
Abstract
Many veterans struggle with their mental health, and wilderness therapies offer promising unconventional approaches that improve psychological symptoms. However, less is known about broader psychosocial benefits, such as post-trip attitudes toward treatment and mental health or the degree and longevity of related improvements in social connection, coping, and life skills. Our study investigated whether veterans who had undergone a 3-day wilderness therapy program during the preceding 2 years would report relatively high treatment-seeking willingness, sense of social connection, and improvement in and continued use of coping and life skills. Among 28 participants from the 2 prior years of the Huts for Vets wilderness therapy program, the veterans reported high openness to a range of further treatment options, including one-on-one therapy, group therapy, and therapies with other veterans. They also reported improved social connection and strong coping strategy continuance and benefits. Open-ended responses supported these findings, with veterans reporting increased feelings of camaraderie, improved confidence and self-perception, and help-seeking willingness. These results extend previous findings and suggest the potential for the spreading activation of wilderness therapy benefits for veterans.
Service members exposed to combat deployments experience high rates of psychological and emotional difficulties, such as depression, anxiety, and post-traumatic stress disorder (PTSD), as well as broader psychosocial struggles, including social isolation (Bird, 2015; Gelkopf et al., 2013; Shorer et al., 2023). Unfortunately, many veterans report a range of stigma beliefs about mental illness that may interfere with their openness to seeking psychological treatments for these problems (Brown and Bruce, 2016; Bryan and Morrow, 2011; Hoge et al., 2004; Stecker et al., 2013). Wilderness, outdoor, and adventure therapies may offer a more acceptable means of psychological treatment for veterans with many of the benefits of traditional therapies, as well as additional benefits specific to the therapy medium (Forsyth et al., 2020). However, their longer-term impact on broader psychosocial outcomes, such as openness to future treatment, social connection, and coping skills, is not yet known.
Wilderness therapies are group programs providing outdoor experiences to engage individuals in mental health treatment (Gass et al., 2020). There is a broad array of outdoor group programs, such as wilderness therapy, adventure therapy, outdoor leisure programs, nature interventions, and other nature-based therapies, offered in a variety of nature/wilderness settings with a range of activities, such as hiking, backpacking, kayaking, white-water rafting, and rock climbing (Bettmann et al., 2020, 2022; Gass et al., 2020; Harper et al., 2014). Program frequency and duration vary widely, from day trips to overnight trips of a few days to a week or more to multiple weekly adventure sessions over the course of a year (Bird, 2015; Duvall and Kaplan, 2014; Gelkopf et al., 2013). A meta-analysis by Bowen and Neill (2013) identified several key therapeutic components believed to contribute to the effectiveness of wilderness therapies. Among these were interaction with nature, creation of eustress through positive heightened arousal, meaningful engagement in outdoor experiences, a focus on positive change, and group processes that contribute to improved psychosocial outcomes.
A meta-analysis by Greer and Vin-Raviv (2019) and a growing body of research highlight the effectiveness of wilderness therapies in producing psychological benefits, including reduced anxiety, depression, and PTSD among veteran populations (Davis-Berman et al., 2018; Duvall and Kaplan, 2014; Shorer et al., 2023). Vella et al. (2023) researched the efficacy of a 3.5-day Huts for Vets (HFV) program, including wilderness hikes, philosophical and psychological readings and discussions, and instruction in coping practices (e.g., mindfulness, yoga, Qigong) and life skills (e.g., cooking, cleaning). After the HFV wilderness trip, the 32 program participants reported significant decreases in anxiety, depression, PTSD, and somatic stress symptoms immediately after the program and at the 6-week follow-up.
While the immediate psychological benefits of wilderness therapy are well documented, some veterans continue to experience adjustment difficulties or symptom relapses, making openness to other forms of treatment particularly important. To date, only two studies have examined veteran willingness to seek professional psychological services after wilderness therapy, and they have had somewhat mixed but promising findings. Bettmann et al. (2020) found that after a 6-day adventure trip, veterans reported improved professional treatment-seeking willingness from pretrip to 1-month post-trip. Another study by Bettmann et al. (2023) reported that after a 3-day adventure trip, veterans’ willingness to seek professional psychological help did not change significantly from pre- to post-trip but was significantly higher at 1-year post-trip. These studies are an important first step in understanding veteran openness to treatment after wilderness therapy programs and should be expanded to include a broader scope of mental health treatment openness and attitudes. For example, are veterans more open to other veteran group treatments and other wilderness experiences, and what are their attitudes toward mental health and speaking about their mental health with others after wilderness therapy programs?
