
Abstract
This meta-analysis was performed to evaluate the role of CDH1 promoter methylation in colorectal carcinogenesis. The PubMed, CISCOM, CINAHL, Web of Science, Google Scholar, EBSCO, Cochrane Library, and CBM databases were searched for relevant articles published before November 1st, 2013 without any language restrictions. Meta-analysis was conducted using the STATA 12.0 software. Crude odds ratios (ORs) with 95% confidence intervals (95% CIs) were calculated. Nine clinical cohort studies met all our inclusion criteria and were included in this meta-analysis. A total of 883 colorectal cancer (CRC) patients were assessed. Our meta-analysis results revealed that the frequencies of CDH1 promoter methylation in CRC tissues were higher than those in control tissues (OR=2.61, 95% CI=1.24–5.50, p=0.012). A subgroup analysis by ethnicity showed that CDH1 promoter methylation was closely linked to the pathogenesis of CRC among Asians and Africans (Asians: OR=2.90, 95% CI=1.26–6.67, p=0.012; Africans: OR=3.81, 95% CI=1.56–9.34, p=0.003; respectively), but not among Caucasians (OR=1.68, 95% CI=0.24–11.72, p=0.598). A further subgroup analysis by type of control tissues suggested that CRC tissues also exhibited higher frequencies of CDH1 promoter methylation than those of normal and adjacent tissues (normal: OR=1.57, 95% CI=1.12–2.21, p=0.009; adjacent: OR=5.07, 95% CI=2.91–8.82, p<0.001; respectively). However, we found no evidence for any significant difference in the frequencies of CDH1 promoter methylation between CRC tissues and adenomas tissues (OR=1.18, 95% CI=0.74–1.90, p=0.485). Our findings provide empirical evidence that CDH1 promoter methylation may play an important role in colorectal carcinogenesis. Thus, CDH1 promoter methylation may be a useful biomarker for the early diagnosis of CRC.
Introduction
C
E-cadherin, encoded by the CDH1 gene, belongs to the cadherin family, which plays a crucial role in establishing and maintaining intercellular connections (Li et al., 2012). The human CDH1 gene is located on chromosome 16q22.1 and consists of 16 exons, spanning ∼100 kb (Christofori and Semb, 1999). Previous studies have shown that abnormalities in the CDH1 gene are significantly associated with colorectal carcinogenesis (Grunhage et al., 2008; Xiong et al., 2012). E-cadherin is considered to be an inhibitor of invasion in numerous tumor cells, while methylation of the CDH1 gene may lead to downregulation or deletion of E-cadherin expression, weaken adhesion junction-mediated contacts among cells, and induce invasion and dissemination of CRC cells (Schmalhofer et al., 2009; Schrader et al., 2011; Stoops et al., 2011). Hence, aberrant CDH1 gene promoter methylation was speculated to be strongly correlated with colorectal carcinogenesis (Desotelle et al., 2013). Several previous studies have suggested that CDH1 promoter methylation might be a reliable predictor for the development and progression of CRC (Darwanto et al., 2003; Huang et al., 2005; Wang et al., 2012). However, some contradictory conclusions have also been published on the relationship between CDH1 promoter methylation and the risk of CRC (Lin et al., 2004; Garrity-Park et al., 2010; Kang et al., 2012). Therefore, we performed the present meta-analysis to more precisely evaluate the role of CDH1 promoter methylation in colorectal carcinogenesis.
Materials and Methods
Literature search
The PubMed, CISCOM, CINAHL, Web of Science, Google Scholar, EBSCO, Cochrane Library, and CBM databases were searched for relevant articles published before November 1st, 2013 without any language restrictions. The following keywords and MeSH terms were used: [“methylation” or “DNA methylation” or “de-methylation” or “hypermethylation”] and [“colorectal cancer” or “CRC” or “colorectal neoplasm” or “colorectal tumor” or “colorectal carcinoma” or “colorectal carcinogenesis”] and [“CDH1”or “E-cadherin” or “epithelial cadherin” or “cadherin-1” or “uvomorulin”]. We also performed a manual search to find other potential articles.
