
Abstract
Rare autosomal aneuploidies (RAAs) can cause miscarriage or other pregnancy complications and lead to inconsistent results of noninvasive prenatal testing (NIPT), but many NIPT providers have not yet started to provide related services. Our aim was to develop a semiconductor sequencing platform (SSP)-based method for detecting RAAs when pregnant women performed NIPT. Fifty-three aneuploidy samples with verified karyotyping or array comparative genomic hybridization (aCGH) results were collected and subjected to RAAs detection using an SSP to develop a method by genomic sequencing. Various trisomies on all chromosomes other than chromosomes 17 and 19, four multiple aneusomies, one monosomy and five sex chromosome abnormalities were got by our method which can directly identify RAAs via a z-score. Then, artificial mixtures of 10% and 5% DNA were created by adding fragmented fifty-three tissue samples and used in an NIPT simulation to develop a bioinformatics analysis method which can use in NIPT. And the results were in accordance with those of karyotyping and aCGH. Therefore, our method has potential for use in NIPT. Finally, 23,823 clinical plasma samples were tested to verify the performance of our approach. Karyotyping or aCGH was performed on the positive clinical samples. In total, 188 of 23,823 clinical samples were positive (T2, n = 1; T7, n = 1; T13, n = 15; T18, n = 45; T21, n = 125; and multiple aneusomies, n = 1) and verified by karyotyping or aCGH; no sample was a false negative. Several false positives were detected, one of which showed maternal copy number variation (CNV). One case of multiple aneusomies was caused by a maternal tumor. The method developed enables detection of RAAs without increasing costs.
Introduction
S
RAAs involve all autosomal chromosomes other than 21, 18, or 13 and are infrequently present at birth. While RAAs are rare, they are associated with an increased risk of miscarriage, stillbirth, and early neonatal death (Alberman and Creasy, 1977). Although they usually occur in early pregnancy, RAAs may also develop in pregnant women at 9–12 weeks of gestation, which is typically when NIPT is performed (Gregg et al., 2016; Pertile et al., 2017).
Several reports have emphasized the importance of detecting RAAs (Bayindir et al., 2015; Bianchi et al., 2015; Hartwig et al., 2017) for monitoring the health of the pregnancy and minimizing the frequency of false-positive and -negative NIPT results. In addition, aneuploidy is frequently noted in solid tumors (Kapranos et al., 2005); therefore, RAAs can be used to identify maternal tumors during pregnancy (Amant et al., 2015).
In this study, we developed a method to detect all fetal autosomal aneuploidies with a semiconductor sequencing platform (SSP) for use in NIPT. The method enables assessment of chromosomes 1–22 with no increase in cost.
Materials and Methods
Study design
This study was organized into three phases. Phase I involved the development and definition of a method for determining the aneuploidy state of chromosomes in 53 tissue samples previously validated by karyotyping or array comparative genomic hybridization (aCGH). Phase II involved the production of 10% and 5% artificial genomic DNA mixtures to assess the feasibility of the method for NIPT. In phase III, we verified the performance of the developed method in a prospective manner using 23,823 pregnant subjects. The positive results were verified by aCGH or karyotyping.
Samples and clinical materials
The study was performed according to the guidelines of the Clinical Research Ethics Committee of the Guangzhou DaRui Clinical Laboratory Center. Informed consent was obtained from patients before their participation in the study. From November 2013 to September 2017, a total of 53 tissue samples (T1, n = 1; T2, n = 2; T3, n = 2; T4, n = 2; T5, n = 1; T6, n = 2; T7, n = 2; T8, n = 2; T9, n = 1; T10, n = 2; T11, n = 1; T12, n = 1; T13, n = 1; T14, n = 2; T15, n = 1; T16, n = 5; T18, n = 4; T20, n = 1; T21, n = 1; T22, n = 4; 47, XXX, n = 1; 47, XXY, n = 1; 45, X, n = 3; monosomy 21, n = 1; mosaic, n = 5; and multiple aneusomies, n = 4), including trisomies of all autosomal chromosomes (excluding 17 and 19 and cases of other aneuploidies), 450 pregnant females without aneuploidy samples, 23,823 maternal blood samples of pregnant women, and 50 peripheral blood from nonpregnant healthy women aged 20–32 years, were collected. All tissue samples and 450 samples had been confirmed by karyotyping or aCGH, and the maternal age range was 20–45 years with a mean of 29 years. The gestational age range was 9–24 weeks, with a mean of 15 weeks.
