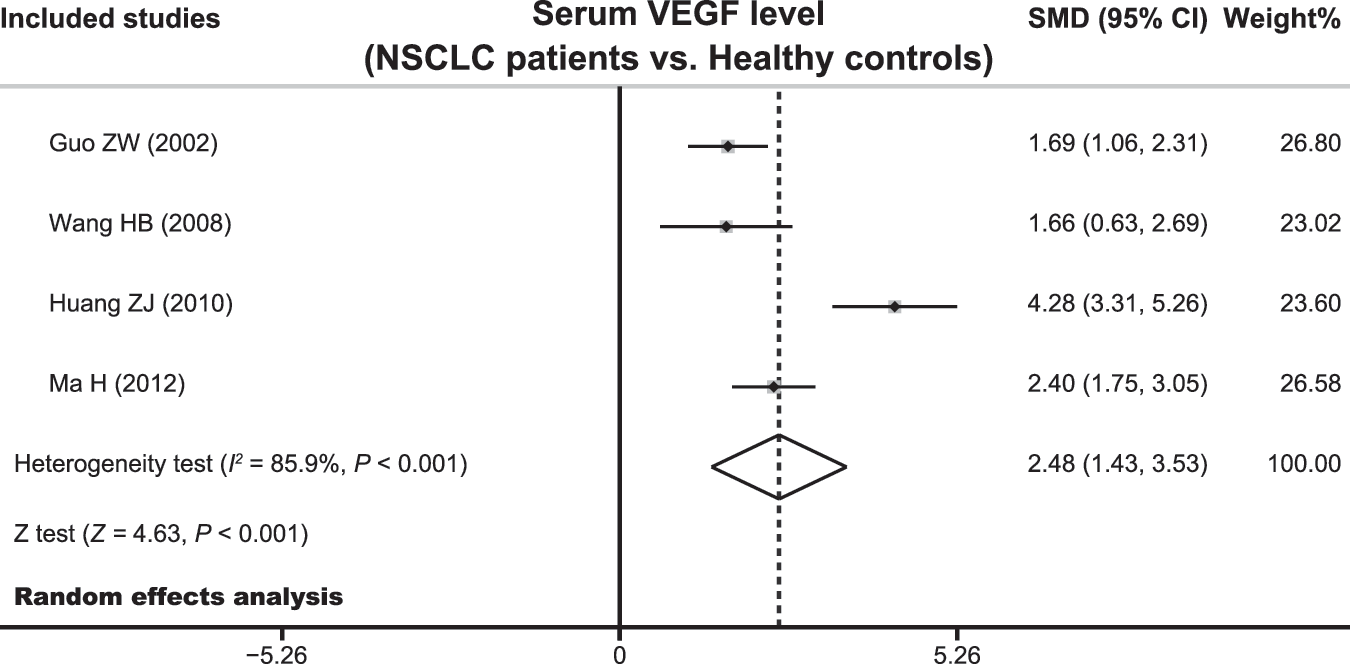
Forest plot for the difference in serum vascular endothelial growth factor (VEGF) levels between nonsmall cell lung cancer (NSCLC) patients and healthy controls.
Five studies involved the difference in serum VEGF levels between pre- and postradiotherapy care of NSCLC patients. The heterogeneity obviously existed (I 2=90.9%, p=0.001), so the random effects model was conducted to pool the results. There was significant differences in serum VEGF levels between before and after radiotherapy of NSCLC patients (SMD=−1.21, 95% CI=−2.06 to −0.36, p<0.001) (Fig. 3). In the subgroup analysis based on NOS score, the results showed that serum VEGF level of NSCLC patients after radiotherapy was lower than those before radiotherapy in the high-quality (NOS=7) subgroup (SMD=−1.68, 95% CI=−2.51 to −0.85, p<0.001), but not in the low-quality (NOS=6) subgroup (SMD=−0.41, 95% CI=−1.43 to 0.60, p=0.428).

Forest plot for the difference in serum VEGF levels between before and after radiotherapy of NSCLC patients.
The difference in serum VEGF levels between the effective (CR+PR) and noneffective (SD+PD) groups were investigated in four studies. Since obvious heterogeneity was observed, the random effects model was used (all p<0.05). We found significant differences in serum VEGF levels between effective and noneffective clinical response groups pre- and postradiotherapy (before radiotherapy: SMD=−0.78, 95% CI=−1.39 to −0.16, p=0.013; after radiotherapy: SMD=−3.62, 95% CI=−5.93 to −1.32, p=0.002; respectively) (Fig. 4). Stratified analysis based on NOS score also revealed significant differences in serum VEGF levels between effective and noneffective clinical response groups pre- and postradiotherapy (all p<0.05).