Selection criteria
The included studies had to meet all the following criteria: (1) the study must be a clinical cohort study; (2) the study must relate to the role of CDH1 promoter methylation in colorectal carcinogenesis; (3) all patients diagnosed with CRC must be confirmed through histopathologic examinations; and (4) the study must provide sufficient information about the frequencies of CDH1 promoter methylation. If a study did not meet the inclusion criteria, it was excluded. The most recent or the largest sample size publication was included when the authors published several studies using the same subjects.
Data extraction
Relevant data were systematically extracted from all included studies by two researchers using a standardized form. The researchers collected the following data: language of publication, publication year of article, the first author's surname, geographical location, design of study, sample size, the source of the subjects, methylation frequencies, source of samples, detection method of methylation, etc.
Quality assessment
Methodological quality was independently assessed by two researchers according to the Newcastle–Ottawa scale (NOS) criteria (Stang, 2010). The NOS criteria is scored based on three aspects: (1) subject selection: 0–4; (2) comparability of subject: 0–2; (3) clinical outcome: 0–3. NOS scores range from 0 to 9 with scores ≥7 indicating high quality.
Statistical analysis
The STATA version 12.0 (Stata Corp, College Station, TX) software was used for this meta-analysis. We calculated crude odds ratios (ORs) with their 95% confidence intervals (95% CIs) to evaluate relationships. The Z-test was used to estimate the statistical significance of the pooled statistics. The Cochran's Q-statistic and I 2 test were used to evaluate potential heterogeneity between studies (Zintzaras and Ioannidis, 2005). If the Q-test showed a p<0.05 or I 2 test exhibited a result >50%, indicating significant heterogeneity, the random-effects model was conducted; otherwise, the fixed-effects model was used. We also performed subgroup and meta-regression analyses to investigate potential sources of heterogeneity. To evaluate the influence of single studies on the overall estimate, a sensitivity analysis was performed. We conducted Begger's funnel plots and Egger's linear regression test to investigate publication bias (Peters et al., 2006).
Results
Characteristics of included studies
Initially, the searched keywords identified 260 articles. We reviewed the titles and abstracts of all articles and excluded 129 articles. Full texts and data integrity were then reviewed and another 122 articles were excluded. Finally, nine clinical cohort studies were included in this meta-analysis (Toyooka et al., 2002; Darwanto et al., 2003; Lee et al., 2004; Lin et al., 2004; Huang et al., 2005; Garrity-Park et al., 2010; Miladi-Abdennadher et al., 2010; Kang et al., 2012; Wang et al., 2012). The publication years of eligible studies range from 2002 to 2012. Figure 1 shows the selection process of eligible articles. Distribution of the number of topic-related literature in electronic databases over the last decade is shown in Figure 2. A total of 883 CRC patients were assessed. Overall, six studies were conducted among Asians, two studies among Caucasians, and only one study among Africans. Tissue samples were used for detection of CDH1 promoter methylation; and the classical methylation-specific polymerase chain reaction was performed in all included studies. The NOS scores of all included studies were ≥5. We summarized the study characteristics and methodological quality in Table 1.