DNA extraction
Genomic DNA was extracted from tissue samples using a QIAamp DNA Mini Kit (QIAamp DNA Blood Mini Kit; Qiagen GmbH, Hilden, Germany) following the manufacturer's instructions. Circulating free fetal DNA (cff DNA) was extracted using a commercial blood DNA kit (Nucleic Acid Isolation or Purification Reagent; DaRui, Guangzhou, China) following the manufacturer's instructions and stored at −80°C before use.
Artificial DNA mixtures
Genomic DNA was sheared using a Covaris M220 instrument (Covaris, Woburn, MA). DNA fragments (140–200 bp) were purified using beads (Agencourt AMPure XP; Beckman Coulter Genomics, Danvers, MA) and quantified using a Qubit® 2.0 (Life Technologies, Carlsbad, CA). Peripheral blood (50 mL) from nonpregnant healthy women aged 20–32 years was collected into EDTA tubes. Plasma was separated by centrifugation, and DNA was extracted using a commercial blood DNA kit (Nucleic Acid Isolation or Purification Reagent; DaRui) according to the manufacturer's instructions, quantified using a Qubit 2.0, and stored at −80°C before use.
Artificial DNA mixtures (5% [n = 53] and 10% [n = 53]) were prepared by adding the appropriate proportion of fragmented DNA to peripheral blood plasma from nonpregnant healthy women. Mixtures of fetal DNA fraction (5% and 10%) were also prepared.
DNA library construction and sequencing
Fragmented DNA samples and artificial DNA mixtures were subjected to library construction using an Ion Plus Fragment Library Kit according to a modified version of the Ion Xpress™ Plus gDNA Fragment Library Preparation User Guide (Life Technologies). Fifteen libraries were pooled and amplified by emulsion PCR using the Ion OneTouch™ 2 System (Life Technologies), which enables automated delivery of templated ion-sphere particles (ISPs). Template-positive ISPs were enriched with the Ion OneTouch™ ES (Life Technologies). The ISPs were loaded immediately onto the ion semiconductor chip, which was placed in the Ion Proton sequencer at 300 flows for sequencing according to the manufacturer's instructions.
Method development
Based on the protocol of a commercial kit (Trisomy Detection Kit; DaAn, Guangzhou, China), we improved several algorithms to enhance the accuracy of the results. We filtered out two types of bin which was different from conventional: those for which the sequencing depth was too high or too low (i.e., an up to threefold greater standard deviation [SD] of sequencing depth within the same chromosome), and those showing excessive variation in the depth of sequencing among multiple normal samples (i.e., a variation coefficient of >3). We also separated the data of male and female patients while filtering to increase the reliability of the results. We obtained an average of 5 million raw reads per sample; the mean rate of unique-mapping reads was 75% (3.5 MB). Following completion of data handling (computation and quality control metrics aligned to the human genomic reference sequence [hg19]), two-step correction—bin-offset correction and GC correction—was applied to remove variations among bins. Then, the sequences of each sample were binned according to the index and mapped to the unmasked hg19. The remaining unique aligned reads (with the exception of chromosome Y) were normalized to a constant 100 K and then allocated to 20 K equal-sized bins to generate read count statistics. The chromosome ratio in a test case of chromosome i was calculated using the following equation:
where i is the number of chromosomes, and Ni is the number of unique reads of chromosome i.