Increased openness to treatment could help veterans engage with other therapeutic approaches and seek additional support, perhaps improving their ability to build trust and form meaningful relationships, which is another significant struggle for veterans. The loss of the community that military service provided can lead to feelings of isolation, which contributes to mental health decline (Wesselmann et al., 2018). Wilderness therapy may offer gains both through immediate social connections and improved post-treatment social functioning. A meta-analysis by Bowen and Neill (2013) found that adventure therapy participants reported improved capacity to interact within social situations across 206 studies. Recent studies with veterans have expanded upon this, finding increased reported feelings of camaraderie, sense of belonging, and social quality of life immediately after and up to 12 months after participating in wilderness programs (Bird, 2015; Gelkopf et al., 2013; Harper et al., 2014). To our knowledge, no studies have examined social connection for wilderness therapy participants beyond 12 months post-treatment nor have these issues been examined qualitatively.
Another potential long-term benefit of wilderness therapy programs may be improved coping and life skills and their continued use. Wilderness therapy activities have been shown to effectively teach coping skills that veterans can apply when facing everyday challenges (Gass et al., 2020; Gelkopf et al., 2013). For example, in the HFV program, veterans are taught yoga, mindfulness, Qigong, cooking, and nutrition while on their trip. Veterans can continue to use these skills and knowledge in their home environment, which may contribute to maintaining treatment gains. Given promising findings of decreased psychopathology symptoms up to 6 weeks post-trip (e.g., Vella et al., 2023), it seems likely that coping strategy and life skill use are contributors to these benefits, but this has not yet been examined.
Current Research
The current study hypothesized that veterans who participated in a wilderness therapy trip with the HFV program during the preceding 2 years would report: (1) improved openness to a range of mental health treatment options and positive attitudes toward and openness about mental health; (2) longer-term enhanced sense of social connection in general and with the veteran community; and (3) use of and benefits from the coping and life skills they learned during the trip, such as yoga or mindfulness.
Method
Participants
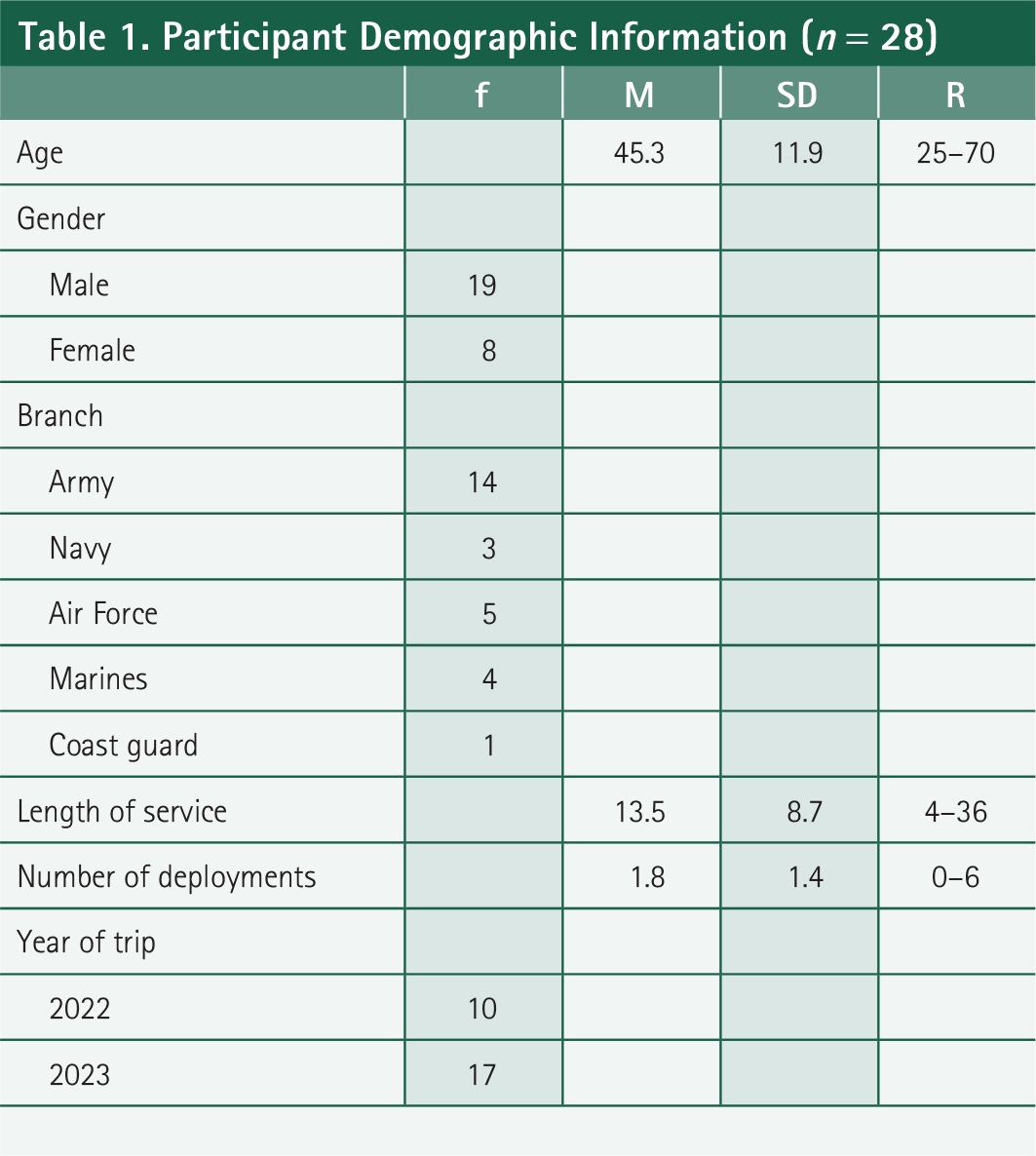