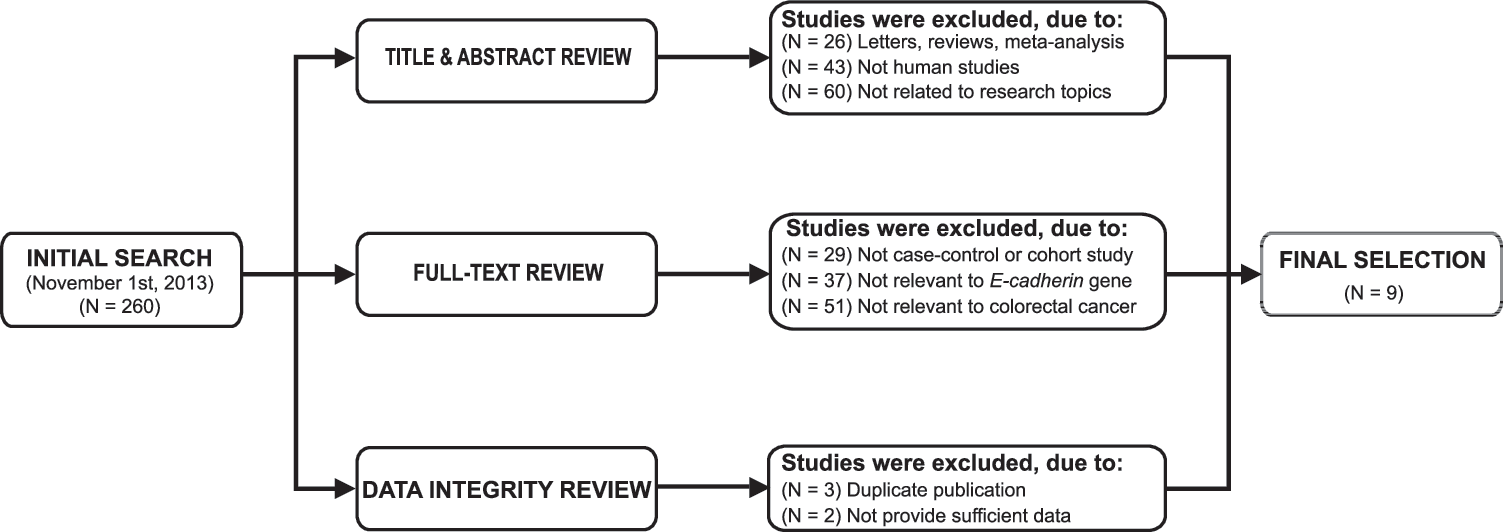
Flowchart of literature search and study selection. Nine cohort studies were included in this meta-analysis.
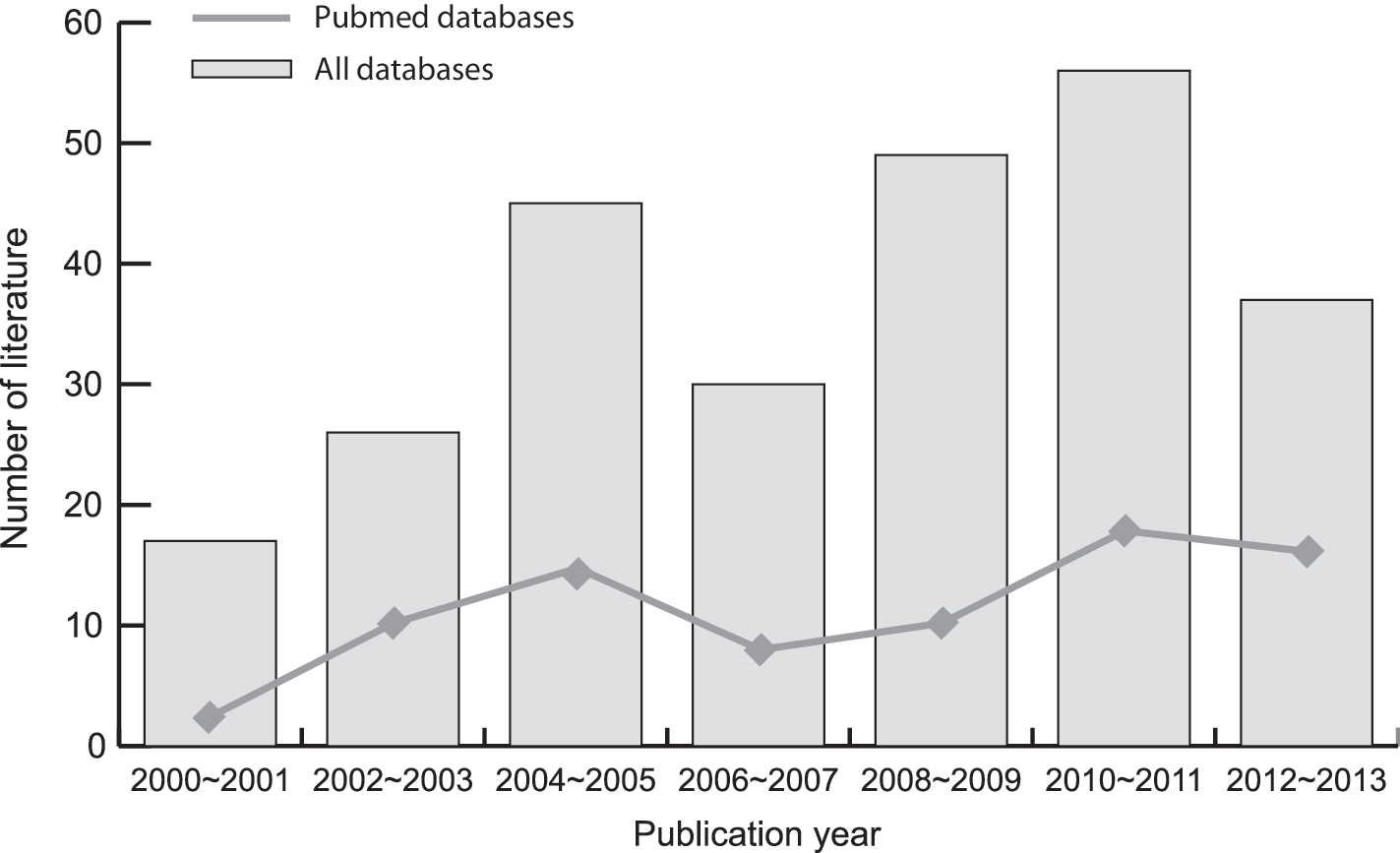
Distribution of the number of topic-related literature in electronic databases over the last decade.
MSP, methylation-specific polymerase chain reaction; NOS, Newcastle–Ottawa scale.
Quantitative data synthesis
The random-effects model was conducted due to the existence of significant heterogeneity between studies (I 2=82.3%, p<0.001). Our meta-analysis results revealed that the frequencies of CDH1 promoter methylation in the CRC tissues were higher than those in control tissues (OR=2.61, 95% CI=1.24–5.50, p=0.012) (Fig. 3). A subgroup analysis by ethnicity showed that CDH1 promoter methylation was closely linked to the pathogenesis of CRC among Asians and Africans (Asians: OR=2.90, 95% CI=1.26–6.67, p=0.012; Africans: OR=3.81, 95% CI=1.56–9.34, p=0.003; respectively), but not among Caucasians (OR=1.68, 95% CI=0.24–11.72, p=0.598) (Fig. 4A). Further subgroup analysis by type of control tissues suggested that CRC tissues also exhibited higher frequencies of CDH1 promoter methylation than those of normal and adjacent tissues (normal: OR=1.57, 95% CI=1.12–2.21, p=0.009; adjacent: OR=5.07, 95% CI=2.91–8.82, p<0.001; respectively) (Fig. 4B). However, we found no evidence for any significant difference in the frequencies of CDH1 promoter methylation between CRC tissues and adenomas tissues (OR=1.18, 95% CI=0.74–1.90, p=0.485).

Forest plots for the relationships between CDH1 promoter methylation and colorectal carcinogenesis under the random-effects model.
