
Abstract
Mental health difficulties are highly prevalent and costly, and mental health services are often overwhelmed. Brief and cost-effective interventions are needed to help improve mental well-being. We aimed to test the effect of a nature-based guided imagery (GI) and a nature-based meditation (NBM) on mental well-being and a range of clinically relevant measures over a 2-week period, including three time points. The community sample included 40 individuals (mean age = 38.63, standard deviation = 12.99; gender = 11 males, 28 females, and 1 responded as “nonbinary”). Participants were randomly assigned 1:1 to either the GI or the NBM. Participants were given one audio file to listen to (either GI or NBM), both of which were ∼20 minutes in duration. Similar to previous work, we found evidence for increases in well-being and nature connection immediately following the GI. The results suggest that both the GI and NBM are likely to be effective in improving mental well-being. There were statistically significant increases in well-being, self-compassion, and mindfulness, as well as decreases in rumination, negative affect, and depressive symptoms. There was also evidence for clinically meaningful improvements in depressive symptoms and well-being. This experimental study provides preliminary evidence to support the development of nature-based interventions to improve well-being. Further research is needed to test this in larger and clinical samples, either as an adjunct to therapy or as self-help for those with mild-to-moderate symptoms of depression.
Mental health costs run high in the United Kingdom and a recent estimate puts the figure at approximately £118 billion, annually (McDaid et al., 2022). Mental health services in the United Kingdom are often overwhelmed and some have made the case that the workforce is at breaking point (James, 2022). This naturally may lead to a more reactive “rule of rescue” approach to mental health, typically in the form of treatment (Budd, Iqbal, Harding, Rees, & Bhutani, 2021). The rule of rescue has been defined as “an ethical imperative to save individual lives even when money might be more efficiently spent to prevent deaths in the larger population” (Doughety, 1993, p. 1359). Although traditional treatment approaches are helpful for many with mental health difficulties, both psychological and pharmacological treatment efficacy is moderate at best, with typically less than 50% of patients in remission after therapy (Kolovos et al., 2017; Van Bronswijk, Moopen, Beijers, Ruhe, & Peeters, 2019). This outcome is compounded by high recurrence rates (Burcusa & Iacono, 2007). That is, approximately half of individuals who have recovered from a depressive episode will relapse, and this risk only increases with each subsequent relapse. In addition, treatment efficacy itself for an individual is likely to wane with every relapse (Moriarty et al., 2020). For these reasons, innovation in psychosocial interventions is urgently needed (Pile, Williamson, Saunders, Holmes, & Lau, 2021). Alternative approaches have been explored including focusing on sleep, diet, and exercise (Pomp, Fleig, Schwarzer, & Lippke, 2013) in the field of so-called “lifestyle psychiatry” (Firth et al., 2020). More recently, other novel approaches to intervention have emerged including contact and connection with nature (Lopresti, 2019).
Using nature-based psychological interventions is a nascent and growing area (Bratman et al., 2019; Cooley, Jones, Kurtz, & Robertson, 2020) and may have potential in both preventing and treating common mental health difficulties such as clinical depression (Owens & Bunce, 2022b). One approach in this area has been to develop nature-based meditation (NBM) interventions that have shown promise, yet a dearth of empirical evidence hampers the ability to draw firm conclusions and make recommendations (Djernis, Lundsgaard, Rønn-Smidt, & Dahlgaard, 2023). In a recent study, the effect of a brief nature-based outdoor-guided meditation was tested and found to significantly reduce depressive rumination, defined as the tendency to repetitively analyze the causes, meanings, and consequences of depression (Watkins & Roberts, 2020), depressive symptoms, and increase well-being in young people over the short term, when compared with non-nature-based indoor meditation and attention control (Owens & Bunce, 2022a). However, there are many situations where delivering an intervention (e.g., therapy or self-help) intra natura can be challenging. For example, mental health in-patients, other hospital in-patients confined to bed, those living in urban areas with limited access to green or blue spaces, and mental health or other services with limited capacity, may all struggle to receive or provide a beneficial dose of nature. Similarly, those with busy lives, working, or studying indoors may not always manage to spend enough time in nature to receive benefit. In addition, homework or top-up exercises between therapy sessions may only be possible in certain circumstances by using some form of virtual nature exposure. Several alternatives to being out in nature have been explored, including the use of indoor plants (Han, Ruan, & Liao, 2022), virtual reality (Browning et al., 2019), exposure to forest video (Owens & Bunce, 2023), and digital forest therapy (Reese, Stahlberg, & Menzel, 2022). A further innovative alternative that has shown promise for mental health symptoms in other contexts is guided mental imagery.
Mental imagery is the representation and experience of sensory information in the “mind’s eye” of something real when a percept is absent, or of an entirely imaginary object. It is thought that a common set of neural pathways underly both mental imagery and perception (Dijkstra, Bosch, & van Gerven, 2019; Kosslyn, Ganis, & Thompson, 2001). Guided imagery (GI) takes many forms and is in fact an ancient technique (Krau, 2020). The essence of GI involves external instructions given to guide the recipient to invoke internal multisensory experiences within internal representations in the form of mental images. GI and related interventions, including emotional imagery, can lead to increases in positive emotions (Blackwell & Holmes, 2017; Fredrickson, 2000; Pile, Smith, et al., 2021; Pile, Williamson, et al., 2021; Quoidbach, Mikolajczak, & Gross, 2015; Toussaint et al., 2021), as well as reductions in stress markers such as salivary cortisol (Watanabe et al., 2006), which may allow the immune system to function more effectively (Trakhtenberg, 2009).