The participants for the current study (demographic information shown in Table 1) included 28 veterans (Mage = 45.3, SD = 11.9; 19 men and 9 women) who participated in a 3.5-day outdoor wilderness therapy program through HFV in Aspen, Colorado, during the summer of 2022 or 2023. A majority served in the Army (50%), and participants had an average service length of 13.5 years and an average of 1.8 deployments. Of the 28 veterans who participated, 10 were from the summer 2022 programs, 17 were from the summer 2023 programs, and 1 did not report trip year.
Participant Demographic Information (n = 28)
Recruitment for the current study consisted of an email containing an anonymous survey link administered through Qualtrics and sent out to HFV participants from the previous 2 years. All participants viewed a consent waiver at the beginning of the survey, and continuation to the survey represented consent. The survey took approximately 15–20 min to complete. Data collection occurred from January to March of 2024. The recruitment email was sent to 84 veterans who participated in the HFV wilderness program in the summer of 2022 or 2023. This study was approved by the internal review board for Florida Atlantic University.
Intervention
During their 3.5-day wilderness therapy program, HFV takes approximately 10–12 veterans per trip to stay in mountain huts in Aspen, Colorado, between June and September. There are licensed mental health coaches and wilderness guides on the trips. There are all-male, all-female, and coed trips. Veterans participate in hikes up to an elevation of 11,300 feet and across 6.5 miles.
Veterans engage in 4–5 discussions based on assigned readings pertaining to philosophy, psychology, and the wilderness. Program leaders select readings for discussion from a larger set, which varies somewhat depending on group composition (e.g., all-male trip readings include more male authors, and all-female trip readings include more female authors) and issues of the group members and may be adjusted depending on how discussions are progressing. Readings include Indian Wisdom by Chief Luther Standing Bear, The Road Less Traveled by Robert Frost, Green Exercise: A Walk in the Woods by John Schwartzberg, Veteran Expeditions to Wilderness by Stacy Bare, St. Crispin’s Day Speech by William Shakespeare, The Tragic Blessing of Combat Veterans by Auden Schendler, Sixteen by Tao Te Ching, Solitude by Henry David Thoreau, Learning to Let Go by Kayla Williams, Fight Like a Girl by Kate Germano and Kelly Kennedy, selections from Man’s Search for Meaning by Viktor Frankl, and others.