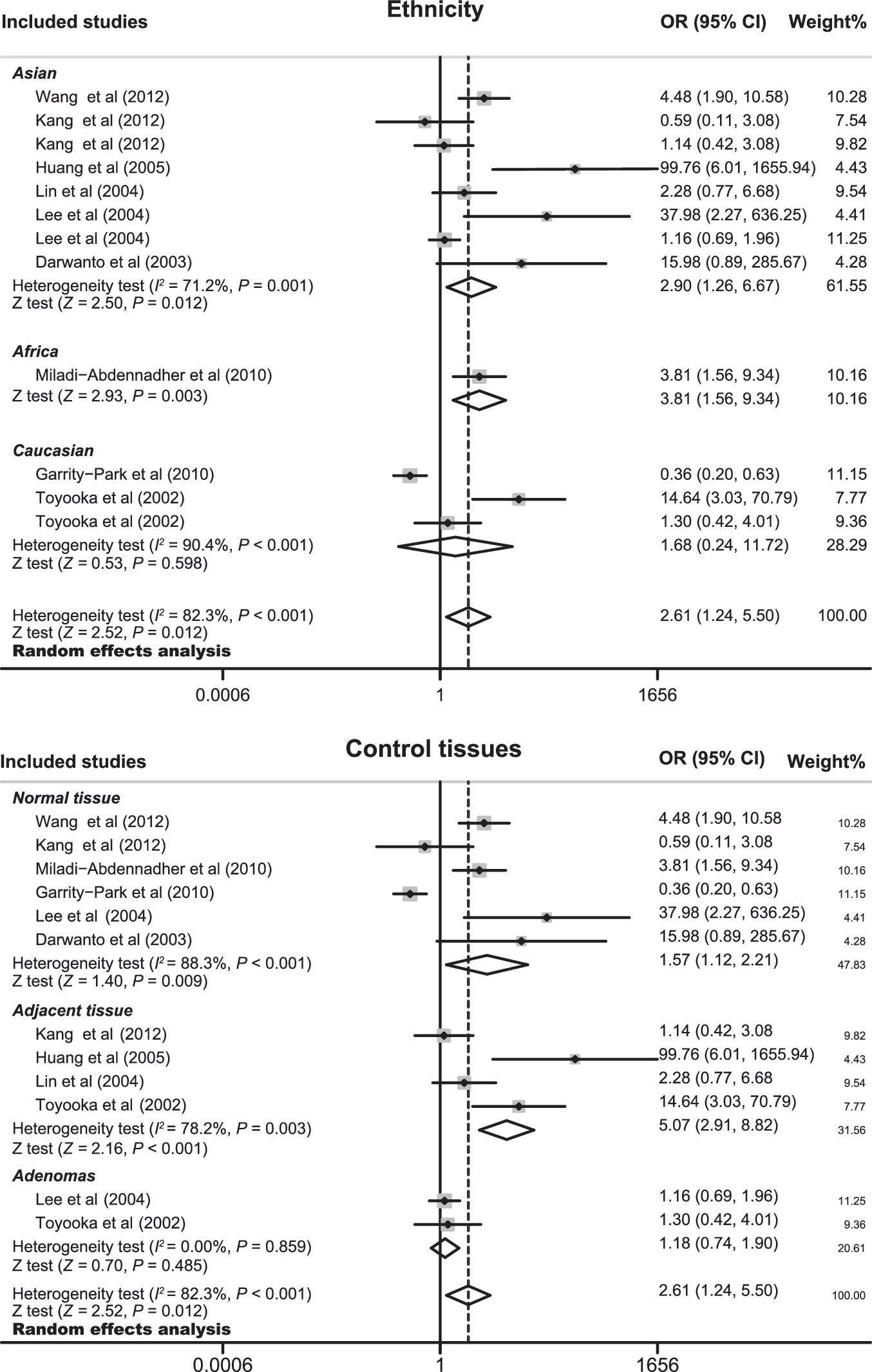
Subgroup analyses by ethnicity and type of control tissues of the relationships between CDH1 promoter methylation and colorectal carcinogenesis under the random-effects model.