Perhaps unsurprisingly given the plethora of benefits in the natural environment (Bratman et al., 2019), GI interventions often include elements of nature (Fredrickson, 2000). A recent study, for example, compared a 10-min nature GI intervention to urban GI and found that those in the nature GI condition increased their self-reported levels of connectedness to nature (Coughlan et al., 2022). Similarly, mental imagery of “restorative” natural environments (e.g., “forest path,” “mountain lake”) has been shown to produce higher levels of relaxation and stronger positive emotional valence when compared to imagery of restorative built and nonrestorative urban environments (Koivisto & Grassini, 2022). Furthermore, Nguyen and Brymer (Nguyen & Brymer, 2018) exposed 48 participants to a nature-based and an urban-based GI recording, randomizing the order of presentation, to assess the effects on self-reported state anxiety. The results of this study showed that while both interventions reduced state anxiety, the nature-based version reduced anxiety significantly more than the urban version.
The aim of the current study was to extend previous work by testing the immediate and mid-term effects of brief nature-based interventions on nature connection and a range of outcomes informed by clinical psychology. These include rumination, depressive symptoms, well-being, affect, mindfulness and self-compassion [“how we relate to ourselves in instances of perceived failure, inadequacy, or personal suffering” (Neff, 2023)]. Given that GI in the present study was nature-based and influenced by psycho-evolutionary nature-related theoretical perspectives including biophilia (Wilson, 1984) and stress reduction theory (Ulrich et al., 1991), we also expected improvements in nature connection.
We hypothesized that rumination would reduce for several reasons. First, other interventions that incorporate mindfulness-based interventions have been shown to reduce rumination (Gu, Strauss, Bond, & Cavanagh, 2015; Winnebeck, Fissler, Gärtner, Chadwick, & Barnhofer, 2017), including those that are nature-based (Choe, Jorgensen, & Sheffield, 2020; McEwan et al., 2021). Furthermore, similar nature-based interventions have shown reductions in rumination (Owens & Bunce, 2022a), with one study suggesting that the effect may be explained to some extent by reduced activity in the subgenual prefrontal cortex, an area implicated in depressive rumination (Bratman, Hamilton, Hahn, Daily, & Gross, 2015). In addition, individuals may ruminate using imagery as well as verbal processes, therefore GI may help individuals to distract themselves in light of repetitive negative thinking (Lawrence, Siegle, & Schwartz-Mette, 2023).
We hypothesized improvements in depression, well-being, and affect over time because the interventions were designed to reduce stress and there is a well-known causal link between stressful life events and clinical depression (Hammen, 2005). Furthermore, the interventions also draw on principles of mindfulness and so we expected change in both decentering and mindful curiosity.
We hypothesized that self-compassion would increase for three reasons. First, interventions that include elements of mindfulness often result in increased self-compassion (Baer, Lykins, & Peters, 2012). Second, attention restoration theory (Kaplan, 1995) suggests that nature exposure facilitates opportunities for “cognitive quiet,” which may allow for self-compassion to emerge (Swami et al., 2019). Third, a theoretical central component of self-compassion is self-transcendence (Miller & Verhaeghen, 2022), defined as reduced self-saliency and increased connection to the environment and others (Yaden, Haidt, Hood, Vago, & Newberg, 2017), and nature experiences of awe or the sublime may in turn give rise to experiences of transcendence. For example, recognizing that there exists something greater than ourselves (Løvoll & Sæther, 2022) may be one experience related to awe and such experiences may increase compassion (Katherine Nelson-Coffey et al., 2019).
We tested two nature-based interventions in this experimental study, rather than using a nonintervention condition (e.g., a waitlist or attentional control). We compared the novel GI with a meditation that has been shown in one study to be effective in improving mental well-being relative to an attentional control group (Owens & Bunce, 2022a). We hypothesized that both the GI and NBM would produce similarly positive benefits to participants, both immediately and over a 2-week period.
Material and Methods
Participants
This was a community sample (N = 40; mean age = 38.63, standard deviation [SD] = 12.99; gender = 11 males [27.50%], 28 females [70.0%], and 1 responded as “nonbinary” [2.50%]). Participants were recruited via social media advertisements and were given the opportunity to opt into a prize draw with a random chance to win one of three gift cards valued at £20 each as a “thank you” for participation. All participants gave informed consent before entering the study. The study was reviewed and approved by an Ethics Committee.
Measures
State rumination
The Brief State Rumination Inventory is a psychometrically valid measure sensitive to situational changes in rumination (Marchetti, Mor, Chiorri, & Koster, 2018). The scale has eight items (e.g., “right now, it is hard for me to shut off negative thoughts about myself”). Participants indicate their response on a visual analogue scale, ranging from 0 (completely disagree) to 100 (completely agree). Participants’ scores are summed to give an overall score. The internal consistency (α) in the present sample was good at baseline (α = 0.83).