The z-score for each chromosome in a test sample was derived by subtracting the mean chromosome ratio in a reference set of euploid control pregnancies from the chromosome ratio in a test case and dividing by the SD of the chromosome ratio in the reference set according to the following equation:
where i is the number of chromosomes, Ratioi is the chromosome ratio in a test case of chromosome i, μi is the mean chromosome ratio in a reference set of chromosome i, and σi is the SD of the chromosome ratio in the reference set in chromosome i. The reference set was obtained from 450 pregnant females without aneuploidy samples from the NIPT platform of Guangzhou DaRui Clinical Laboratory Center.
aCGH and karyotyping
DNA (500 ng per sample) was labeled and hybridized to a SurePrint G3 Human CGH Microarray (98 × 60 K; Agilent Technologies, Palo Alto, CA) consisting of 60,000 oligonucleotides, and the whole genome was assayed at an effective backbone resolution of 200 kb. The slides were scanned using an Agilent SureScan Microarray scanner, and the images were analyzed using Agilent Genomic Workbench software.
Cells were cultured from amniocentesis samples and stained, and the chromosomes were viewed under a microscope.
Results
At present, aneuploidies are detected by calculating the z-score to quantify the deviation in the number of sequence reads at the chromosome level from the number expected in normal; that is, euploid, samples (Fan and Quake, 2010). In this study, we identified the aneuploidy status of all autosomal chromosomes by calculating z-scores using a normal range of −3 < z < 3 (Chiu et al., 2011).
Sequencing of genomic DNA by SSP
A total of 28 types of aneuploidy were detected by SSP in 53 miscarriage tissue samples (Fig. 1). Trisomies were detected in all autosomal chromosomes other than 17 and 19. Furthermore, three double aneusomies (D6017 [T12, monosomy 21], D8017 [T8, T21], and D7093 [T20, XXX]) and one multiple aneusomy (D6010 [T2, T7, T13, XXY]) were detected. Moreover, one monosomy (chr21) and five sex chromosome abnormalities (3 cases of 45, X, 1 case of trisomy XXX, and 1 case of 47, XXY) were identified. The results of SSP were in agreement with those of karyotyping and aCGH. The mean z-scores of aneuploid specimens were markedly higher than those of euploid samples (Fig. 2A).

Numbers of chromosomal aneuploidies in genomic DNA and artificial DNA mixtures. D8004 (mosaic trisomy 7), D8099 (mosaic trisomy 8), D6033 (mosaic trisomy 16), D6024 (mosaic trisomy 21), D8073 (mosaic trisomy 21), D6010 (T2, T7, T13, XXY), D6017 (T12, monosomy 21), D8017 (T8, T21), and D7093 (T20, XXX). Color images available online at

Mean z-scores of tissue samples
Simulation results
Fifty-three artificial 10% and 5% DNA mixtures were created to simulate NIPT and tested by our developed method. The SSP results were similar to those of 53 genomic DNA samples (Fig. 1) and were in accordance with the karyotyping and aCGH results; moreover, there was no false positive or negative. The mean z-scores of aneuploid specimens were markedly higher than those of euploid samples (Fig. 2B, C).
Clinical samples and validation
Of the 23,823 samples, 188 and 23,635 yielded positive and negative results, respectively. Two RAAs and one multiple aneusomy were detected. One case of trisomy 2, one case of trisomy 7, and one case of multiple aneusomies (trisomy 5, trisomy 13, trisomy 14, monosomy 15, trisomy 18, trisomy 20, and trisomy 21) were detected. In addition, several common chromosomal aneuploidies of trisomy 21 (n = 125), 18 (n = 45), and 13 (n = 15) were identified (Fig. 3).
