
Abstract
Compared with other breast cancer subtypes, triple negative breast cancer (TNBC) is an aggressive malignancy with a high recurrence rate and reduced overall survival. Immune checkpoint inhibition (ICI) has shown modest results in this subgroup, highlighting the need for improved targeted therapeutic options. Notch is a defining feature of TNBC and drives the expression of interleukin-1 beta (IL1β) and C-C motif chemokine ligand 2 (CCL2). These cytokines are involved in the recruitment of tumor-associated macrophages (TAMs) to the tumor, resulting in immune evasion and tumor progression. Targeting Notch, IL1β or CCL2 may reduce TAM recruitment and resistance to ICI, illuminating the potential of combination immunotherapy in TNBC.
Introduction
Breast cancer is a heterogenous disease, with multiple subtypes that display different patterns of gene expression, prognosis, and response to treatment (Sorlie et al, 2001). Clinically, breast cancer is classified by the presence or absence of three markers: estrogen receptor (ER-positive), progesterone receptor (PR-positive), and human epidermal growth factor receptor 2 (HER2-positive). Triple negative breast cancer (TNBC) lacks the expression of these markers, rendering endocrine and HER2-directed therapies inutile. TNBC accounts for ∼15% of invasive breast cancers, primarily affects young women, those of African or Hispanic ancestry, and individuals with BRCA1 mutations. Despite current treatments efforts, compared with other breast cancer subtypes, TNBC has a high rate of recurrence and poor overall survival (OS) (Liedtke et al, 2008). There is, thus, an unmet need for improved therapeutics in this subpopulation of patients.
Targeting the immune system is one therapeutic approach that has been evaluated across a range of tumor types for the past decade. Immune targeting agents include cancer vaccines, chimeric antigen receptor T cell transplantation, and immune checkpoint inhibition (ICI). The overarching aim of these immunotherapies is to boost cancer-specific T cell responses. Despite these advances, durable clinical responses have been appreciated in a minority of cancer patients, and the benefits seen among patients with breast cancer have been modest. This underscores the need for a deeper understanding of the immune tumor microenvironment (TME) and how its configuration predicts outcome and therapeutic response for women with breast cancer.
The objectives of this review are to summarize the current treatment landscape for TNBC, to explore the biological rationale for an immune targeted approach in TNBC, and to examine the current clinical evidence to support immunotherapy in TNBC. Finally, we will discuss the Notch pathway as a novel target that may potentiate the effects of immunotherapy for patients with TNBC.
Current Treatments of TNBC
Standard therapy for TNBC involves surgery, radiotherapy, chemotherapy, and more recently immunotherapy. The type of surgery, location of radiotherapy, as well as choice and order of chemotherapy/immunotherapy (before or after surgery) depends on the tumor characteristics (stage, type, and immune biomarkers), in addition to patient factors and preferences (Gradishar et al, 2022).
For early-stage TNBC (stages I–III), breast-conserving surgery (BCS; lumpectomy) is often recommended in conjunction with surgical staging of the axillary lymph nodes by sentinel lymph node biopsy. Radiation follows BCS and may be limited to the chest wall or the axillary region depending on whether tumor is present within the axillary lymph nodes. Mastectomy is reserved for tumors too large for BCS or where radiotherapy is contraindicated.
For patients with TNBC, chemotherapy may be given before surgery (neoadjuvant chemotherapy, NAC) or after surgery (adjuvant chemotherapy). NAC is indicated for tumors that are palpable or T1c and larger (Gradishar et al, 2022). NAC may also be used to convert inoperable tumors to operable, to eliminate the need for mastectomy or axillary lymph node dissection, and to gauge tumor response in vivo. Clinical T1a/b tumors can undergo upfront surgery and possible de-escalation of chemotherapy depending on pathological stage confirmed after excision (Gradishar et al, 2022). Neoadjuvant or adjuvant regimens usually include some combination of an anthracycline (doxorubicin or epirubicin), alkylating agent (cyclophosphamide), taxane (paclitaxel or docetaxel), and consideration of platinum agent (carboplatin).
