
Abstract
Single-nucleotide polymorphisms (SNPs) in the ESR1/ESR2 genes play a role in osteoporosis (OP). Our objective was to determine associations of polymorphisms in ESR genes with OP and fracture, SNP–SNP interactions, and involvement of comorbidities. We analyzed 170 Mexican osteoporotic women (FNOP), 173 with hip fracture (HFx), and 210 controls. The SNPs, ESR1 rs2234693CC, rs851982CC and rs1999805AA, were associated with reduced OP risk (odds ratios [ORs] = 0.35, 0.40 and 0.32, respectively; p < 0.05); rs2234693CC was associated with reduced fracture risk (OR = 0.24; p < 0.05). The obese/overweight carriers of rs9340799GG had a lower OP (OR = 0.15, p = 0.016) and fracture (OR = 0.12, p = 0.0057) risk. The rs9479055AA and rs3020404AA hypertensive carriers had a higher OP risk (OR = 5.96, p = 0.032; and OR = 5.29, p = 0.02, respectively).
In addition, rs3020404AA had a higher risk of fracture (OR = 4.90, p = 0.045). The rs2228480GG hypertensive carriers had a higher risk of fracture (OR = 6.22, p = 0.0038). We found a synergic relation between the ESR1 rs3020331 and rs1999805 in femoral neck OP and HFx. The rs2234693 (PvuII) and rs9340799 (XbaI) polymorphisms are associated with a high risk forming a haplotype. The epistasis analysis suggests the contribution of both genes (ESR1/ESR2) to the risk of OP and fracture. Epistasis and involvement of obesity and hypertension lead to a significant modification of the risk.
Introduction
The equilibrium between bone formation and resorption is directly related to osteoblast and osteoclast quantity and activity and determines bone quantity and quality. Estrogen receptors, alpha (ESR1) and beta (ESR2), regulate the transcription of genes involved in bone metabolism acting as transcription factors by binding to DNA or by interacting with other transcription factors. The effects of estrogens on bone are mediated principally by ESR1, but ESR2 plays a role (Noirrit-Esclassan et al., 2021).
Estrogens have a proapoptotic effect in osteoclasts and antiapoptotic effects in osteoblasts (Krum et al., 2008; Martin-Millan et al., 2010); their protective effects on bone include the induction of osteoprotegerin expression in osteoblasts and the repression of pro-osteoclastic cytokine expression by inhibiting nuclear factor kappa B (Bord et al., 2003; Krum et al., 2010). Estrogen deficiency has been associated with increased levels of cytokines that induce osteoclast differentiation. Some of the consequences of the decrease in estrogen levels in postmenopausal women are reduction of bone mineral density (BMD), osteoporosis (OP), and increased risk of fractures (Fx).
Genetic factors participate in OP onset and development. Polymorphisms in genes of bone metabolism have been studied in relation to OP and Fx. Among the most widely studied single-nucleotide polymorphisms (SNPs) are the SNPs in the ESR1 gene, especially the rs9340799 (XbaI) and rs2234693 (PvuII) SNPs, with different results depending on ethnicity (Holliday et al., 2011; Sonoda et al., 2012; Paternoster et al., 2013; Wang et al., 2018; Zhu et al., 2018; Saoji et al., 2019).
OP involves the interaction between genetic and environmental risk factors (Bijelic et al., 2016, 2017). The prevalence of several risk factors, such as obesity and diabetes, potentially increases with age. There is an important relationship between obesity and bone, but whether obesity is a protective or a risk factor for OP is still under discussion (Greco et al., 2015). The presence of diseases, such as type 2 diabetes (T2D), cardiovascular disease, hypertension, arthritis, and other old age-related diseases (Pouresmaeili et al., 2018) and genetic variants, has an impact on the risk of OP; studying them together and considering their interactions, could minimize discrepancies in the association of several genetic variants in different populations.
This study aimed to determine the association of 13 polymorphisms in the ESR1 and ESR2 genes, evaluate the SNP–SNP interaction, the involvement of comorbidities, and the additive effect of the SNPs on the risk of OP and hip fracture (HFx) in Mexican women.