During trips, a mental health coach teaches mindfulness through breathing techniques and guided meditation, typically lasting 45 min per session, and also practiced during 1 h of solo time in nature. Participants learn yoga from the mental health coach, which is practiced twice for 45–60 min. Veterans also learn Qigong, which is led by the group leader and is typically practiced twice for 30 min. Additionally, participants learn life skills by helping in the kitchen, preparing meals, washing dishes, chopping wood, starting a fire, and/or cleaning the hut.
Study design and survey design
The current study represents a mixed-methods retrospective design with quantitative and qualitative measures of HFV wilderness therapy program outcomes. Veteran- and program-specific survey items were designed to adequately capture HFV program outcomes specifically. Survey brevity, simplicity, and valence neutrality were prioritized to minimize participant fatigue, attrition, and distress. Thus, we selected a small number of items from standardized measures to assess psychological distress and well-being. We developed brief, veteran-specific, and program-specific assessments of openness to treatment, mental health attitudes, and social connection, which overlap and extend item content from a range of other longer measures developed for other populations (e.g., Fischer and Farina, 1995; Kravetz et al., 1985; Mundt et al., 2002; Schuster et al., 1990) and emphasize the areas of focus of the HFV program. Our items evaluating coping and life skill use and benefits and their continued use were focused exclusively on the skills taught during the HFV wilderness program.
Measures
Demographic and military service information
This survey included seven questions regarding demographic and military service information: age, gender, military branch, length of service, number of deployments, period of service, and year of HFV trip.
Psychological distress and well-being
A brief distress index was calculated using three items from the Kessler Psychological Distress scale (Kessler et al., 2002): nervous, restless/fidgety, and that everything was an effort. A well-being index was calculated using four items from the Diener Flourishing Scale (Diener et al., 2010): You actively contributed to the happiness and well-being of others, you are a good person and live a good life, you are optimistic about your future, and you are engaged and interested in daily activities. Participants rated the frequency of their experience of each over the last 30 days using a 5-point Likert scale (1—never, 5—daily). The internal consistency was strong for both the distress and well-being items, α = 0.86 and α = 0.81, respectively.
Openness to treatment and mental health attitudes
Participants rated their agreement with six statements about openness to seeking out further therapy options and feelings toward and discussions of mental health with others (i.e., “I would be open to traditional one-on-one therapy,” “I would be open to group therapy,” “I would be open to therapies with other veterans,” “I would be open to another wilderness trip,” “I know there are positive ways to address mental health,” and “I am more willing to discuss my mental health with others”) using a 5-point Likert scale (1—definitely not open to, 5—would seek out). The internal consistency was strong for the openness to treatment items, α = 0.79.
Social connection
Participants rated their agreement with four social connection statements using a 6-point Likert scale (1—completely disagree, 6—completely agree). The items assessed participants’ feelings about social situations, social connections, and forming relationships with others (i.e., “I have an easier time connecting with people after finishing my HFV trip,” “This trip inspired me to connect with more veterans,” “I feel more comfortable forming relationships after participating in this trip,” and “I feel more comfortable in social settings”). The internal consistency was high for the social connection items, α = 0.91.
Coping benefits and continued use
Continued coping and life skill use and benefits were measured with a series of questions. First, participants rated their agreement using a 6-point Likert scale (1—completely disagree, 6—completely agree) with five items about whether each skill (mindfulness, yoga, Qigong, philosophical readings, and life skills) from the HFV trip was beneficial. Second, in a series of five branching questions, participants indicated whether they had continued to use each skill after their trip with a yes, no, or maybe response. An answer of no led to a question, “Would you continue that skill?” with a yes or no response. An answer of yes to having continued the skill led to two questions rated on a 5-point scale, one regarding the frequency of each skill used (1—a great deal, 5—none) and one regarding its level of usefulness (1—not at all useful, 5—extremely useful). Internal consistency was high for the coping benefit items, α = 0.90, and was adequate for the continued use items, α = 0.71.