A PARP inhibitor (olaparib) may also be used in the adjuvant setting if the patient has a BRCA1/2 mutation (Tutt et al, 2021). NAC may also inform adjuvant treatment decisions, as guidelines support the use of the antimetabolite capecitabine in patients with residual disease (Gradishar et al, 2022; Masuda et al, 2017). For late-stage TNBC (stage IV) or breast cancer metastasis, chemotherapy is the mainstay of treatment. Microtubule inhibitors (vinorelbine or eribulin) (Cortes et al, 2011; Zelek et al, 2001) or antibody-drug conjugates such as sacituzumab govitecan (Bardia et al, 2021) may be used for late-stage TNBC in addition to the agents mentioned earlier.
Although TNBC initially responds favorably to chemotherapy, recurrence commonly occurs (De Giorgi et al, 2007; Dent et al, 2007). For TNBC patients who do not achieve pathological complete response (pCR) with NAC, relapse rates are especially high (Cortazar et al, 2014; Soares et al, 2021; Spring et al, 2020; von Minckwitz et al, 2012; Yee et al, 2020). Despite current treatments, median OS is only 11–18 months in the metastatic setting (Aly et al, 2019; den Brok et al, 2017; Kassam et al, 2009; Li et al, 2019; Skinner et al, 2021), with objective response rates (ORR) to first-line single agent chemotherapy ranging from 12% to 30% (Awada et al, 2014; Baselga et al, 2013; Li et al, 2019; Miles et al, 2013; Trédan et al, 2015). Therefore, more targeted therapeutic options are needed for this aggressive subgroup of breast cancer.
Immunotherapy
TNBC is characterized as highly infiltrated with immune cells, mainly tumor infiltrating lymphocytes (TILs) and tumor-associated macrophages (TAMs) (Bingle et al, 2002; Denkert et al, 2018; Leek et al, 1996; Loi et al, 2019; Park et al, 2019). Clinically, elevated TAMs have been associated with poor prognosis in breast cancer (Bingle et al, 2002; Leek et al, 1996; Paik et al, 2004), whereas TILs are associated with improved outcome (Adams et al, 2014; Denkert et al, 2010; Garcia-Teijido et al, 2016; Loi et al, 2013; Savas et al, 2016). This immune-cell-rich TME creates a favorable condition for the use of immunotherapy and blocking immune checkpoint pathways. The normal function of immune checkpoint pathways (e.g., programmed death 1 [PD-1]/programmed death ligand 1 [PDL-1] or cytotoxic T lymphocyte-associated protein 4 [CTLA4]) is to blunt immune responses and promote self-tolerance by inhibiting effector T cell activity and enhancing the function and development of regulatory T cells (Tregs) (Francisco et al, 2010; Gianchecchi et al, 2013).
Pathologically, immune checkpoints are a prominent mechanism of immune escape in cancer by instead attenuating host immune response to tumor cells. Immune checkpoint inhibitors (ICIs) can, for example, target PD-1 on TILs or PDL-1 on tumor cells and TAMs, thus restoring TIL function and allowing the immune system to target and destroy the cancer (Pardoll, 2012). Indeed, recent clinical trials in other tumor types such as lung cancer and melanoma have demonstrated ICIs can generate durable remissions and impressive OS benefits (Baas et al, 2021; Eggermont et al, 2021; Eggermont et al, 2018; Eggermont et al, 2016; Fehrenbacher et al, 2016; Gandhi et al, 2018; Hodi et al, 2010; Luke et al, 2022; Reck et al, 2016).
Given that TNBCs also have high PDL-1 expression (Cimino-Mathews et al, 2016; Gatalica et al, 2014; Mittendorf et al, 2014; Sabatier et al, 2015), ICIs have recently been investigated in this tumor type (Keenan and Tolaney, 2020). Unfortunately, efficacy of ICIs as a single agent is low, with monotherapy ORRs ranging from 5% in unselected patients, to 21% in treatment-naive PDL-1 positive patients (Adams et al, 2019a; Adams et al, 2019b; Dirix et al, 2018; Emens et al, 2019; Nanda et al, 2016; Winer et al, 2021). The first phase III trial of immunotherapy in unresectable, locally advanced or metastatic TNBC (IMpassion130) compared nab-paclitaxel plus atezolizumab—a monoclonal antibody targeting PDL-1—with nab-paclitaxel alone, and demonstrated improvements in ORR (56.0% vs. 45.9%, respectively, p = 0.002) (Schmid et al, 2018).