Materials and Methods
This study was reviewed by the Institutional Review Board, which assigned the registration number 14/16, after approval. All procedures were performed in accordance with the Declaration of Helsinki, revised in 2013.
Subjects
The study included 553 Mexican women: 170 women with femoral neck osteoporosis (FNOP), 173 women with HFx, and 210 controls (without OP, HFx, or osteopenia). Women were not related, and had at least three generations of Mexican Mestizo ancestry. All the participants and their ancestors were born in the central, southern, and southeastern regions of Mexico. The participants agreed to participate by signing a consent form.
Bone mineral density
Women were classified (osteoporotic and nonosteoporotic) in accordance with the World Health Organization statements, by densitometric analysis (femoral neck and lumbar spine) (Hologic 2000; Hologic, Inc., San Francisco, CA).
Genotyping
Genomic DNA was obtained (PUREGENE DNA Extraction Kit, PUREGENE Blood Core Kit; Qiagen, Minneapolis, MN) and genotyped for rs2234693, rs2228480, rs9340799, rs9371557, rs9479055, rs4870044, rs3020331, rs851982, rs3020404, rs1999805, and rs1801132 in ESR1; and rs4986938 and rs1256031 in ESR2, by real-time PCR with TaqMan probes (Applied Biosystems, Foster City, CA). Reactions were performed in a StepOne Real-Time PCR System (Applied Biosystems) in a 25 μL reaction (1 × TaqMan PCR master mix, specific probe 100 nm, primers 900 nm each and 25 ng of genomic DNA) cycling with an initial denaturation step at 95°C for 10 min followed by 40 cycles at 92°C for 15 s and 60°C for 1 min.
Statistical analysis
Hardy–Weinberg equilibrium (HWE), unconditional logistic regression models and odds ratios (ORs) with 95% confidence intervals (CIs), were calculated with SNPStats software (
Results
The rs4986938 polymorphism deviates from the HWE (p = 0.00013). All other polymorphisms were in HWE in controls. The mean age of the patients was 70.22 ± 9.44 years (FNOP) and 74.1 ± 9.87 years (HFx); the controls were 57.7 ± 8.42 years. Age, BMI, age at menarche, coffee intake, hypertension, T2D, and the number of children, were significantly different in both groups; age at menopause was different only in the FNOP group. Smoking, glucocorticoid intake, and arthritis did not differ significantly. All the principal characteristics of the studied groups are shown in Table 1.
Characteristics of Women with Femoral Neck Osteoporosis, Women with Hip Fracture, and Controls
Significant values are shown in bold.
Standard deviation.
Femoral neck osteoporosis.
Hip fracture.
Body mass index.
BMI, body mass index; FNOP, femoral neck osteoporosis; HFx, hip fracture; SD, standard deviation.
Association of polymorphisms
The rs2234693 CC was associated with a reduced risk of OP (OR = 0.35 [0.14–0.84], p = 0.014 and OR = 0.31 [0.13–0.72], p = 0.0053) and HFx (OR = 0.24 [0.09–0.59], p = 0.0023 and OR = 0.22 [0.09–0.54], p < 0.0001). On the other hand, the rs851982 CC (OR = 0.40 [0.17–0.92], p = 0.028) and rs1999805 AA (OR = 0.36 [0.16–0.79], p = 0.0021 and OR = 0.32 [0.16–0.62], p < 0.0001) were associated with a reduced risk of OP. In addition, rs3020404 showed a trend toward reduced risk of FNOP (OR = 0.54 [0.30–0.99], p = 0.053). None of the ESR2 polymorphisms showed an association (Table 2 and Supplementary Table S1).
Association of the ESR1 and ESR2 Polymorphisms with Femoral Neck Osteoporosis and Hip Fracture
The models with significant or marginally significant associations are shown; significant and marginally significant values are shown in bold.
Femoral neck osteoporosis.
Crude data.
Adjusted by age and BMI.
Hip fracture.
CI, confidence interval; OR, odds ratio; SNP, single-nucleotide polymorphism.