Forest plot for the difference in serum VEGF levels between the effective (complete response [CR]+partial response [PR]) and noneffective (stable disease [SD]+progressive disease [PD]) groups.
Five of 14 studies focused on the associations between serum VEGF levels and tumor–node–metastasis (TNM) stage and histologic grade of NSCLC patients. Significant heterogeneity was identified; so, the random effects model was used (all p<0.05). Nevertheless, serum VEGF levels showed no significant associations with TNM stage and histologic grade of NSCLC patients (TNM stage: SMD=1.63, 95% CI=0.52 to 5.09, p=0.401; histologic grade: SMD=0.40, 95% CI=0.09 to 1.88, p=0.248; respectively) (Fig. 5). We also conducted a subgroup analysis based on NOS score. However, no positive associations of serum VEGF level with TNM stage and histologic grade of NSCLC patients were observed (all p<0.05).

Forest plots for the associations of serum VEGF levels with tumor–node–metastasis (TNM) stage and histologic grade of NSCLC patients.
Only three studies reported the relationship between serum VEGF levels and OS of NSCLC patients. No heterogeneity was found; therefore, the fixed effects model was conducted. NSCLC patients with positive VEGF expression had shorter OS than those with negative VEGF expression (hazard ratio=1.55, 95% CI=1.05 to 2.04, p<0.001) (Fig. 6). In the subgroup analysis by NOS score, we observed positive correlations between positive VEGF expression and poor OS of NSCLC patients in both high-quality (NOS=7) and low-quality (NOS=6) subgroups (all p<0.05).

Forest plots for the relationship between serum VEGF levels and overall survival of NSCLC patients.
We performed sensitivity analyses to evaluate the influence of single studies on the overall estimate. The results indicated that the overall pooled estimates could not be affected by single study (Fig. 7). Begger's funnel plot and Egger's linear regression test were used to assess potential publication bias of included studies. We found no evidence of obvious asymmetry in the Begger's funnel plots (Fig. 8). Egger's test also did not display any strong statistical evidence for publication bias (all p>0.05).

Sensitivity analysis of the summary odds ratio coefficients on the relationships of serum VEGF levels with radiosensitivity in patients with NSCLC.
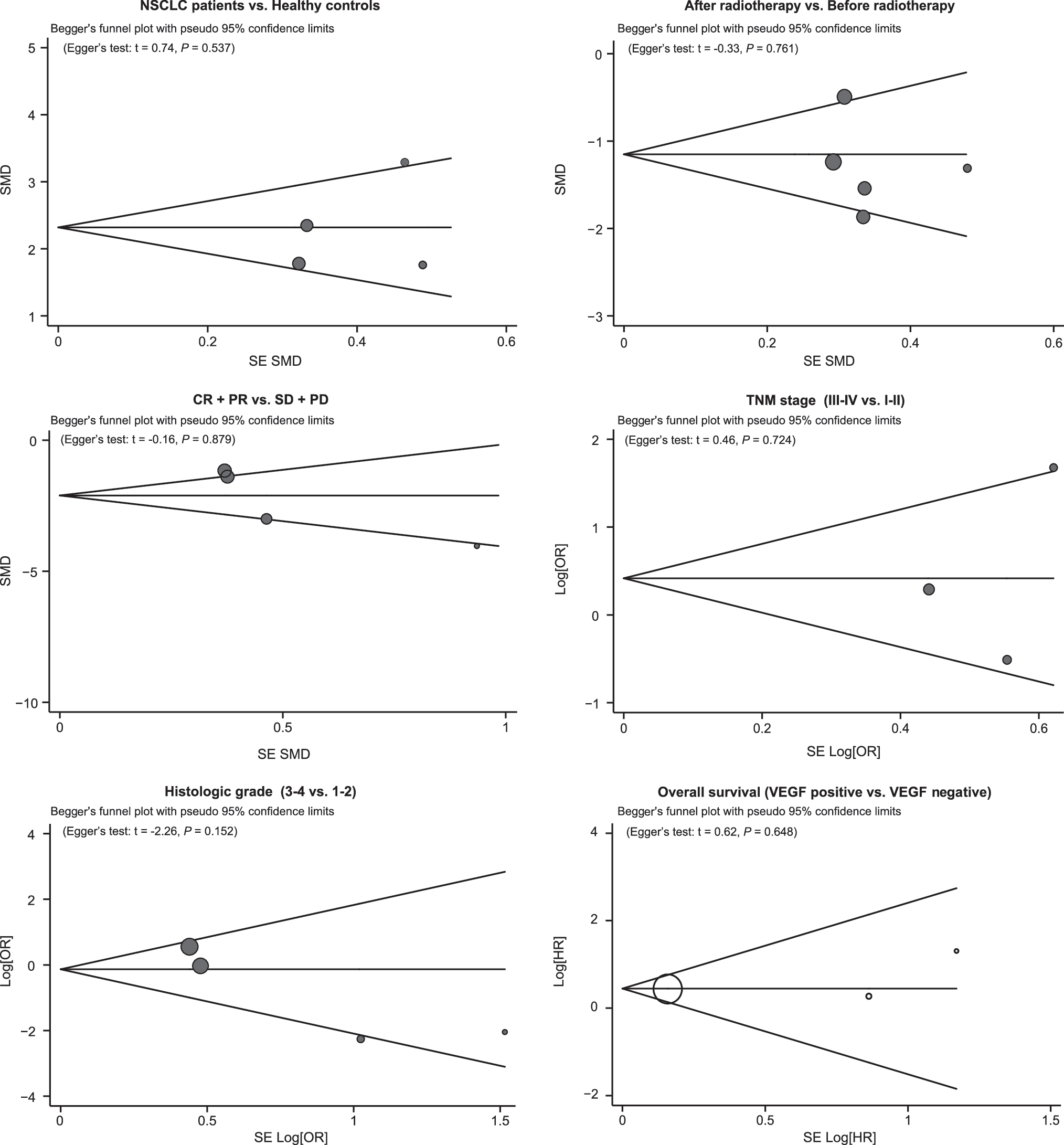
Begger's funnel plots of the relationships between serum VEGF level and radiosensitivity of NSCLC patients.
Discussion
VEGF, a subfamily of growth factors, plays a crucial role in the stimulation, proliferation, and migration of endothelial cells and increases the permeability of vessel walls. It can induce the development of neovascularization through a paracrine mechanism in both physiological and pathological processes, such as developmental and reproductive angiogenesis and proliferative retinopathies (Choi et al., 2013; Faur et al., 2013). In addition, it has been reported that a number of solid tumor cells in experimental and human models produce larger amounts of VEGF and express higher levels of VEGF mRNA, suggesting