In the subgroup of patients with PDL-1 positive tumors, atezolizumab plus nab-paclitaxel resulted in a 7 month improvement in median OS compared with nab-paclitaxel alone (25.0 months vs. 18.0 months, Hazard Ratio [HR]: 0.71), as well as an improvement in progression-free survival (PFS) of 7.5 months versus 5.3 months (HR: 0.63, p < 0.0001) (Schmid et al, 2020b; Schmid et al, 2018). Importantly, before this trial, no other targeted agent had shown a survival benefit in this population. These results led to the accelerated U.S. Food and Drug Administration (FDA) approval of atezolizumab plus nab-paclitaxel as a first-line treatment for PDL-1 positive metastatic TNBC (FDA, 2019), establishing the first immunotherapy approval in breast cancer. Disappointingly, approval was later withdrawn after a subsequent trial (IMpassion131) failed to meet the primary end point of PFS superiority, and in fact demonstrated possible inferior OS in the combination ICI/paclitaxel group (Cancer Network, 2021; Miles et al, 2021).
Pembrolizumab, a humanized anti-PD-1 antibody, has also been extensively studied in TNBC (Adams et al, 2019a, Adams et al, 2019b; Nanda et al, 2016; Winer et al, 2021). In the phase III KEYNOTE-355 trial, TNBC patients with metastatic tumors expressing high levels of PDL-1 were treated with pembrolizumab in combination with standard chemotherapy. Combination treatment showed significant improvements in PFS (9.7 months vs. 5.6 months, HR: 0.65, p = 0.0012) and OS (23.0 months vs. 16.1 months, HR: 0.73, p = 0.0185) compared with chemotherapy alone (Cortes et al, 2022; Cortes et al, 2020). In early (stage II–III) TNBC, KEYNOTE-522 compared standard chemotherapy plus pembrolizumab with chemotherapy alone and demonstrated improvements for combination treatment in pCR (64.8% vs. 51.2%, p < 0.001), and 3-year event-free survival (84.5% vs. 76.8%, HR: 0.63, p < 0.001) (Schmid et al, 2022; Schmid et al, 2020a). KEYNOTE-522 led to approval of the first immunotherapeutic for early-stage TNBC (FDA, 2021).
Pembrolizumab is currently the only National Comprehensive Cancer Network (NCCN)-recommended ICI for TNBC. Neoadjuvant pembrolizumab is recommended in combination with chemotherapy for stage II–III TNBC, with adjuvant pembrolizumab recommended in stage I–III TNBC after preoperative systemic therapy, or as first-line therapy in recurrent unresectable or metastatic disease with a combined positive score ≥10 (Gradishar et al, 2022).
Although ICIs show promise in TNBC, predicting which patients will respond to ICI treatment remains a challenge. Despite PDL-1 being predictive of response in some advanced/metastatic trials (Cortes et al, 2020; Schmid et al, 2020b), this finding was not consistent in the early-stage TNBC trials (Mittendorf et al, 2020; Schmid et al, 2022; Schmid et al, 2020a). These outcomes may be due to several factors, including lack of interchangeability between assays and scoring systems, and poor reproducibility among pathologists (Badve et al, 2022; Bianchini et al, 2016; Rizzo and Ricci, 2022). Regardless, accurate predictive biomarkers of ICI response and strategies to increase response rates are needed.
Targeting Notch Signaling as a Novel Therapy
The Notch signaling pathway plays a crucial role in intercellular signaling and tissue patterning during development (Nichols et al, 2007). Mammals have four Notch receptors (NOTCH1–4) that interact with five Notch ligands (DLL1, DLL3, DLL4, JAG1, and JAG2). Interaction between Notch ligands and their receptors leads to a series of proteolytic events, including the presenilin-protease (γ-secretase)-mediated cleavage of the Notch receptor.
This cleavage liberates the active cytoplasmic domain fragment—intracellular NOTCH (NIC)—from the plasma membrane, which then translocates to the nucleus and initiates the expression of target genes (Callahan and Egan, 2004). Our group and others have shown that JAG1 and Notch activation are hallmarks of TNBC and independent predictors of outcome (Dickson et al, 2007; Reedijk et al, 2008; Shen et al, 2017; Stylianou et al, 2006). However, Notch is also heterogeneously expressed in normal tissues, limiting the clinical utility of anti-Notch therapies due to their side effects (Andersson and Lendahl, 2014; Majumder et al, 2021).