Comorbidities
The obese/overweight carriers of rs9340799 GG, had a reduced risk of FNOP (OR = 0.15 [0.04–0.63], p = 0.016) and HFx (OR = 0.12 [0.03–0.58], p = 0.0057). The AA genotype was a protector against OP and Fx in overweight/obese women (OR = 0.2 in both cases). On the other hand, hypertensive carriers of rs9479055 AA, have an almost sixfold increase in the risk of OP compared with nonhypertensive women (OR = 5.96 [1.65–21.52], p = 0.032) and the same occurred with rs3020404 AA carriers, with a fivefold risk of FNOP (OR = 5.29 [1.63–17.19], p = 0.02) and HFx (OR = 4.90 [1.52–15.76], p = 0.045). Furthermore, ESR1 rs2228480 GG carriers with hypertension had a sixfold higher risk of HFx (OR = 6.22 [2.41–16.02], p = 0.0038) (Table 3). Neither T2D nor arthritis analysis showed significant associations and are not shown.
Association of ESR1 and ESR2 Polymorphisms by Comorbidities in Women with Femoral Neck Osteoporosis and Hip Fracture
Significant values are shown in bold.
Femoral neck osteoporosis.
Adjusted by age.
Adjusted by age and BMI.
Hip fracture.
SNP–SNP interaction
The best prediction model of SNP combinations in the FNOP group included 6 SNPs; the model that included the 11 polymorphisms showed an adequate CVC; however, the accuracy was barely 0.52 (Table 4). There was a strong synergy between ESR1 rs3020331 and rs1999805, ESR1 rs9479055 and rs1801132, and ESR1 rs2234693 and ESR2 rs1256031 in FNOP (Fig. 1). The correlation between ESR1 rs9371557 and ESR2 rs4986938 is invalid because rs4986938 is not in HWE. The model 11, included all the analyzed ESR1 and ESR2 polymorphisms that showed interactions.

Dendrograms of SNP–SNP interaction on OP and fracture risk. FNOP, femoral neck osteoporosis; HFx, hip fracture; SNP, single-nucleotide polymorphism.
Models of SNP-SNP Interaction in Femoral Neck Osteoporosis and Hip Fracture
Risk estimate was based on the combination and dichotomization of the distribution of genetic factors according to the MDR software. Best models are shown in bold.
Femoral neck osteoporosis.
Testing balanced accuracy.
Crossvalidation consistency.
OR-multifactor-dimensionality reduction
Hip fracture.
MDR, multifactor dimensionality reduction.
In HFx, the best model, had four polymorphisms with CVC 7/10 and an accuracy of 0.58. The dendrogram shows synergistic interactions among ESR1 rs851982 and ESR2 rs1256031. Again, a stronger synergistic relationship was observed with rs3020331 and rs1999805, while the couple formed by rs3020331 and rs1999805 interacted in a synergistic way with rs2234693 (Fig. 1). Models with more than 10 SNPs gave infinite OR values and very wide CIs, and were not included in Table 4.
Haplotypes
In the FNOP group, two blocks with strong LD (D’ > 0.8) were found. FNOP block 1: rs3020331/rs851982 (D’ = 0.88, r 2 = 0.77) and FNOP block 2: rs2234693/rs9340799 (D’ = 0.96, r 2 = 0.72). A third block had an important LD, rs9479055/rs4870044 (D’ = 0.74, r 2 = 0.51). FNOP block 1, had 4 haplotypes, CT (61.9%), TC (32.6%), CC (2.8%), and TT (2.7%); and FNOP block 2 had 3 haplotypes, TA (67.7%), CG (25.2%), and CA (6.5%) (Fig. 2). There were no associations of ESR1 haplotypes with FNOP. On the other hand, block 3 presented 4 haplotypes, AC (49.7%), CT (36.5%), CC (7.8%), and AT (6%), and the latter (AT), was associated with a high risk of FNOP (OR = 2 [1.08–3.68], p = 0.027).