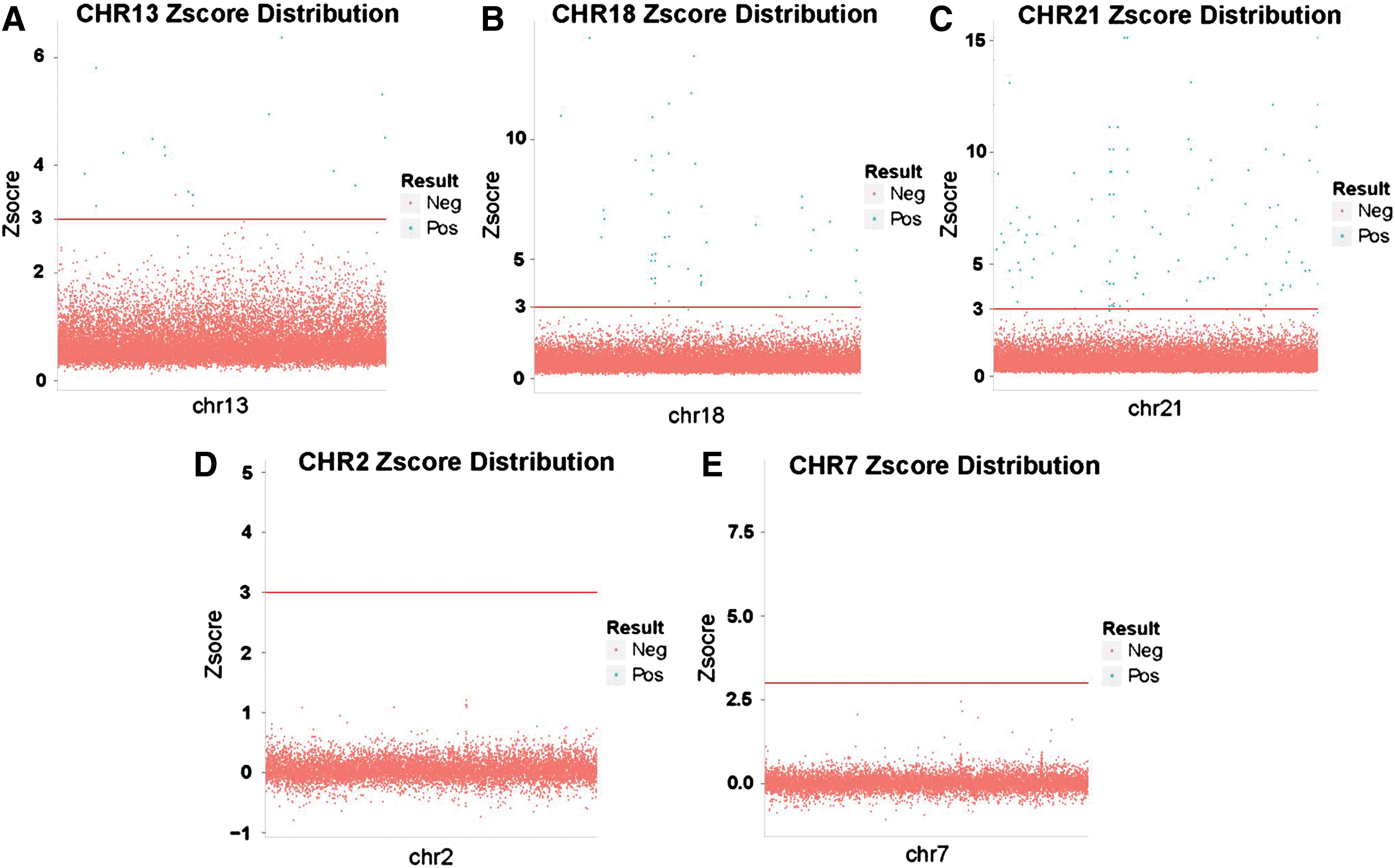
Z-scores of clinical samples (N = 23,823) and cutoffs for detection of fetal aneuploidy.
Two RAAs were detected by our method—one trisomy 2 and one trisomy 7. aCGH analysis of these two samples yielded similar results (Fig. 4). In addition, one sample showed multiple aneuploidies (trisomy 5, trisomy 13, trisomy 14, monosomy 15, trisomy 18, trisomy 20, and trisomy 21). Cases of multiple aneuploidies are relatively rare, so we made some validation plans. Karyotyping was performed on samples obtained by amniocentesis to verify the chromosome status of the fetus. The results revealed that this sample had normal diploid cells (Fig. 5A). Therefore, aCGH of the mother's genomic DNA was performed to identify any copy number variations (CNVs) that could lead to a positive NIPT result. The karyotype of the mother was normal; however, several microduplications were detected in chromosomes 2, 4, 8, 14, and 22; in contrast, the result of NIPT was positive only for chromosome 14 (Fig. 5B). A search of the Database of Genomic Variants database indicated that these are nonpathogenic repeats. A subsequent review of the woman's medical history showed that she suffered from uterine leiomyoma before becoming pregnant.