Depressive symptoms
We used the Patient Health Questionnaire (PHQ-8) (Kroenke et al., 2009) in the current study, a well-validated eight-item self-report instrument that assesses current symptoms of depression over the past 2 weeks and is based on Diagnostic and Statistical Manual of Mental Disorders IV (DSM-IV) criteria for major depression. The PHQ-8 compares well with the original PHQ-9 (Wu et al., 2020). The α in the present sample was good at baseline (α = 0.77).
Well-being
The Warwick Edinburgh Mental Well-Being Scale (WEMWBS) is a well-validated measure of well-being (Clarke et al., 2011) and sensitive to change in mental well-being interventions (Shah, Cader, Andrews, McCabe, & Stewart-Brown, 2021). We used the short seven-item version (SWEMWBS) in the present study (Ng Fat, Scholes, Boniface, Mindell, & Stewart-Brown, 2017). The scale asks participants to reflect over the past 2 weeks (e.g., “I have been feeling optimistic about the future”). Higher scores indicate higher well-being. The α in the present sample was good at baseline (α = 0.78).
Affect
The Positive and Negative Affect Schedule Short Form (I-PANAS-SF) is a 10-item scale measuring state positive affect (Pos) and negative affect (Neg) using a 5-point Likert scale (1 = “not at all/very slightly” to 5 = “extremely”) (Thompson, 2007). Participants are asked to reflect on how strongly they feel each item at the moment (e.g., “determined,” “nervous”). The I-PANAS-SF has good psychometric qualities, including convergent validity and internal reliability (Thompson, 2007). In the current study, α was acceptable but low at baseline, Pos α = 0.61, Neg α = 0.68.
Mindfulness
The Toronto Mindfulness Scale (Lau et al., 2006) is a 13-item self-report measure tapping into two dimensions; mindful decentering (e.g., “I experienced myself as separate from my changing thoughts and feelings,” and mindful curiosity (e.g., “I was curious about each of the thoughts and feelings that I was having”). This scale has been found to have good construct validity (Lau et al., 2006). The α in the present sample was good at baseline for the curiosity (α = 0.90) and decentering (α = 0.78) subscales.
Self-compassion
The Self-Compassion Scale (short form) is a six-item measure to assess state self-compassion. Three items in the scale measure negative components (e.g., “I feel intolerant and impatient toward myself”) and three measure positive components (e.g., “I’m keeping things in perspective”). Participants indicate how well each statement describes how they are feeling “right now” using a 5-point Likert scale ranging from 1 (“Not at all true for me”) to 5 (“Very true for me”). Three items (which characterized isolation, overidentification, and judgment) were reverse-coded. Scores are derived by calculating a single mean and higher scores indicate greater state self-compassion. This short version has been found to be strongly correlated with its longer counterpart and has adequate internal consistency (Neff, Tóth-Király, Knox, Kuchar, & Davidson, 2021). The α in the present sample was low at baseline (α = 0.61).
Nature connection
The Nature Relatedness Scale (NR6) is a six-item measure that evaluates one’s relationship and connectedness to nature. Participants are asked to rate the strength of their agreement (1 = “strongly disagree” to 5 = “strongly agree”) with statements on nature relatedness. Example items include, “My ideal vacation spot would be a remote, wilderness area” and “I feel very connected to all living things and the earth”). It has been found to have good internal consistency and can reliably predict happiness and nature contact (Nisbet & Zelenski, 2013). The average of each participant’s score is taken, with higher scores indicating strong nature relatedness. The α in the present sample was good at baseline (α = 0.88).
Interventions
The nature-based GI was designed and recorded by a clinical psychologist and designed to be listened to independently. Audio files were created to facilitate independent listening via a portable device with headphones.
Nature-based GI
The GI was informed by a number of clinical and theoretical frameworks and grounded in principles of mental imagery. Primarily, it was designed to tap into our proclivity toward nature or biophilia (Wilson, 1984). Specifically, the aim was to facilitate a connection to nature (Pritchard, Richardson, Sheffield, & McEwan, 2020), affect stress reduction (Ulrich et al., 1991), and attention restoration through “soft fascination” (Kaplan, 1995), and to instill a sense of appreciation of the beauty (e.g., fractal patterns; Hägerhäll et al., 2015) or even awe of nature (Løvoll & Sæther, 2022) through imagery. Consistent with principles of Shinrin Yoku, or forest bathing, (Morita et al., 2007), participants were asked to be open to imagining sights, sounds, smells, and touch sensations, as well as accepting of any emotions that may arise. The present GI also draws on mindfulness principles (Kabat-Zinn, 2003) by encouraging participants to pay attention to their current mental representations, be aware of mental phenomena, and curious awareness. Finally, the GI was informed by approaches that make use of spirituality and the sense of being part of something bigger than oneself, that is, eliciting transcendent experiences (Bethelmy & Corraliza, 2019). The logic of this approach is to combine elements that are known or likely to improve mental well-being. The GI condition took place indoors in a spacious, quiet, private room in the university (see Fig. 1) and participants listened to the script (see Supplementary material) in small groups of up to three people.

Locations of the two interventions: GI and Meditation.