Previously, we discovered that under conditions of cellular stress, such as hypoxia or nutrient deprivation commonly found in the TME, the deubiquitinase USP9x forms a multiprotein complex with pseudokinase tribbles homolog 3 (TRB3) and mind bomb 1 (MIB1), protecting these proteins from ubiquitin-dependent degradation (Izrailit et al, 2017; Izrailit et al, 2013). Stabilization of TRB3 and MIB1 leads to JAG1 transcriptional upregulation and JAG1 ubiquitination, respectively, resulting in Notch pathway activation (Fig. 1). Using a murine TNBC model, we confirmed that USP9x knockdown abrogates Notch activation and decreases tumor growth without the toxicities associated with Notch inhibitors (Jaiswal et al, 2021). This study supports the potential of USP9x inhibition to target Notch in metabolically vulnerable tissues such as TNBC, whereas sparing normal Notch-dependent tissues.
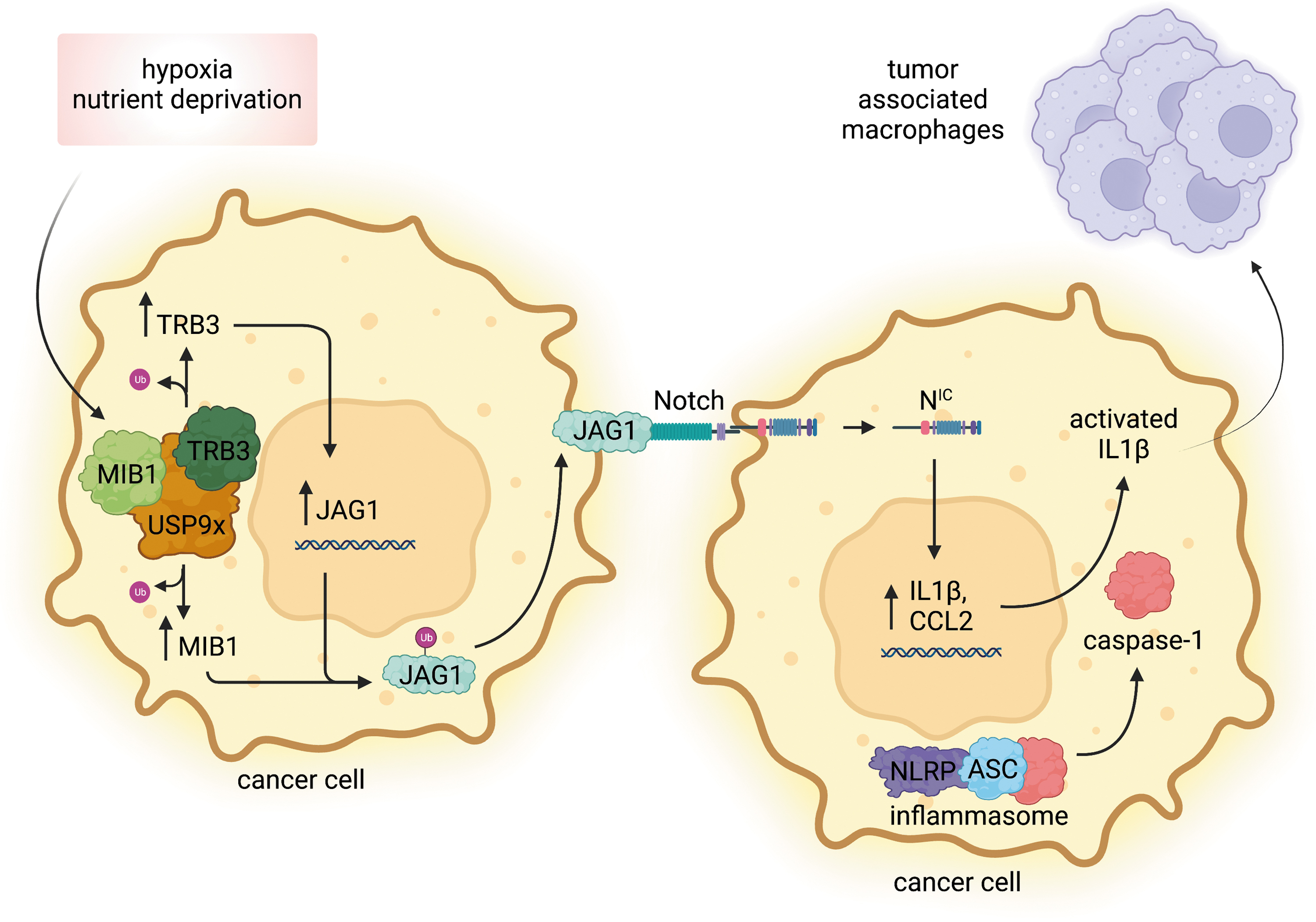
Association between Notch, USP9x, IL1β, and CCL2 in TNBC. Under conditions of cellular stress, such as hypoxia or nutrient deprivation, USP9x forms a multiprotein complex with TRB3 and MIB1, protecting these proteins from ubiquitin-dependent degradation. Stabilization of TRB3 and MIB1 leads to JAG1 transcriptional upregulation and JAG1 ubiquitination, respectively. As a transmembrane ligand, JAG1 interacts with the Notch receptor on an adjacent cancer cell, resulting in the γ-secretase-mediated cleavage of the Notch receptor. This cleavage liberates the active cytoplasmic domain fragment NIC from the plasma membrane, allowing it to translocate to the nucleus and to initiate the expression of IL1β and CCL2. Caspase-1, presumably activated by the inflammasome, cleaves pro-IL1β into its active form. Secreted IL1β then aids in the recruitment of TAMs. Created with
In addition to Notch being a key feature of TNBC, we discovered that Notch activation results in the expression and secretion of interleukin-1 beta (IL1β) and C-C motif chemokine ligand 2 (CCL2) (Shen et al, 2017). Using both in vitro and in vivo models, we found that Notch-driven expression of IL1β and CCL2 also results in the recruitment of TAMs (Shen et al, 2017). Both IL1β and CCL2 are known to have protumoral effects in many tumor types (Hemmerlein et al, 2001; Kim et al, 2013; Lee et al, 