Analysis of chromosomal aneuploidy using a semiconductor sequencing platform
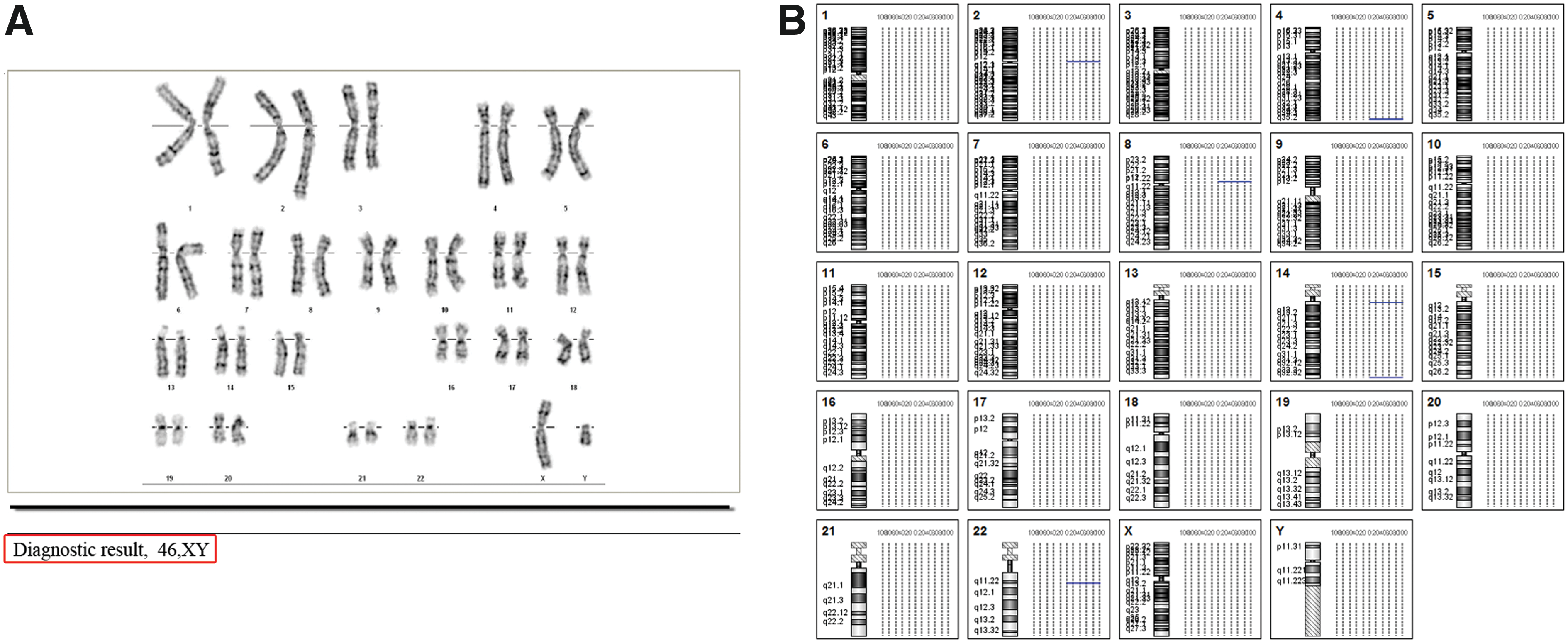
Validation of one case of multiple aneuploidies by karyotyping
The T13-, T18-, and T21-positive samples were confirmed by full karyotyping, which identified several false positives (Table 1). A causal analysis showed that among the false positives for T21, one had maternal CNV, which was a microduplication on 21q11.2–21q12.1 (10 MB) (Fig. 6).