Meta-regression analyses also confirmed that type of control tissues might be a main source of heterogeneity (p=0.046) (as shown in Table 2). The results of a sensitivity analysis suggested that no single study could influence the overall pooled estimates (Fig. 5). We found no evidence of obvious asymmetry in the Begger's funnel plots (Fig. 6). Egger's test also did not display strong statistical evidence for publication bias (t=−1.97, p=0.077).
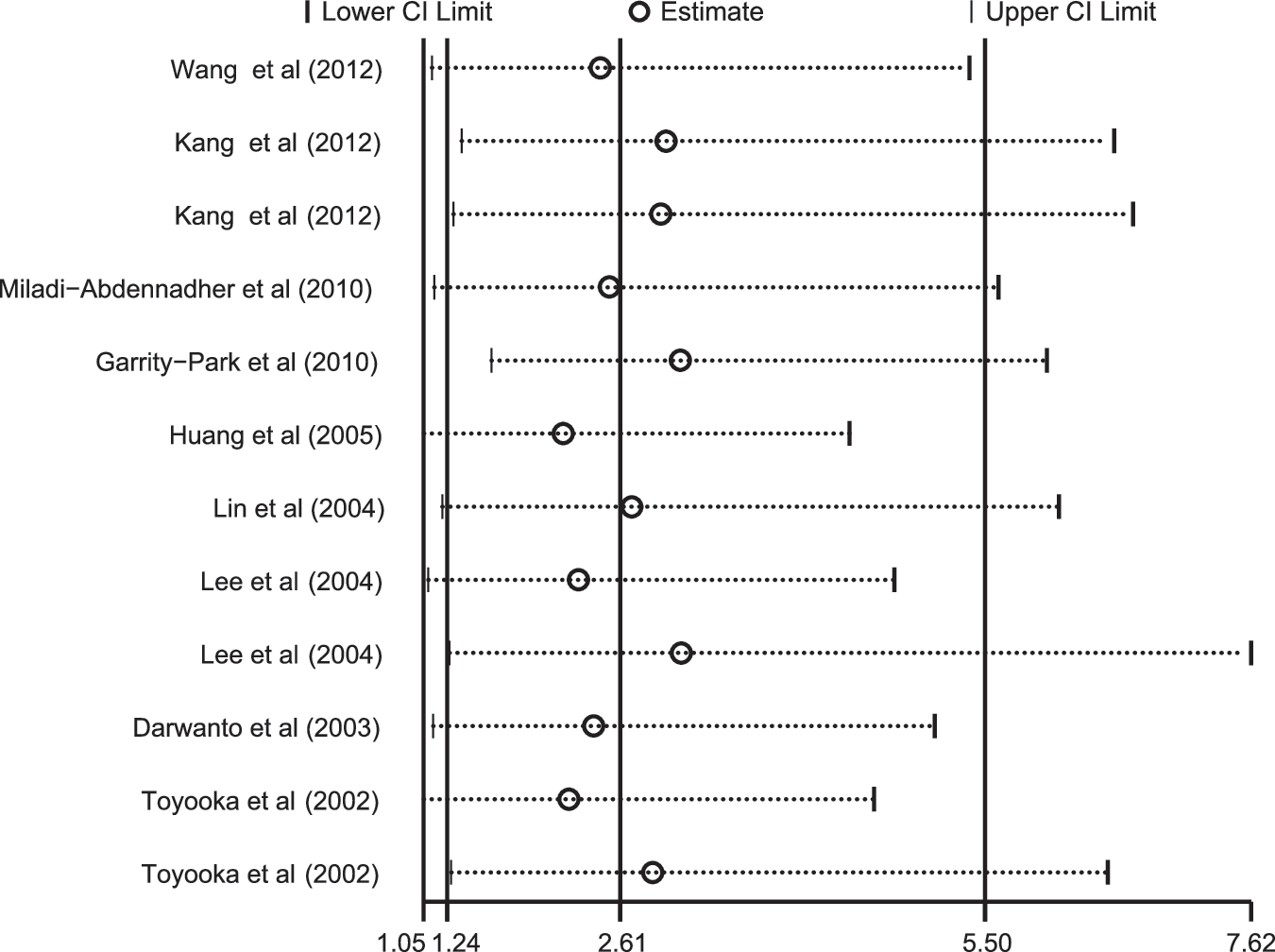
Sensitivity analysis of the summary of odds ratio coefficients on the relationships between CDH1 promoter methylation and colorectal carcinogenesis.