Qualitative data
We asked participants five open-ended questions about their experiences participating in the HFV program: “How has your overall view of wellness changed since this trip?” “Do you think this experience has had a positive effect on your life? If yes, how?” “Is there anything that can be improved for the next participants?” “What did you find most helpful during this experience?” and “Did this trip help you find something you felt you were missing? If yes, what?” Participants could type their responses into text boxes.
The researchers used both deductive and inductive approaches to examine the qualitative data, with more emphasis placed on the insights and information to be gained through an inductive approach. The first author reviewed all open-ended responses to identify themes for rater coding, with special attention to responses pertaining to the primary variables of interest in the study (treatment openness, social connection, and use of and benefits from coping and life skills) as well as an open mind for other emerging themes and patterns. This review of the qualitative data led to refinements of the primary variable categories to better reflect the lived experiences of participants. Treatment openness was observed to be part of a broader category of responses involving asking for help and/or making mental health a priority. The theme of social connection was refined to incorporate camaraderie and a sense of connection with fellow veterans. The coping and life skill use and benefits category largely focused on the benefits obtained from the skills. In addition, a notable theme of participants’ improved sense of identity and insight emerged. This category included reports of enhanced self-confidence, sense of purpose, self-compassion, willingness to be vulnerable, and personal insight.
Next, the first author devised definitions of the themes and trained the raters to code participant responses according to the different themes by providing hypothetical sample responses. An advanced undergraduate rater and PhD psychologist independently coded participants’ free responses for the four identified themes: asking for help/making mental health a priority, camaraderie/connecting with fellow veterans, benefits of coping use, and improved identity/insight. These themes were coded as either present or absent for each participant based on their responses to all open-ended questions. For example, the presence of asking for help might include statements about understanding the usefulness of help-seeking, whereas the presence of camaraderie might include statements that participants felt a sense of community or reconnection with others. The raters averaged 81.5% agreement with their ratings across all four themes for all participants. Cohen’s kappa coefficient was calculated to assess rater agreement, revealing a kappa of 0.61 (95% CI: 0.60, 0.62), which indicates substantial agreement beyond chance (Landis and Koch, 1977). The two raters and the first author discussed all coding disagreements and decided on a final coding category by consensus. As an additional check, the first author reviewed the coding of a randomly selected 10% of the sample and was in agreement with 96% of the ratings (the single rating disagreement with a single coder had already been addressed previously in the review of rater disagreements).
Results
Frequency of reported psychosocial improvements
Openness to treatment
After the wilderness therapy trip, the majority of participants reported they are definitely open to or would seek out traditional one-on-one therapy (67.8%) and therapies with veteran groups (64.2%), and a large minority (39.3%) reported they are definitely open to or would seek out group therapy. Further, 92.9% completely or mostly agreed that there are positive ways to address mental health, and 78.5% completely or mostly agreed that they are more willing to discuss their mental health with others.
Social connection
A majority of participants (75.0%) completely or mostly agreed that the HFV program inspired them to connect with more veterans, and many either completely or mostly agreed that they felt more comfortable forming relationships with others (50.0%). A large minority of participants completely or mostly agreed that they felt more comfortable in social settings (42.9%) and had an easier time connecting with other people (35.7%).
Coping benefits and continued use
As shown in Table 2, reflecting back on the skills taught in the HFV program, the vast majority of participants completely or mostly agreed that the mindfulness they learned was beneficial and that the readings from the trip were beneficial. Half completely or mostly agreed that the yoga and life skills were beneficial. A minority (35.7%) completely or mostly agreed that the Qigong was beneficial.