The nature-based meditation condition
We used a 20-min NBM that has been shown to be effective relative to attention control in a single previous study (Owens & Bunce, 2022a). The meditation is underpinned by key theories and approaches used in clinical psychology; mindfulness, compassion-focused therapy, and forest bathing. The NBM condition took place outdoors in a quasi-natural space at the university, between June and August (Northern hemisphere; see Fig. 1), with all three NBM sessions occurring in the same place. The participants listened to the script in groups of up to three people.
Procedure
Participants were allocated to condition using a 1:1 randomization list generated by sealedenvelope.com. Prior to each session, participants were emailed links for the questionnaires, with directions to only fill them out after further instructions once they arrived on site. They were also sent a copy of the audio recording of their allocated condition. Participants first completed the baseline questionnaire (T0) and then participated in their randomly allocated condition, followed immediately by self-report assessments (T1). Approximately 1 week later (mean = 8.94 days, SD = 4.40), participants first repeated the intervention and then the assessment (T2). Approximately 2 weeks from T0 (mean = 17.21 days, SD = 6.75), the participants repeated the intervention and then the assessment for the third and final time (T3). The duration of each session lasted approximately 30 min. Sessions involved one to three participants at a time, depending on their availability. Prior to starting the intervention, participants were given the opportunity to ask questions about the intervention, with regard to general information on nature-based interventions and meditation. Participants were encouraged to practice at least three times between sessions.
Statistical analysis
This is an initial proof-of-principle test of the GI intervention and so we were primarily interested in whether it would perform similarly to a comparable intervention (the NBM). We hypothesized that the effect for GI would be similar to the NBM. Our sample size calculation in G*Power was based on detecting a difference between conditions, should one exist, on any of the outcome measures. Given the expected similarity between the two active interventions, we reasoned that only a large effect size (Cohen’s d = 0.8) between conditions would be worth detecting in this preliminary study. To have 80% power to detect such a difference at the 0.05 level of significance required a total of 40 participants. In the end, a total of 40 participants were randomized to one of the two interventions.
We used STATA (version 17) for analysis and tested baseline differences between the conditions using Analysis of Variance (ANOVA) for continuous data and chi-square tests of association for categorial data. Mixed models were used to assess the effect of time for both groups jointly on the outcome measures. We used Stata’s mixed command with robust standard errors and maximum likelihood estimation in conjunction with the contrast command. Models were specified with a random effect for the individual (id) and we tested the effect of time. We tested for both linear and quadratic change and follow-up tests identified at which timepoints, if any, change was seen on the outcome measures, relative to baseline (T0). Parameter estimates are reported with 95% confidence intervals (CIs). We also tested the Group × Time interaction to see if in this preliminary data there was any evidence of difference over time between the conditions. We used the plotly package in R to illustrate the change over time in figures. Error bars refer to 1 ± standard error (SE) of the mean.
Results
Forty participants were randomized 1:1 to one of the two conditions (GI, n = 20, and Meditation, n = 20) and six were lost to follow-up at T2 (five in the imagery condition and one in the meditation condition), giving an 85% retention rate. We first tested for differences between randomization conditions baseline measures and found none, suggesting that randomization was successful (see Table 1).
Means, Standard Deviations of Baseline Characteristics and Study Measures.
Note. p-values refer to differences between conditions. Tests used were ANOVA for continuous data and χ2 tests of association for categorical data. Hedge’s g refers to the difference between T0 and T3 for all measures.
Means, standard deviations, and proportions of baseline characteristics and study measures.
BSRI, Brief State Rumination Inventory; CUR, curiosity; DEC, decentering; GI, guided imagery; NR6, Nature Relatedness Scale; PANAS NEG, Positive and Negative Affect Schedule negative affect; PANAS POS, Positive and Negative Affect Schedule positive affect; PHQ-8, Patient Health Questionnaire; SD, standard deviation; SSC, Self-Compassion Scale; WEMWBS, Warwick Edinburgh Mental Well-Being Scale.
Rumination
There was a significant effect of time for rumination (χ2 = 49.50, p < 0.0001) and no Group × Time interaction (χ2 = 1.27, p = 0.74). The linear model was the best fit to the data (χ2 = 24.53, p < 0.0001) but the quadratic model was also a significant fit (χ2 = 9.83, p < 0.01). Post hoc contrasts showed a significant decrease in rumination immediately after the intervention (T1) (B = −119.55, SE = 19.84, p < 0.0001, 95% CI = −158.43 to −80.67), at T2 (B = −116.41, SE = 22.36, p < 0.0001, 95% CI = −160.23 to −72.59), and at T3 (B = −148.94, SE = 26.27, p < 0.0001, 95% CI = −200.42 to −97.45).