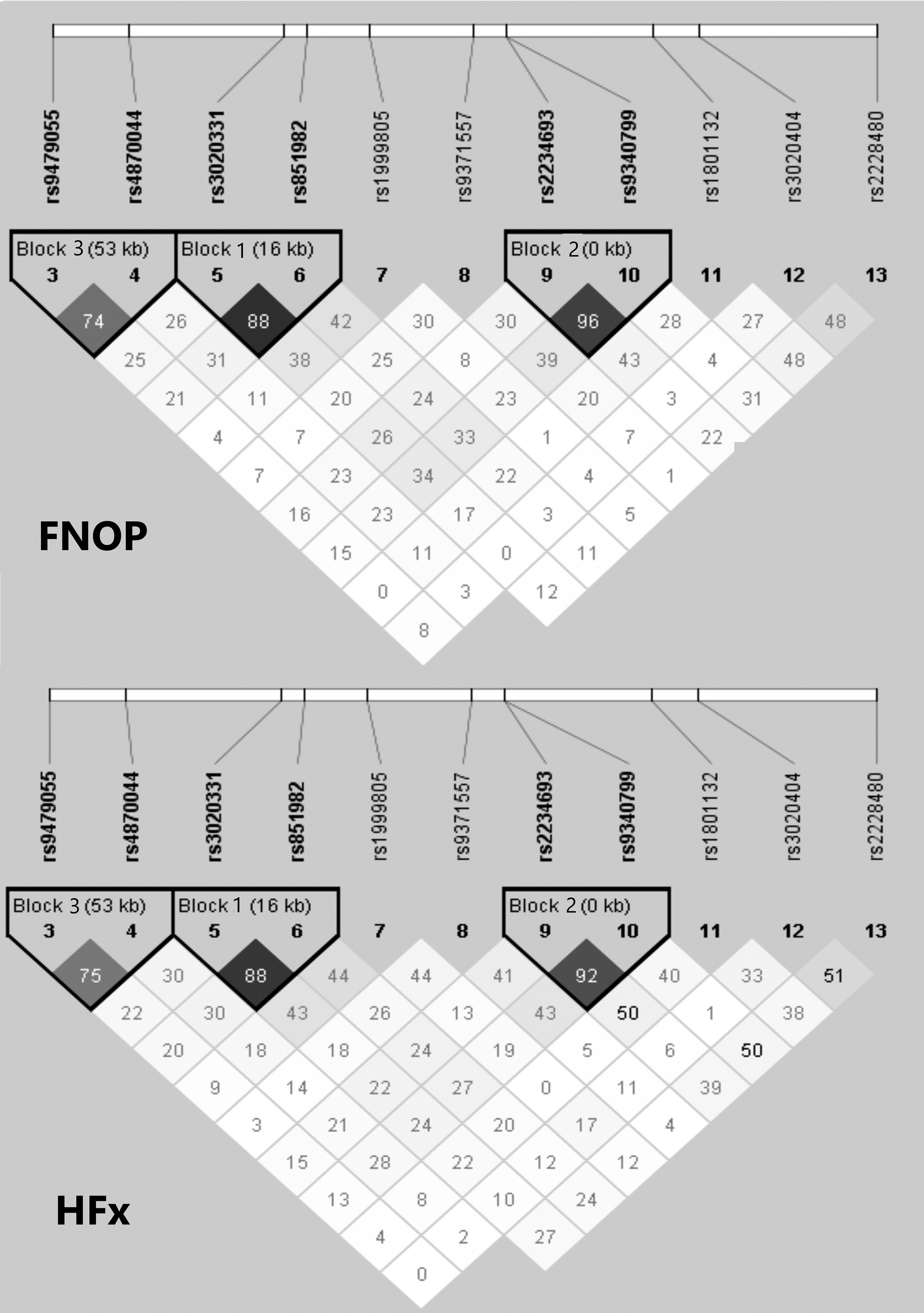
Linkage disequilibrium plot for 11 selected SNPs within ESR1 (HaploView), in samples of women with femoral neck osteoporosis (FNOP) and Hip fracture (HFx). Haplotype blocks were constructed by using the Solid Spine method. ESR1 rs3020331 was located in a linkage disequilibrium block with rs851982. ESR1 rs2234693 and rs9340799 were located in another linkage disequilibrium block nearby. ESR1 rs9479055 was located in a linkage disequilibrium block with rs4870044.
In women with HFx, two strong LD blocks in ESR1 were found: HFx block 1: rs3020331/rs851982 (D’ = 0.885, r 2 = 0.74) and HFx block 2: rs2234693/rs9340799 (D’ = 0.922, r 2 = 0.649); with important linkage disequilibrium at the HFx block 3: rs9479055/rs4870044 (D’ = 0.754, r 2 = 0.49). HFx block 1 presented four haplotypes: CT (60.6%), TC (32.9%), CC (3.9%), and TT (2.6%). None of these was associated with HFx.