Frequency of Agreement with Coping Benefit and Continued Use Statements
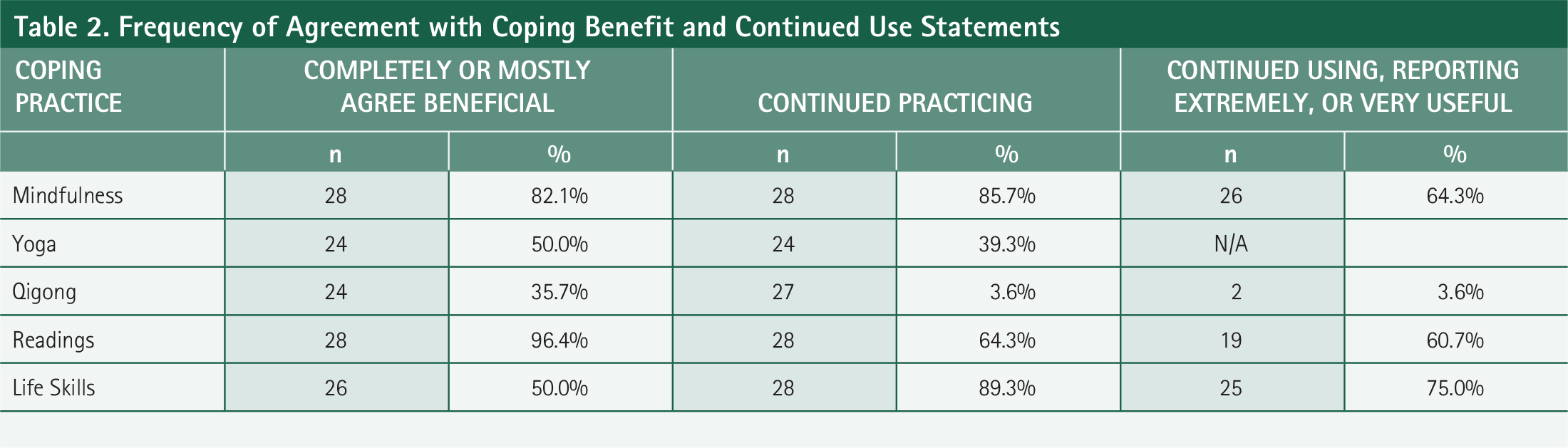
Overall, a large majority continued using the life skills they were taught after returning from the trip and reported that these skills have been either extremely or very useful. Most participants continued practicing mindfulness, with a majority stating that these skills have been extremely or very useful. A minority of respondents have continued practicing yoga. (Due to an error within Qualtrics, the follow-up question about yoga’s benefits for those who have continued was not presented. This is indicated by N/A in the table.) Most have not continued practicing Qigong, and of those who have not continued, a large minority reported that they are not open to continuing that practice.
Relationships between variables
Bivariate correlations were computed to examine the relationships among the primary variables. Normality was assessed using the Shapiro–Wilk test. All variables except coping benefits had p > 0.05, suggesting normality. Since the coping benefits distribution was abnormal, Spearman’s rank correlation test was calculated.
As would be expected, distress and well-being were significantly negatively correlated (r = −0.56, p < 0.012). Continued coping and well-being were also negatively correlated (r = −0.45, p < 0.038), with those reporting less well-being reporting more attempts at coping. Coping benefits were significantly negatively correlated with distress (r = −0.56, p < 0.009), with those reporting the most benefits from their coping practices reporting the least distress. Those reporting the most coping benefits also reported the highest well-being, with coping benefits and well-being significantly positively correlated (r = 0.54, p = < 0.012). Additionally, openness to treatment and distress were strongly positively correlated (r = 0.41, p < 0.034), with veterans reporting the most distress also reporting the most openness to treatment options.
Qualitative analysis
In their open-ended responses, a sizeable minority (33.3%) of veterans wrote about improved psychological knowledge and insight, prioritizing mental health, and/or learning how to ask for help as a result of their HFV trip. For example, some participants described a better understanding of their psychological state. A 52-year-old male said, “This trip helped me realize that internalizing is not healthy,” and another noted that they were “more in touch with actual needs instead of pushing them to the side” (37-year-old male). Other veterans reported managing their health and wellness better. For example, a 35-year-old male stated, “This trip allowed me to understand the depth of my issues and gave me the strength to manage them,” and a 36-year-old female wrote, “I made my mental health a priority and try to get outside every day.” Another participant noted, “I’ve taken a more active role in my physical and mental well-being” (36-year-old female). Others wrote about improved help-seeking and willingness to discuss psychological struggles. A 57-year-old male stated, “I realized I do not have to burden it all. I can ask for help,” and a 37-year-old male wrote, “I learned how to ask for help.”