2017; McLoed et al, 2016; Mitsunaga et al, 2013; Ohta et al, 2003; Ohta et al, 2002; Tanaka et al, 2009), and have been shown to be associated with macrophage infiltration and poor outcome (Kaplanov et al, 2019; Li et al, 2014; Pollard, 2004; Qian et al, 2011; Saji et al, 2001; Soria et al, 2011; Ueno et al, 2000; Valkovic et al, 1998; Wu et al, 2018).
Confirming these findings, we noted that USP9x inhibition results in changes in the immune TME, with loss of immunosuppressive TAMs and emergence of activated cytotoxic T cells. This remodeling of the TME was also shown to be through IL1β and CCL2 (Jaiswal et al, 2021) (Fig. 1). Furthermore, we correlated the TNBC subtype to elevated expression of inflammasome components apoptosis-associated speck-like protein containing a CARD (ASC), nucleotide-binding oligomerization domain, leucine-rich repeat and pyrin domain containing (NLRP) proteins, as well as caspase-1 (Shen et al, 2017).
The inflammasome, when activated, releases active caspase-1, which is now in position to proteolytically cleave IL1β, as well as IL18 and gasdermin D (Broz and Dixit, 2016; Thornberry et al, 1992). This cleavage promotes maturation and secretion of IL1β, subsequently recruiting TAMs (Fig. 1). TNBC, therefore, contains the adequate machinery for both “priming” of IL1β by driving its expression through Notch activation, as well as “cleavage” of IL1β into its active form by caspase-1. Inhibiting IL1β could, therefore, be used as a novel therapeutic strategy for TNBC.
Interestingly, multiple IL1β inhibitors are already FDA approved and used clinically to treat various autoimmune disorders. Anakinra (Kineret®) is commonly used to treat rheumatoid arthritis patients with a minimal side effect profile (FDA Approved Drug Product, 2020). Rilonacept (Arcalyst®) and canakinumab (Ilaris®) are prescribed for Cryopyrin-Associated Periodic Syndromes (CAPS) (FDA Approved Drug Product, 2016; FDA Approved Drug Product, 2008), whereas canakinumab (Ilaris) is also used to treat Systemic Juvenile Idiopathic Arthritis (SJIA) and Familial Mediterranean Fever (FMF) (FDA Approved Drug Product, 2016). Given that effective and safe IL1β inhibitors already exist, these drugs could be repurposed to treat TNBC without having to undergo the initial drug development phase.