Block 2 presented 4 haplotypes: TA (67.4%), CG (24.3%), CA (6.9%), and TG (1.4%) (Fig. 2). The TG haplotype presented an association with a high risk of HFx (OR = 4.95 [1.04–23.4], p = 0.03). For haplotype construction with all ESR1 SNPs (rs9479055, rs4870044, rs3020331, rs851982, rs1999805, rs9371557, rs2234693, rs93400799, rs1801132, rs3020404, and rs2228480) the haplotype CTCTGATACGA was the most frequent (FNOP, 6.8% and HFx, 7.1%).
Discussion
Consistent with the protective role of estrogens against OP and fracture, women in the control group showed a significantly younger age at menarche than women with FNOP and women with HFx as has been stated (Zhang et al., 2018). Age at menopause occurred later in controls than in FNOP and HFx cases, although it was significant only in the FNOP group. These findings confirm that the longer the period of estrogen production, the lower the bone loss and OP risk (He et al., 2021). On the other hand, most women in the control group had fewer than four children, supporting that having too many children affects the bone quality (Yang et al., 2020) and could predispose women to OP.
Association of ESR polymorphisms
rs2234693 CC was associated with an almost threefold reduction in the risk of OP and a fourfold reduction in the risk of fracture (OR = 0.35 and OR = 0.24, respectively; Table 2), in line with previous reports for other populations (Bustamante et al., 2007; Shang et al., 2016; Mondockova et al., 2018).
Our findings were opposed to those obtained with Chinese postmenopausal women (Shu et al., 2020), which showed no association with BMD or with OP. ESR1 rs851982 CC was associated with less than half of the OP risk (OR = 0.4) than the other genotypes. This result confirms the association obtained in a previous study with Mexican women, which included some samples of the same cohort of this study (Hidalgo-Bravo et al., 2019). The rs1999805 AA genotype showed an association with an approximately three times lower risk of FNOP than the genotypes containing a G allele in the recessive model (OR = 0.32; Table 2). In contrast, AA was associated with a high risk of fracture in Chinese postmenopausal women (Luo et al., 2014).
In our study, the fracture group did not show an association, however, a nonsignificant trend toward protection (OR = 0.58; Supplementary Table S1) was observed with the AA genotype, unlikely to be reported by Luo et al. Ethnic differences in allele frequencies could be one of the reasons for discrepancies in associations between populations.
Obesity
The contribution of obesity to OP risk has been questioned and remains unclear. It has been proposed that it could be a protective or risk factor against fractures, depending on the fracture site (Greco et al., 2015; Sotiriadi-Vlachou, 2017; Walsh and Vilaca, 2017; Fassio et al., 2018; Gkastaris et al., 2020), but it is generally accepted that there is a positive correlation between BMI and BMD.
Women with overweight and obesity were more common in the control group. In contrast, normal weight and underweight women were more common in the FNOP and HFx groups showing significant differences (Table 1), according to the protective role of obesity, which has been proposed (Dytfeld et al., 2011; Sotiriadi-Vlachou, 2017). A significant association of rs9340799 GG with protection, was detected when women were classified by BMI (OR = 0.15 and OR = 0.12, respectively; Table 3).
The assessment of the role of several polymorphisms in this study, could not be established because most of the groups had too few samples (or no samples) for the analysis (Supplementary Table S2). Since obesity, OP, and fragility fractures can frequently coexist in patients, there are many questions to resolve, and further studies are needed, including determinations of lean and fat mass as well as classifying patients by obesity categories and fracture sites to confirm the apparently protective role of obesity.
Hypertension
High blood pressure is considered a risk factor for OP. It has been proposed that the renin–angiotensin system plays a crucial role in OP by indirect stimulation of osteoclast formation by induction of RANKL expression by osteoblasts (Asaba et al., 2009). Hypertensive carriers of rs9479055 AA showed a significant association with a sixfold higher risk of FNOP (OR = 5.96, Table 3). Furthermore, hypertensive carriers of rs3020404 AA had a more than fivefold increased risk of FNOP and HFx (OR = 5.29 and OR = 4.90, respectively; Table 3).