On average, 55.6% of participants spontaneously mentioned camaraderie or feelings of connection with others. For instance, some participants reported reduced seclusion after the trip. A 36-year-old female reported, “I didn’t feel so isolated afterwards and found it easier to relate to others, especially other veterans.” A 56-year-old female stated, “I noticed the conversations we had inspired me to deepen in conversations with fellow veterans and to consider how I was self-isolating.”
Many participants noted deeper feelings of connection with those who share similar experiences. A 52-year-old male stated, “This trip helped me reaffirm my belief that others have the same feelings and experiences as me, and we can all help each other if we talk with those who understand.” A 57-year-old male wrote, “I found the connections with like-minded people to be the most beneficial part of the trip.” Another wrote, “Even though I know there are others going through what I have, it’s even better talking and getting to know other veterans, put a face on it” (52-year-old male). Connection with fellow veterans was a common theme. One veteran reported experiencing “belonging/brotherhood again. Something I have missed since leaving the military” (56-year-old male). A 63-year-old female reported, “Being more exposed to like-minded female veterans, sharing similar but different stories, relatable. Being vulnerable and open to talk more in-depth about my trauma… The camaraderie between new veterans during the hike was the most beneficial part of the trip. We motivated and encouraged each other to keep going, and if someone needed extra water or a hiking pole, we quickly lent the hand.” Veterans described functional and emotional support. One touted the benefits of “being around other veterans who inspire and encourage me getting out in nature” (55-year-old male). Another veteran noted that the trip had increased his “desire for/engagement in social and supportive interaction with other men” and that “the interaction with other male veterans has helped me be more comfortable with other men” (61-year-old male).
A large majority of participants (70.4%) wrote about the benefits of coping strategies and skills they learned in the program. A 42-year-old female said, “I use the tools and discussions we had on the trip as a daily reminder that it is okay to feel,” and a 56-year-old female reported, “I feel more prepared to take on new challenges.” Another said, “This trip gave me more optimism and tools” (37-year-old male). Some participants identified the trip activities they found beneficial. For example, a 44-year-old male wrote, “I found the mindfulness and learning of nature’s benefit to be the most helpful during this experience.” A 45-year-old male wrote, “Learning how to reconnect with nature and others were valuable skills I learned to use. I have since used them when having really rough days.” Another noted, “The readings inspired a level of intimacy and vulnerability that I am so grateful for reframing my relationship with veterans” (56-year-old female). Another veteran wrote that the trip impacted his life “in a very profound way. I was able to discuss amongst my group a moral injury that I had experienced in combat for the first time since it occurred. I had guilt I had been carrying around for many years” (56-year-old male).
Some participants (37.0%) reported developing increased confidence, self-understanding, and sense of purpose. For instance, a 42-year-old female wrote, “I feel more confident in myself and connected with nature,” and a 61-year-old female reported, “Challenging myself made me realize I can do more than I thought I could.” Another veteran wrote, “It made me so proud that I hiked up that hill. It gave me a sense of peace and revived my confidence” (35-year-old male). One participant stated, “This trip helped me find self-compassion” (35-year-old male). A 37-year-old male wrote, “Realizing my lost sense of purpose was very powerful.”
Some veteran written responses included multiple themes together, interweaving them in meaningful and compelling ways and describing enduring change. For example, one veteran wrote, “I didn’t feel so isolated afterwards and found it easier to relate to others, especially other veterans. I used what I learned and the experience to encourage other veterans to heal which also makes me feel good” (26-year-old female). Another wrote, “I felt an ability to find a true depth of connection and an ability to express all of me compared to the limited me that I felt permission to express in the toxic military culture at times” (56-year-old female).
Discussion
The purpose of this study was to investigate, both quantitatively and qualitatively, the impact of veteran participation in the HFV wilderness therapy program during the preceding 2 years on openness to psychological treatments, mental health attitudes and behaviors, social connection, and the use and benefits of coping and life skills. Findings from existing studies have suggested the benefit of wilderness programs, particularly in decreasing psychopathology symptoms in the short term (Bettmann et al., 2022, 2023; Duvall and Kaplan, 2014; Forsyth et al., 2020; Scheinfeld et al., 2017; Vella et al., 2013, 2023). Less is known about the broader psychosocial outcomes, particularly more than 6 months after wilderness therapy.