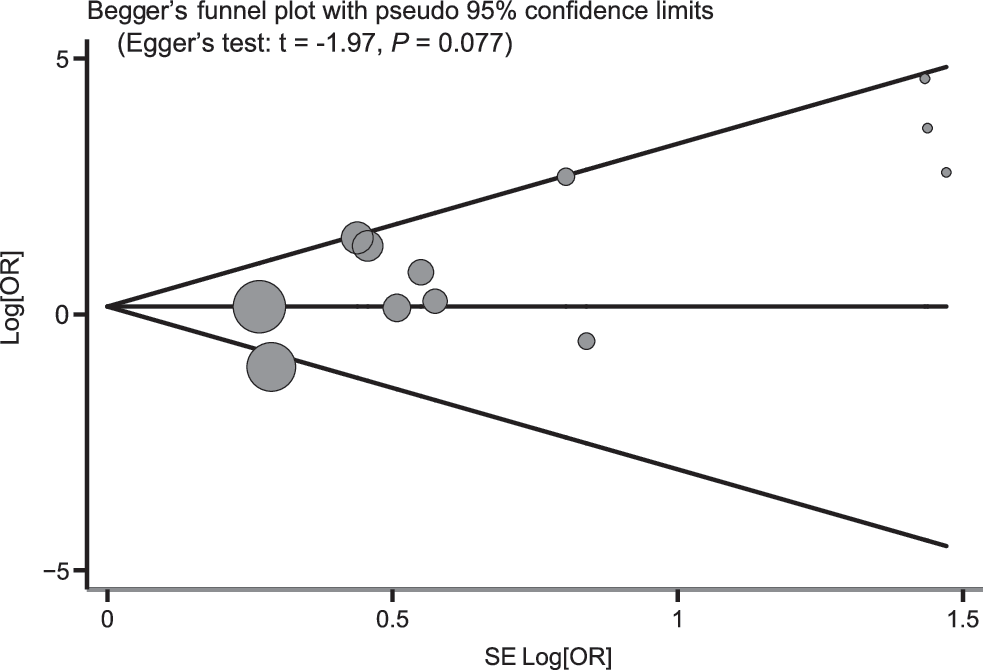
Begger's funnel plot of publication biases on the relationships between CDH1 promoter methylation and colorectal carcinogenesis.
SE, standard error; 95% CI, 95% confidence interval; UL, upper limit; LL, lower limit.
Discussion
E-cadherin, a member of the cadherin superfamily, is a Ca2+-dependent cell–cell adhesion molecule (Shirkoohi, 2013). Generally, E-cadherin is involved in a variety of biological processes such as selecting cell recognition and adhesion, maintaining tissue integrity in the epithelium, and regulating intra- and intercellular signaling pathways (Van den Bossche et al., 2012). A number of previous studies have demonstrated that E-cadherin may play an important role in the pathogenesis of CRC (Kim et al., 2010; Li et al., 2011). It is widely accepted that E-cadherin may be responsible for inhibiting tumor invasion and metastasis in epithelial cells (Baranwal and Alahari, 2009). However, aberrant methylation of the CDH1 gene may lead to the downregulated or absent expression of E-cadherin, which may be conducive to the invasion and metastasis of human cancers, including CRC (Elzagheid et al., 2012; Halvey et al., 2012). Therefore, it has been postulated that CDH1 promoter methylation may be strongly correlated with colorectal carcinogenesis (Garrity-Park et al., 2010). Additionally, it is worth noting that numerous studies have been conducted to investigate the potential associations between CDH1 promoter methylation and CRC, especially focusing on tissue samples, including CRC tissues, adenomas tissues, normal tissues, and adjacent tissues (Toyooka et al., 2002; Darwanto et al., 2003; Lee et al., 2004; Lin et al., 2004; Huang et al., 2005; Garrity-Park et al., 2010; Miladi-Abdennadher et al., 2010; Kang et al., 2012; Wang et al., 2012). E-cadherin is expressed in most human epithelial tissues (Behrens et al., 1991) and the key strength of the current research is that CRC tissues and normal human tissues are examined in epigenetic studies (Kang et al., 2012).