Self-compassion
For state self-compassion, only the linear model was a good fit to the data (χ2 = 13.68, p < 0.0001) and there was a significant effect of time (χ2 = 34.36, p < 0.0001) and no Group
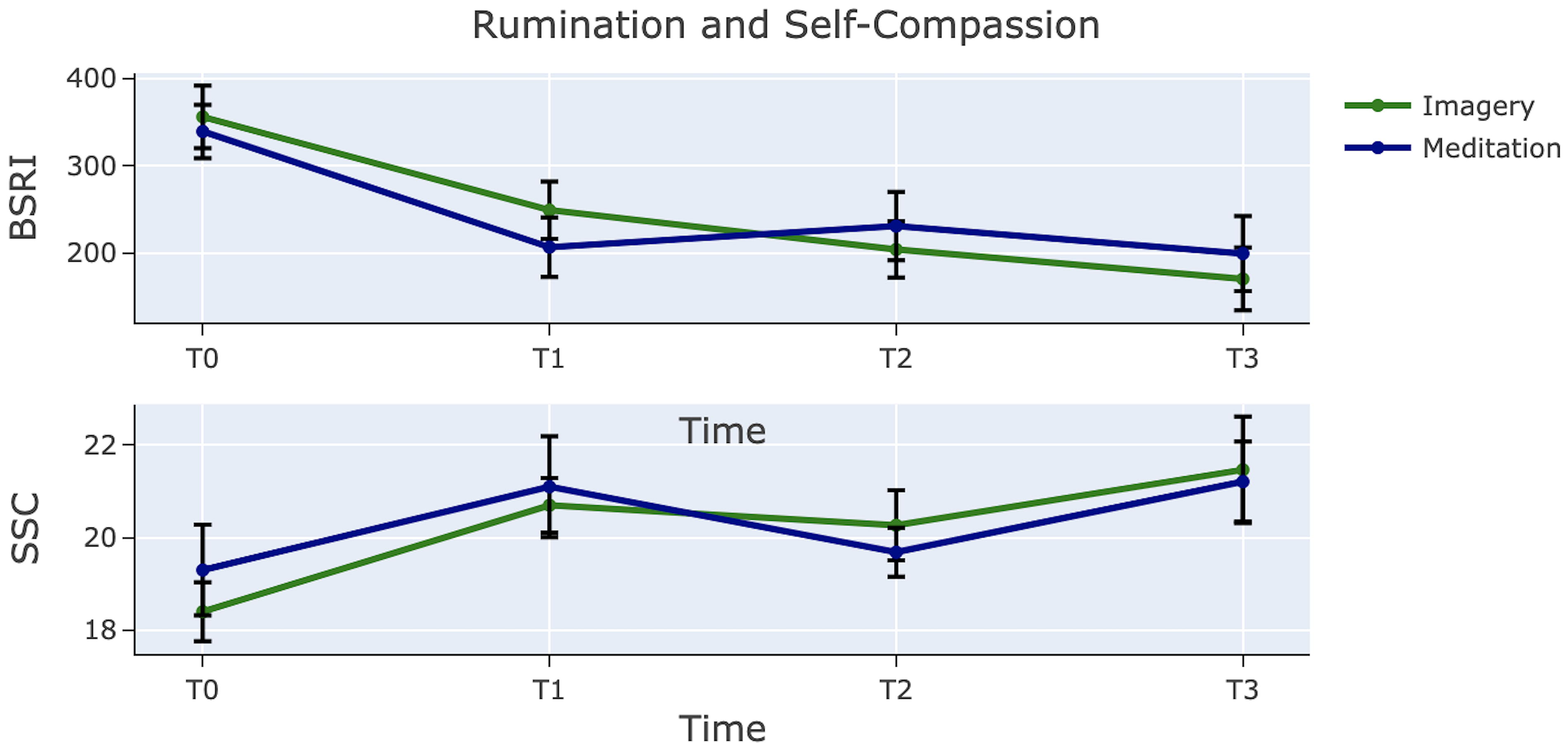
Mean change of rumination and self-compassion by condition. Error bars refer to 1 ± SE of the mean. SE, standard error.
Positive and negative affect
There was a significant effect of time (χ2 = 33.92, p < 0.0001) and no Group × Time interaction (χ2 = 6.59, p = 0.09) for negative affect. The linear model was the best fit to the data (χ2 = 25.47, p < 0.0001) with some weaker evidence also for the quadratic model (χ2 = 4.32, p < 0.05). Post hoc contrasts indicated a significant decrease in negative affect over time relative to baseline: at T1 (B = −0.25, SE = 0.05, p < 0.0001, 95% CI = −0.35 to −0.15), at T2 (B = −0.29, SE = 0.07, p < 0.0001, 95% CI = 0.09 to −0.16), and T3 (B = −0.39, SE = 0.07, p < 0.0001, 95% CI = −0.54 to −0.25).
There was neither a significant effect of time (χ2 = 7.26, p = 0.06) nor a Group × Time interaction (χ2 = 0.48, p = 0.92) for positive affect (see Fig. 3).

Mean change in affect by condition. Error bars refer to 1 ± SE of the mean.
Nature relatedness
There was a significant effect of time (χ2 = 10.63, p < 0.05) and no Group × Time interaction (χ2 = 1.40, p = 0.70) on the NR6. Only the quadratic model was a significant fit to the data (χ2 = 3.57, p = 0.05). Post hoc contrasts indicated a significant increase in nature relatedness at T1 (B = 0.16, SE = 0.05, p < 0.01, 95% CI = 0.06–0.27), none at T2 (B = 0.10, SE = 0.06, p = 0.09, 95% CI = −0.01 to 0.22), and an increase at T3 (B = 0.14, SE = 0.07, p < 0.05, 95% CI = 0.01–0.27). See Figure 3.