Clinically, the best evidence validating these Notch-driven cytokines as a tumor promoters comes from the Novartis phase III CANTOS trial, where canakinumab was studied as a novel therapy for heart failure patients (Ridker et al, 2017). Although the primary objective of the study was to evaluate differences in major adverse cardiac events, canakinumab also resulted in a >50% reduction in death from all cancers in a cohort of 10,061 patients. More recently, research has demonstrated that air pollution (2.5 μm particulate matter) mediates its increased risk of non-small cell lung cancer (NSCLC) through an influx of macrophages and an increase in IL1β production, thereby promoting carcinogenesis within the lung tissue (Swanton et al, 2022). These findings support the hypothesis that effective IL1β and CCL2 antagonists, either alone or in combination with other immune modifying agents, could provide novel therapeutic opportunities among patients with TNBC with specific immune phenotypes.
Combination with Immune Checkpoint Inhibitors
Correlation between IL1β and PDL-1 expression has been shown in several cancers, including pancreatic, gastric, and NSCLC (Herremans et al, 2022; Li et al, 2020; Lu et al, 2021). In melanoma, the BRAFV600E mutation was found to induce IL1β secretion by melanoma cells, resulting in the increased expression of PDL-1 (Khalili et al, 2012). In hepatocellular carcinoma (HCC), PDL-1 expression on HCC cells was found to be driven through TAM-derived IL1β (Zong et al, 2019). Given this link between IL1β and PDL-1 expression, IL1β could represent a novel marker to predict ICI response.
As well, TAMs have been shown to recruit immunosuppressive Tregs and inhibit TIL function through PD-1/PDL-1 independent mechanisms, thereby providing an extra layer of immune escape for tumors (Bogels et al, 2012; Movahedi et al, 2010; Ruffell et al, 2014). Inhibiting TAM recruitment through IL1β inhibition could relieve this immune attenuation, making tumors more susceptible to ICI (Fig. 2). Indeed, treating mice with an anti-IL1β antibody followed by an anti-PD-1 antibody in a TNBC allograft mouse model resulted in decreased tumor progression compared with either of the treatments alone (Kaplanov et al, 2019). Predictably, combination therapy resulted in increased recruitment of CD8+ TILs to the tumor site compared with the individual treatments.
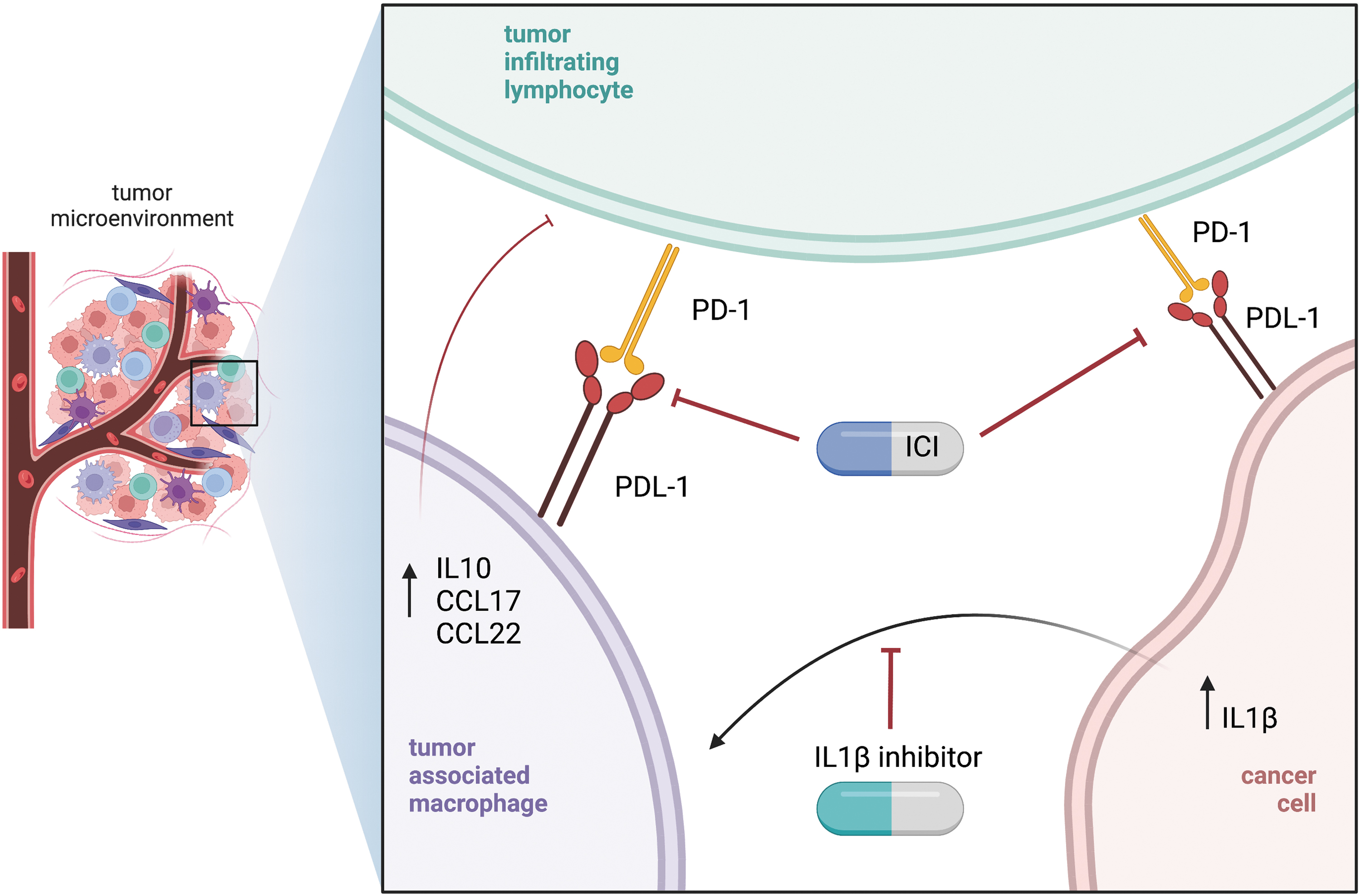