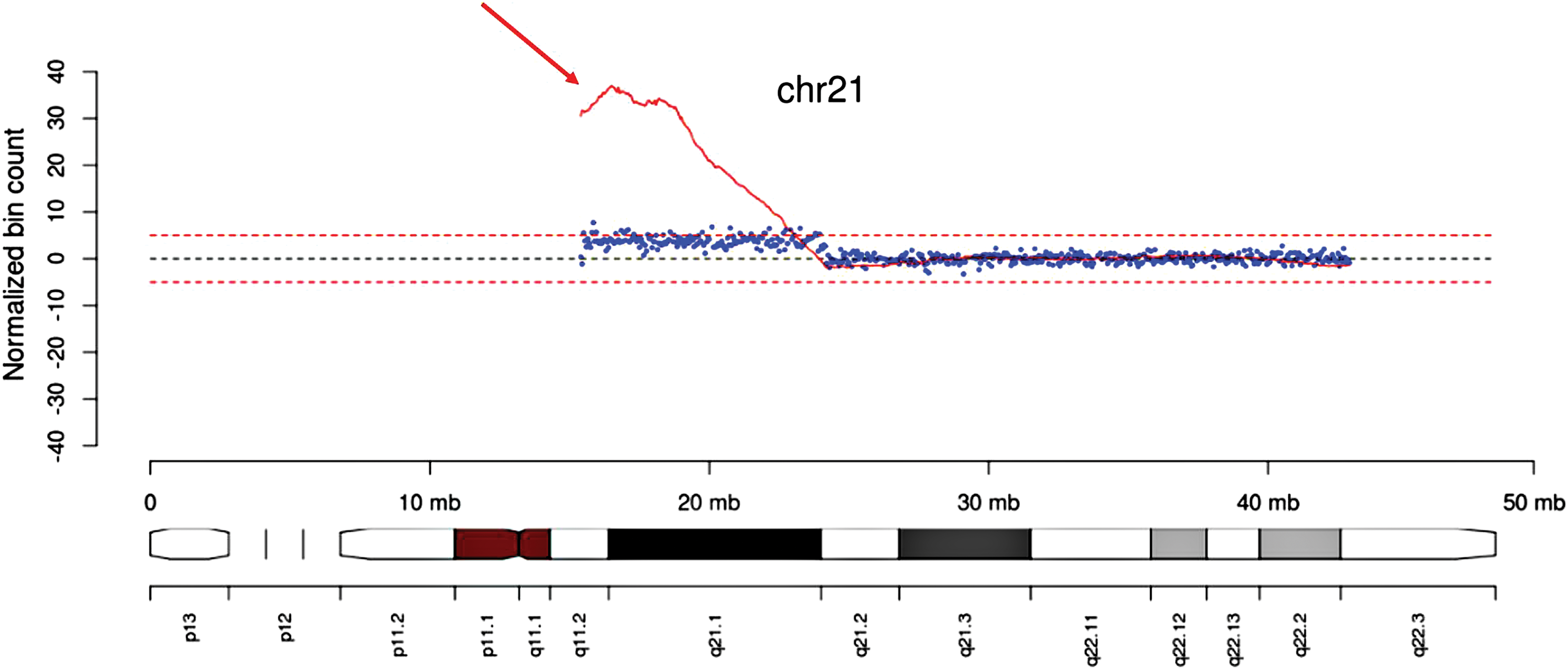
Validation of one false-positive T21 case. Red arrow indicates a microduplication on 21q11.2–21q12.1 (10 MB). Color images available online at
aCGH, array comparative genomic hybridization; N/A, not applicable; SSP, semiconductor sequencing platform.
Discussion
In this study, we developed a method to detect RAAs based on SSP, which relies on the existing detection method for T13, T18, and T21. The developed method overcomes the limitation of current NIPT as it enables detection of aneuploidies other than trisomies 21, 18, and 13 at no additional cost. Detection of RAAs can also provide information for monitoring the health of the fetus.