Mindfulness
There was a significant effect of time for curiosity (χ2 = 21.11, p < 0.001) and no Group × Time interaction (χ2 = 3.36, p = 0.33). Neither linear (χ2 = 0.05, p = 0.92) nor quadratic (χ2 = 0.39, p = 0.53) models fit the data very well. Post hoc contrasts indicated a significant increase in curiosity from baseline only at T1 (B = 2.75, SE = 0.78, p < 0.0001, 95% CI = 1.27–4.23) and not at T2 (B = −.56, SE = 1.22, p = 0.65, 95% CI = −2.95 to 1.84) or T3 (B = 1.34, SE = 0.90, p = 0.14, 95% CI = −0.42 to 3.11).
For decentering, there was a significant effect of time (χ2 = 35.97, p < 0.0001) and no Group × Time interaction (χ2 = 5.63, p = 0.13). Linear (χ2 = 3.57, p = 0.05) and quadratic (χ2 = 3.57, p = 0.05) models were reasonable fits to the data. Follow-up tests indicated that there was a significant increase in decentering from baseline at T1 (B = 4.40, SE = 0.81, p < 0.0001, 95% CI = 2.81–5.99), no difference at T2 (B = 1.65, SE = 1.07, p = 0.12, 95% CI = −0.44 to 3.74), and an increase at T3 (B = 3.28, SE = 0.90, p < 0.0001, 95% CI = 1.51–5.05). See Figure 4.
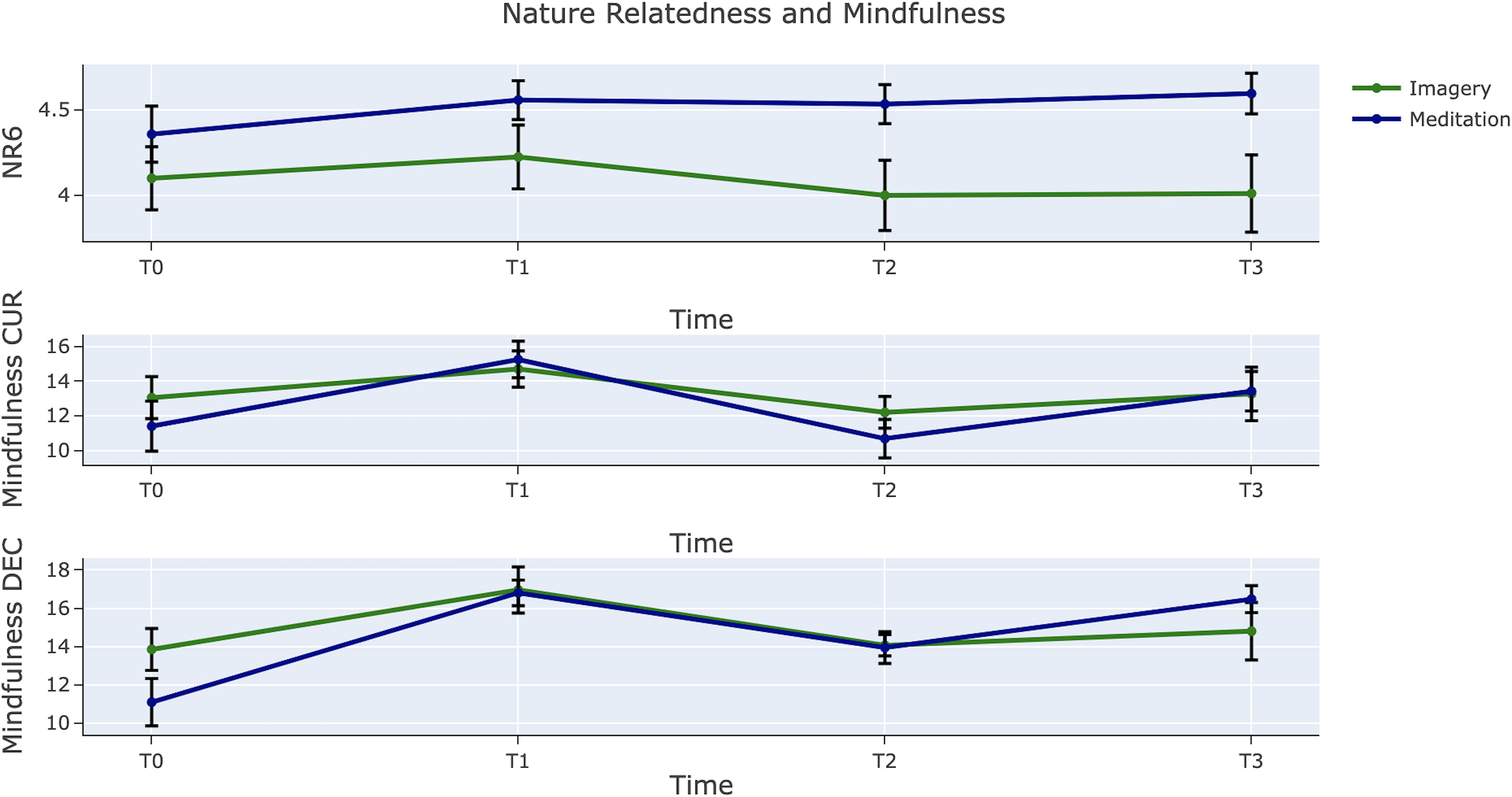
Mean change in nature relatedness and mindfulness by condition. Error bars refer to 1 ± SE of the mean.