Our results indicate that, hypertension notoriously increases the risk of OP in carriers of several ESR1 polymorphisms, supporting previous reports, which have documented that hypertensive women have a higher risk of OP and fragility fracture (Li et al., 2017). The lack of association of other polymorphisms might be due to the limited number of samples with each genotype (Supplementary Table S2).
T2D has been associated with high BMD and an increased risk of HFx. Alterations might induce augmented cortical porosity explaining the increased risk of fractures. On the other hand, T2D frequently coexists with obesity, which could explain the high BMD in these patients (Walsh and Vilaca, 2017; Rathinavelu et al., 2018). The lack of association in our study (data not shown) might be due to the limited number of samples with some genotypes; it needs to be evaluated in a larger sample of Mexican women.
In postmenopausal women with rheumatoid arthritis, the prevalence of OP is much higher (Sapir-Koren and Livshits, 2017), possibly due to glucocorticoid intake and chronic inflammation. However, in our study, the frequency of arthritis in FNOP and HFx was very low and there were no significant associations (data not shown).
SNP–SNP interaction
The cumulative risk of the polymorphisms indicates synergy between them (Table 4). The epistasis analysis suggests the contribution of both, the ESR1 and ESR2 genes to OP and fracture risk. The interaction of ESR1 rs3020331 and rs1999805 revealed this effect as a critical factor that has a role in the risk of OP and HFx (Fig. 1). The MDR interaction graphs (not shown), indicated information gain in FNOP and HFx. The combined effect of the two variants gave an increase in entropy of 3.21% and 2.87%, respectively.
Haplotypes
The frequencies of the haplotype rs2234693 ((PvuII)/rs9340799 (XbaI), in this and other studies with Mexican populations, are consistent with those reported in Caucasian populations, mainly in Italian and English women, and were different from those reported for Japanese populations (Kobayashi et al., 1996; Becherini et al., 2000; Albagha et al., 2001; Carrillo-Moreno et al., 2019).
Previous studies showed a TA haplotype (px) relationship with low lumbar spine BMD and increased vertebral fracture risk (van Meurs et al., 2003). Korean women carrying the TG (pX) haplotype had lower BMD values at the trochanter (Nam et al., 2005). In this study, the TG haplotype was associated with high fracture risk. In contrast, Albagha et al. (2005), found that the TA (px) haplotype was related to femoral neck bone loss in postmenopausal Scottish women (Albagha et al., 2005). Our results are in line with the meta-analysis by Tang et al. (2013), which found that carriers of haplotypes with the rs2234693 T allele have an increased risk of fractures in the Caucasian population (Tang et al., 2013).
Interestingly, the allele associated with risk was the most frequent in this study (T, ∼70%) and the TT genotype (about 50%). On the other hand, the CC genotype, associated with protection against FNOP and HFx (Table 2), is the less frequent genotype in our population. The TT genotype did not reach significance in the single analysis, but the OR indicated higher risk (OR = 1.52 and OR = 1.4 for FNOP and HFx, respectively; data not shown) as reported.
Conclusions
The ESR1 polymorphism rs2234693 (PvuII) was associated with OP and fracture in a single form and as a haplotype with rs9340799 (XbaI). The MDR analysis indicated that SNP–SNP interactions modify the risk and suggests that a greater number of risk variants present in a sample of women of the Mexican Mestizo population, may generate a higher risk of developing OP and fracture. Even when several polymorphisms did not show an association with FNOP or HFx in the single analysis, their interactions could influence the risk. BMI and hypertension are critical factors in OP and fracture risk, emphasizing the importance of analyzing several intervening factors in assessment of risk, in complex diseases such as OP.
Footnotes
Authors' Confirmation Statement
All authors agree to publish this article.
Acknowledgments
The authors would like to express gratitude to all patients that kindly participated in the study.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by Consejo Nacional de Ciencia y Tecnología under Grant SALUD-2007-C01-69706 and by the research budget assigned to the authors from the Instituto Nacional de Rehabilitación Luis Guillermo Ibarra Ibarra.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.