To evaluate the exact role of CDH1 promoter methylation in CRC carcinogenesis, we performed a meta-analysis of nine cohort studies with a total of 869 CRC patients. Our meta-analysis results indicated that the frequencies of CDH1 promoter methylation in the CRC tissues were higher than those in the control tissues, suggesting that CDH1 promoter methylation may be a causative factor for the incidence of CRC. Although the precise function of CDH1 promoter methylation in the development of CRC remains poorly understood, a possible explanation for this finding is that CDH1 methylation results in the downregulation of E-cadherin levels, leading to the loss of its function, which plays a significant role in neoplastic behavior by influencing the establishment of cell polarity and maintaining normal tissue morphology and cellular differentiation (Dorudi et al., 1995). Our results were consistent with a previous study's findings that CDH1 promoter methylation in CRC is associated with the reduction or absence of E-cadherin expression, which may induce loss of differentiation and increased invasiveness in CRC (Wheeler et al., 2001).
Since heterogeneity obviously existed, we performed stratified analyses based on ethnicity and type of control tissues. Our findings suggested that there were significant associations between CDH1 promoter methylation and colorectal carcinogenesis among Asians and Africans, but not among Caucasians, revealing that ethnic differences may have been the source of heterogeneity between studies concerning the role of CDH1 promoter methylation in the pathogenesis of CRC. This heterogeneity may be explained as the result of the impact of natural selection and random genetic drift on an individual's susceptibility to CRC. Further analysis by type of control tissues demonstrated that CRC tissues showed higher frequencies of CDH1 promoter methylation than did normal and adjacent tissues, but not higher than did adenomas tissues, implying that CDH1 gene methylation may also contribute to the development of benign colorectal tumors. A reasonable explanation for this finding may be that CDH1 gene promoter methylation may contribute to the reduction or elimination of the expression of E-cadherin, which is capable of suppressing invasion in numerous tumor cells (Stoops et al., 2011). In short, our findings were consistent with previous studies in finding that CDH1 promoter methylation may be closely linked to colorectal carcinogenesis and suggesting that CDH1 promoter methylation could be a useful biomarker for the early diagnosis of CRC.
As the first meta-analysis focused on the role of CDH1 promoter methylation in colorectal carcinogenesis, our study has some limitations. First, our results lacked sufficient statistical power to assess the exact roles of CDH1 promoter methylation in colorectal carcinogenesis due to the relatively small sample size of the included data. Second, since meta-analysis is a retrospective study, subject selection bias may have affected the reliability of our results. Third, our meta-analysis failed to obtain original data from the included studies, which may have limited our evaluation of the potential role of CDH1 promoter methylation in the development and progression of CRC. Importantly, the inclusion criteria of cases and controls were not well defined in all included studies and thus might have influenced our results.
In conclusion, our findings provide empirical evidence that CDH1 promoter methylation may play an important role in colorectal carcinogenesis. Thus, CDH1 promoter methylation could be a useful biomarker for the early diagnosis of CRC. However, due to the limitations mentioned above, further research conducted using larger sample sizes is needed to provide a more representative statistical analysis.
Footnotes
Acknowledgment
The authors would like to acknowledge the reviewers for their helpful comments on this article.
Disclosure Statement
The authors have declared that no competing interests exist.