Mental well-being
There was a significant effect of time for depressive symptoms (χ2 = 15.11, p < 0.001) and no Group × Time interaction (χ2 = 1.66, p = 0.44). Linear growth provided a good fit to the data (χ2 = 15.11, p < 0.001) and there was no evidence for the quadratic model (χ2 = 0.00, p = 0.95). Post hoc contrasts suggested a significant decrease in symptoms at T2 (B = −0.87, SE = 0.35, p < 0.05, 95% CI = −1.55 to −0.19) and at T3 (B = −1.33, SE = 0.35, p < 0.001, 95% CI = −2.01 to −0.65).
Well-being significantly increased over time (χ2 = 25.47, p < 0.0001) and there was no Group × Time interaction (χ2 = 2.23, p = 0.33). Both linear (χ2 = 16.34, p < 0.001) and quadratic (χ2 = 5.12, p < 0.05) models provided a good fit to the data. Post hoc contrasts showed that the increase in well-being was seen at T3 (B = 1.86, SE = 0.411, p < 0.0001, 95% CI = 1.05–2.66) but not at T2 (B = 0.45, SE = 0.44, p = 0.31, 95% CI = −0.42 to 1.31). See Figure 5 for an illustration of this effect.

Mean change in depressive symptoms and well-being. Error bars refer to 1 ± SE of the mean.
Discussion
The present study included a community sample of adults and the results provide preliminary empirical evidence to support the further development of novel nature-based interventions in the support of mental well-being. We developed a new GI intervention, tested indoors in this study, and tested a guided meditation that was used outdoors in a quasi-natural setting. The evidence suggests that the effect of GI was similar to the meditation in terms of outcomes, both immediately and over a 2-week period. It is important to note that the NBM has been shown to be superior to an attentional control in a previous study (Owens & Bunce, 2022a) and so the present study also represents a partial replication of that study. The current findings are consistent with and extend previous work on guided nature-based imagery. Similar to previous work (Coughlan et al., 2022), we found evidence for increases in nature connection immediately after the GI. However, continued improvement over after time points may have been driven mostly by the NBM condition, which may suggest that it is important to include real-world exposure to natural environments in an intervention package, to increase sustained connection to nature. Certainly, there is evidence that in other “virtual” exposure contexts, effects on well-being may be weaker when compared with real-world settings (Browning et al., 2020). Although there was no Group × Time interaction detected, it is possible that in a larger replication study differences between the groups on nature connection will appear. Although we did not explicitly measure relaxation in the present study, the results are also consistent with the pattern of results in a previous study that suggested that nature GI increased levels of relaxation when compared with urban and built environment GI (Koivisto & Grassini, 2022). We found reductions in negative affect over the study period but no overall change in positive affect. Similarly, a prior nature-based GI study found reductions in state anxiety after two sessions, 1 week apart (Nguyen & Brymer, 2018). The absence of change in positive affect may represent a power issue in this study and may be explained to some extent by the particularly low reliability on the PANAS positive subscale. It is also possible that the intensity of the intervention may have been too low to produce effects on positive affect. For example, in comparison a more intense, 6-week NBI based in wetlands in the United Kingdom found improvements in well-being, anxiety, stress, and negative as well as positive affect (Maund et al., 2019).
Consistent with related nature-based intervention research, we found change over time in our clinically relevant outcome measures. For example, in an 8-week MBSR study carried out in different locations (nature, urban, and indoor), Choe et al. (2020) found improvements in mindfulness in all conditions and specific positive change in the nature condition for nature connection, stress, and rumination. In the present study, we also saw reductions in rumination, as have other nature-based intervention studies (Lopes, Lima, & Silva, 2020; Owens & Bunce, 2022a). Also consistent with previous research on imagery and rumination, our findings concur with others who suggest that imagery-based distraction may be helpful in reducing the cognitive resources available for maladaptive rumination, whether image-based or verbal in nature (Iyadurai, Hales, Blackwell, Young, & Holmes, 2020; Lawrence et al., 2023). We recognize, however, that mindfulness approaches that are absent an aspect of nature are also effective for reducing psychological distress (Liebmann, Konrad, Singer, & Kanske, 2023) and depressive rumination (Perestelo-Perez, Barraca, Peñate, Rivero-Santana, & Alvarez-Perez, 2017). Depressive rumination is a key driver for the development and maintenance of depression (Watkins & Roberts, 2020) and brief interventions to reduce state and trait rumination may be useful in both treating clinical populations and preventing the onset of problems in community samples (Topper, Emmelkamp, Watkins, & Ehring, 2017).