that VEGF expression may be strongly linked to angiogenesis in tumor development and progression, including gastric, colonic, and lung carcinomas (Hicklin and Ellis, 2005; He et al., 2013; Wang et al., 2013). Several clinical studies have confirmed that VEGF status is predictive of resistance to various treatments, which include radiotherapy, chemotherapy, and endocrine therapy, and that inhibitors to anti-VEGF therapies are effective in reducing tumor size, metastasis, and blood vessel formation (Toi et al., 2001; Takahashi, 2011). Moreover, VEGFR1 antagonists and a tyrosine kinase inhibitor of VEGFR2 reverted radiation-refractory tumor models to radiation-sensitive phenotype, which suggests that the high VEGF expression may define a radio-resistant phenotype (Geng et al., 2001; Veeravagu et al., 2007). Consequently, accumulating amounts of evidence have indicated that the degree of VEGF expression in the tumor tissue was a significant predictor of relapse-free survival and OS in patients with node-negative breast cancer with locoregional radiotherapy treatments (Linderholm et al., 1999). Similarly, other studies have suggested that expression of VEGF determined by immunohistochemical analysis is a highly significant and independent indicator of survival in patients treated with radiotherapy for advanced carcinoma of the cervix (Loncaster et al., 2000; Braicu et al., 2013). Recently, a growing number of studies have shown that VEGF is significantly expressed in NSCLC tissues, and positively correlated with sentinel lymph node metastasis, lymphangiogenesis density, and clinical staging (Hirakawa et al., 2007; Kawai et al., 2008). NSCLC accounts for 80% of the total lung carcinomas, and it has shown poor sensitivity to conventional radiotherapy and chemotherapy treatments (Kim et al., 2013). Naumnik et al. (2009) observed increase in serum VEGF level in patients with NSCLC that decreased after radiotherapy, and they pointed out that serum VEGF level could be used as a complementary diagnostic value of reference. Therefore, it is plausible that the combination of radiotherapy and inhibition of VEGF as therapeutic target could improve the radiosensitivity of the tumor (Ausborn et al., 2012). Further, abundant studies have documented that NSCLC patients with low serum VEGF levels have high radiosensitivity and VEGF expression was negatively correlated with radiosensitivity, revealing that serum VEGF level is strongly associated with tumor burden, tumor metastasis, and therapeutic effectiveness in patients with NSCLC (Takahashi, 2011; Yin et al., 2012). While other studies found no convincing evidence that serum VEGF levels lead to decreasing sensitivity to radiotherapy in patients with NSCLC (Sano et al., 2011; Topkan et al., 2013). This controversy could be explained with several reasons, such as the differences in study designs, sample size, source of controls, and so on. This meta-analysis aims to provide a more comprehensive and reliable conclusion on the associations between serum VEGF levels and sensitivity to radiotherapy for patients with NSCLC.