Combination immunotherapy in TNBC. TILs are inhibited through the PD-1/PDL-1 immune checkpoint pathway. TAMs also induce immunosuppression through immune checkpoint-independent mechanisms by inhibiting TILs and recruiting Tregs. Hypothesis: Targeting IL1β could reduce TAM recruitment, increasing susceptibility to ICI. Created with
Clinical trials assessing synergy between ICIs and IL1β inhibition are in progress. After the CANTOS trial, Novartis launched the CANOPY study program, including several randomized phase II and III clinical trials studying canakinumab in combination with pembrolizumab as a potential treatment option for NSCLC (Paz-Ares et al, 2020). The CANOPY-1 trial studied treatment-naive locally advanced or metastatic NSCLC and randomized them to either canakinumab plus pembrolizumab/chemotherapy or pembrolizumab/chemotherapy alone (Tan et al, 2019).
Although the addition of canakinumab did not improve PFS or OS (Tan et al, 2022), potentially clinically meaningful improvements in both PFS and OS were observed among prespecified subgroups of patients with inflammatory biomarkers, for which the analysis is ongoing (Novartis, 2021). CANOPY-N is an ongoing Phase II trial evaluating the use of neoadjuvant canakinumab either as monotherapy or in combination with pembrolizumab for patients with resectable NSCLC (Garrido et al, 2021). The final data collection for this trial is complete and results are expected within the next year (ClinicalTrials.gov, 2022).
Conclusion
TNBC is a devastating disease with poor prognosis and high recurrence rate. Developing improved therapeutics for this subgroup of patients with breast cancer is essential. Notch is a defining feature of TNBC and drives the expression of IL1β and CCL2. Targeting Notch (through USP9x inhibition) or its downstream products IL1β and CCL2 may resensitize TNBCs to ICI by relieving TILs from additional TAM inhibition. If successful, this therapeutic approach could be used in other disease settings where macrophages are a key barrier to therapeutic efficacy.
Footnotes
Authors' Contributions
Conceptualization, investigation, writing—original draft preparation, and visualization by W.M. Writing—reviewing and editing by B.E.W. Conceptualization, writing—reviewing and editing, and supervision by M.R.
Disclosure Statement
No competing financial interests exist.
Funding Information
This review was supported by funds to M. Reedijk from the Canadian Cancer Society (Award #707511), and to W. Marini from the Canadian Institutes of Health Research (Canada Graduate Scholarships—Doctoral, Award #170849) and the Hold‘em for Life Oncology Clinician Scientist Award. This study was also funded in part by the Ontario Ministry of Health and Long Term Care.