We also found improvements on self-compassion which has been shown to prospectively predict depressive symptoms in community samples (Raes, 2011). Interestingly, in the present brief interventions, we found effect sizes on improvements in self-compassion equivalent to interventions designed specifically to increase self-compassion (Kirby, Tellegen, & Steindl, 2017), some of which are considerably longer in duration than the present interventions (Wallmark, Safarzadeh, Daukantaitė, & Maddux, 2013). Mindfulness facets also improved after the nature-based interventions, which have been reported in other studies. For example, a 30-day intervention that encouraged daily exposure to nature environments reported increases in mindfulness and well-being (Hamann & Ivtzan, 2017). However, it is important to note that this effect on mindfulness was only seen in “wilderness” and not in “urban greenspace,” again suggesting that natural, and perhaps wild, spaces may have particular utility in improving well-being. In the present study, there was a suggestion of a stronger effect for the decentering facet versus curiosity. There is preliminary evidence for the centrality of decentering in the nature-well-being nexus in cross-sectional data (Sanyer, Bettmann, Anstadt, Ganesh, & Hanley, 2022) and future work should test this further, experimentally.
Although this study was not a clinical trial, two directly interpretable clinical measures included were the PHQ, measuring depressive symptoms and the SWEMWBS, and an index of mental well-being. The current sample had low levels of depressive symptoms at baseline but nevertheless, these were reduced in both the GI and NBM groups, by 1.25 and 1.08 points, respectively, before the study end. In both cases, this represents a drop of ∼20%, an approximate minimal clinically important difference (MCID) estimate for the PHQ (Kounali et al., 2022). It should be noted here that in community samples with low symptom levels, improvements in symptoms in real terms will be limited. Similarly, well-being increased by 2 points on the SWEMWBS in the GI group and 1.4 points in the NBM group, consistent with an MCID of 1–3 points (Shah, Cader, Andrews, Wijesekera, & Stewart-Brown, 2018). It is therefore possible that these interventions could improve clinical outcomes for patients but research with these populations is needed before making any recommendations.
While no conclusions for clinical effectiveness on treating or preventing mental disorders can be drawn from the data in the present study, a number of ideas could be tested in the future. For example, given this sample featured participants with low levels of depressive symptoms at baseline, the interventions could be tested in a prevention context in future studies, offering simple and cost-effective resources to reduce depressive symptoms and increase well-being. We recognize, however, that future replication and extension studies are needed to verify the present preliminary findings. There are a number of possibilities for the use of such developed interventions in clinical practice. The interventions may be used to supplement more intensive therapeutic interventions as home practice activities. They facilitate access to nature-based interventions, especially the GI intervention, which does not require any access to outside space. Practitioners may choose to offer GI for those with a preference for imagery and/or those who also may be restricted physically and/or have visual impairment. GI may also have better applicability for people who find traditional mindfulness practice challenging or too abstract. Alternatively, practitioners may suggest the NBM to increase nature connection for people, if in alignment with their therapeutic goals. The NBM could also be used in a graded exposure approach, early on in therapy to support people to begin to gently access nature and can be easily used in any nature context such as quasi-nature, for example, one’s garden, or a public park, through to more wild settings. It can also be used in green and blue spaces according to individual preference. Both interventions could be used as standalone strategies to increase self-compassion, which is important in managing repetitive negative thinking (Schlosser, Jones, Demnitz-King, & Marchant, 2022) and is associated more broadly with positive mental health (Bluth & Neff, 2018). The trajectory of effects shown in this study is useful for practitioners to hold in mind when advising people on the experiences of engaging in these interventions; there may well be a downturn in negative symptoms before an increase. This may support people to have a realistic understanding of the intervention and can be built into initial psychoeducation. The utility of these approaches should be tested in future research.
Strengths and limitations and future directions
This study has several strengths with participants being randomized to condition, good retention rate, comparison of GI with an appropriate active nature-based condition, and the use of well-validated outcome measures. A main limitation of the present study is that we did not measure individual differences in the ability to employ visual imagery which may have affected the results. It may be the case that effects on outcome are moderated by such individual differences and this should be tested in future work. In addition, some psychometric instruments showed relatively weak reliability in this sample which may have affected the results. On balance, this is not very likely, however, given that the measures have been well-validated in other samples. The sample size is limited but appropriate for a proof-of-principle study. The study was also limited to a community sample and it was beyond the scope of the present undertaking to ascertain whether or not participants had histories of mental or physical health diagnoses and level of service use. However, the low level of depressive symptoms suggests that this was not on average a sample that could be characterized as clinical in nature. Future studies should test the effect of nature-based GI and meditation in clinical trials, for example with those with mild-to-moderate depressive symptoms or patients living with clinical depression. It will also be important to test the acceptability of the interventions in future studies. Moreover, future work should focus on bringing together elements that have been shown to be effective in improving mental well-being, such as meditation and GI, into intervention packages that are appropriate for those who are likely to benefit from nature-based approaches. This may be important for both self-help interventions and therapeutic approaches for people who present to mental health services.
Conclusion
This experimental study provides preliminary evidence for the future development of nature-based GI and meditation as interventions to improve mental well-being. While the results of the present study broadly suggest similarities in the outcomes, it might be that differences emerge in different contexts and populations. This could be tested in future studies.
Footnotes
Acknowledgment
We thank the people who gave up their time to participate in the study. Without such volunteers, this research would not be possible.
Authors’ Contributions
M.O.: Conceptualization, data curation, formal analysis, investigation, methodology, resources, visualization, and writing—original draft. H.B.: Conceptualization, visualization, supervision, and writing—reviewing and editing. R.L.: Conceptualization, data curation, investigation, and writing—reviewing and editing.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author Disclosure Statement
All authors declare no competing interests.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.