In this present meta-analysis, we evaluated the relationships between serum VEGF level and radiosensitivity in NSCLC patients. Finally, 14 clinical studies were included with a total of 1602 NSCLC patients and 145 healthy controls. Our meta-analysis results showed that serum VEGF level in NSCLC patients was significantly higher than that in healthy controls, suggesting that high serum VEGF level may play an important role in the progression and development of NSCLC. High expression level of VEGF is responsible for the formation of neovascularization and allows the tumor cells to infiltrate into the lymphatic vessels, which may aggravate the progress of NSCLC (Thangarajah et al., 2009). In addition, there was an obvious decrease in serum VEGF levels after radiotherapy. A reasonable explanation for this decrease in serum VEGF levels may be that radiotherapy can cause degeneration and necrosis of tumor cells, which leads to reduction in secretion of serum VEGF. Bremnes et al. (2006) confirmed that serum VEGF levels in NSCLC patients was significantly evaluated compared with that in the healthy controls, indicating that VEGF could be an important angiogenic factor in primary NSCLC. Further, our results showed that serum VEGF levels in patients of the effective group (CR+PR) was significantly lower than those in the noneffective group (SD+PD), revealing that serum VEGF may be strongly associated with efficacy and outcome of radiotherapy in NSCLC patients. Further analysis revealed that NSCLC patients with positive VEGF expression had a poorer OS than those with negative VEGF expression, suggesting that serum VEGF level may strongly correlate with the prognosis in NSCLC patients receiving radiotherapy. Although the exact function of VEGF in NSCLC is not fully understood yet, a potential explanation might be that VEGF functions as a primary driving force for physiological and pathological angiogenesis, and having positive serum VEGF levels leading to neoangiogenesis representing an important prognostic indicator of poor prognosis in NSCLC through a paracrine mechanism, thus affecting the prognosis of NSCLC patients. These results were consistent with previous studies and suggested that high levels of serum VEGF might be significantly linked to poor prognosis in NSCLC patients treated with radiotherapy (Salgia, 2011; Tischler et al., 2011; Zhang et al., 2012b). Our findings have provided a compelling biological rationale in using serum VEGF as a useful tool for early diagnosis and prognosis of patients with NSCLC receiving radiotherapy.
The current meta-analysis also had several limitations that should be pointed out. First, our results had lacked sufficient statistical power to assess the relationships of serum VEGF levels with radiosensitivity in NSCLC patients due to the small number of studies. Since some of the studies were small and even had standard deviations, our meta-analysis might induce fairly wide CIs, which restrain our confidence in drawing conclusions. Another important limitation of our meta-analysis is that our findings may be confined by source of control. In this meta-analysis, we only investigated the correlations between serum VEGF levels and radiosensitivity in NSCLC patients in Asian populations. It is widely accepted that there exist significant difference in genotypes among different ethnicity due to various environmental conditions and natural selection, which may have an impact on the reliability of our results and constrain the general applicability of our findings. Consequently, the cognitive function of our meta-analysis should be regarded preliminary. Third, our meta-analysis failed to obtain original data from the included studies, which may limit further evaluation of potential role of VEGF in the development and progression of NSCLC. Although our study has several limitations, this is the first meta-analysis focusing on the association of serum VEGF levels with radiosensitivity in NSCLC patients. Further, we performed a highly sensitive literature search strategy for electronic databases. A manual search of the reference lists from the relevant articles was also conducted to find other potential articles. The selection process of eligible articles was based on strict inclusion and exclusion criteria. Importantly, rigorous statistical analysis provided a basis for pooling of information from individual studies.
In conclusion, our meta-analysis suggests that serum VEGF level may be a useful biomarker for predicting radiosensitivity and prognosis of NSCLC patients among Asians. Thus, detection of serum VEGF may be a useful tool for early diagnosis and prognosis of NSCLC receiving radiotherapy. However, due to the limitations mentioned above, further detailed studies are still required to confirm our findings.
Footnotes
Acknowledgments
We would like to acknowledge the reviewers for their helpful comments on this article. We would also like to thank our colleagues at the Department of Oncology, The First Hospital of Qinhuangdao.
Disclosure Statement
No competing financial interests exist.