The developed method yielded a total of 28 types of aneuploidy and detected trisomies on all autosomal chromosomes other than 17 and 19. Multiple aneusomies and monosomies were also detected using this method, which enabled discrimination of normal from abnormal mosaicism, but not calculation of the percentage of mosaicism due to the small number of positive samples. The SSP results were generally in agreement with those of karyotyping and aCGH, and there were no false positives or -negatives. Therefore, our detection method enables differentiation of normal and abnormal samples.
We analyzed 23,823 maternal peripheral blood samples of pregnant women to evaluate the performance of our method; one case of trisomy 2 and one case of trisomy 7 were detected. The most common reason for early abortion is the existence of a major fetal chromosomal abnormality, of which whole-chromosome aneuploidies are the most common (Sahoo et al., 2017). Trisomy 7 is reportedly the most frequently detected chromosomal abnormality (Pertile et al., 2017; Pescia et al., 2017). Human chromosome 7 has been a focus of research, as it exhibits a high proportion of segmentally duplicated sequences (8.2%) (Hillier et al., 2003). Chromosome 2 is unique to the human lineage in being the product of a head-to-head fusion of two intermediate-sized ancestral chromosomes (Hillier et al., 2005). The features of chromosome 2 and 7 render them vital in human growth and development; any mutations therein can have disastrous phenotypic consequences. Therefore, trisomy 2 and 7 may result in early spontaneous miscarriage (Yuan et al., 2017). Thus, detection of RAAs can explain some miscarriages and provides important information for medical management, reproductive counseling, and supportive patient care.
One sample exhibited six chromosomal aneuploidies. Validation using an amniocentesis sample showed that this fetus had a normal karyotype, while aCGH analysis showed several microduplications on chromosomes 2, 4, 8, 14, and 22; of these, only chromosome 14 yielded a positive NIPT result. However, the microduplications were nonpathogenic repeats; that is, the mother was of a normal karyotype. A review of her medical history showed that she had suffered from uterine leiomyoma before becoming pregnant. The incidence of uterine fibroids associated with pregnancy is 0.5–1.0% (Sheiner et al., 2004). Several other reports of discordant NIPT results caused by maternal cancer are extant (Osborne et al., 2013; Amant et al., 2015; Bianchi et al., 2015), thus confirming our findings. Although cancer during pregnancy is relatively rare (incidence, 1 per 1000 pregnancies) (Snyder et al., 2016), an NIPT result showing multiple aneuploidies is a matter of concern.
The karyotyping results indicated several false positives on the three common chromosomes (chr13, chr18, and chr21). One discordant result of T21 was due to maternal CNV; that is, a 10 MB microduplication on 21q11.2–21q12.1. Hartwig et al. (2017) reported that maternal CNV can lead to false-positive or -negative NIPT results, confirming the findings of prior studies (Snyder et al., 2015; Zhang et al., 2015). Our results are consistent with these previous reports. Therefore, maternal CNV is an important cause of discordant NIPT results. Besides, a recent study (Pescia et al., 2017) suggested that there are still two principal reasons which can also cause discordant result of NIPT, one was a low fetal fraction, which could not be detected under current conditions, and the other was likely due to placenta mosaic.
NIPT has high sensitivity and specificity for screening for fetal aneuploidy; however, most centers offering NIPT services lack experience with discordant results. Detection of RAAs by NIPT can sometimes explain the discordant results of NIPT and assist assessment of the health of the fetus. In addition, detection of multiple aneuploidies in NIPT is an indicator of cancer in the mother.
Conclusions
The method developed to test RAAs shows promise, as it enables comprehensive assessment of chromosomes 1–22 and increases the accuracy of NIPT results.
Footnotes
Acknowledgments
The work was supported financially by the Key Program for Health Care Collaborative Innovation of Guangzhou (Grant Nos. 201400000004-4 and 201500000004-4), the Science and Technology Program of Guangzhou (Grant No. 201604020104, 2060404), and the Science and Technology Program of Guangdong (Grant No. 2015A030401040).
Disclosure Statement
No competing financial interests exist.