Perhaps most importantly, our first hypothesis was confirmed, and our results indicate that between 6 and 21 months after participation (10 of our participants were approximately 21 months out) in the 3.5-day HFV wilderness therapy program, the majority of veterans report being open to a range of therapy options. These included traditional one-on-one therapy and therapies with other veterans, with many reporting they would seek these programs out on their own. In addition, our qualitative data indicate improvement in help-seeking willingness, with veterans describing this in their own words. Given the notoriously low rates of treatment-seeking in the veteran population at large and the stigma and skepticism associated with traditional therapy by many in the military, these results are particularly promising (Bettmann et al., 2022; Brown and Bruce, 2016; Greer and Vin-Raviv, 2019; Hoge et al., 2004). It may be the case that participation in a wilderness program could provide a more acceptable gateway to a broader range of treatment options for veterans. Our results are largely consistent with the findings of Bettmann et al. (2020, 2023), who found improved attitudes toward seeking professional psychological help at 1-month and 1-year post-trip, respectively, but not immediately post-trip. Our findings extend to a broader post-trip time period and a broader range of potential treatment options, including not only traditional one-on-one therapy but also another wilderness trip, group therapy, and therapy with other veterans. Taken together, our findings and those of Bettmann et al. (2020, 2023) suggest the potential long-range value of wilderness trips for improving veteran openness to psychological treatment options.
In addition, in both our quantitative and qualitative results, veterans reported positive attitudes and behaviors related to mental health. In our survey, nearly all participants reported that after participation in the HFV program, they realized that there are positive ways to address mental health, and a large majority agreed that they are now more willing to discuss their mental health with others. Qualitatively, similar themes emerged for a sizeable minority of participants who wrote about asking for help, seeking out services, and attending more to their own psychological and emotional needs. Previous studies have consistently shown veterans’ reluctance to discuss their mental health with others due to beliefs about personal responsibility for their mental health and feeling shame for experiencing psychopathology symptoms (Bettmann et al., 2022; Crawford et al., 2015; Dickstein et al., 2010; Shields et al., 2017; Wesselmann et al., 2018). Happily, after HFV, veterans reported being willing to speak about their mental health with others, indicating that HFV provided a safe space to explore therapeutic benefits and improved attitudes and behaviors related to mental health.
Our second hypothesis was also supported. Our results suggest that participation in a wilderness therapy program may assist veterans socially by helping them feel more comfortable connecting with others and forming relationships in loosely structured group activities. This may help increase feelings of social connection and social behaviors while reducing feelings of isolation typically seen in veteran populations (Bettmann et al., 2022; Cacioppo et al., 2015; Wesselmann et al., 2018). Many veterans who participated in the HFV wilderness program (55.6%) felt camaraderie with their fellow veterans, describing belonging, connection, brotherhood, and understanding in the qualitative data. HFV’s therapeutic discussions may also have helped encourage positive feelings regarding mental health conversations, as many reported in close-ended questions and open-ended responses being more willing to discuss their mental health after their trip. A meta-analysis by Bowen and Neill (2013) examined wilderness therapy participant outcomes, including social development, which was defined as the “capacity to interact within social situations.” The researchers found significant improvement in social development in the short term (M = 181 days). Our study extends this, assessing social outcomes up to 21 months for 10 of our participants and asking specifically about comfort levels with building relationships, being in social settings, and new inspiration to connect with other veterans. The findings from the meta-analysis are consistent with those of the present study, which may indicate the potential benefit of veteran wilderness programs for improving feelings of social connection broadly as well as with other veterans.
Veterans also seemed to perceive themselves in a more positive and nuanced way after the HFV program, with a sizeable minority mentioning new feelings of confidence, sense of purpose, and insight in their written responses. Improved insight and self-compassion may also allow veterans grace to understand the depth of their trauma and give themselves permission to seek treatment and reach out to others, contributing to the range of psychosocial improvements we found.
Additionally, our third hypothesis was supported, and our results indicated that veterans who participate in the HFV programs, which teach coping and life skills, will likely find those skills beneficial and continue using them after the trip ends. Veterans nearly unanimously rated the philosophical readings and discussions of HFV to be beneficial (96.4%), with mindfulness also widely endorsed as beneficial (82.1%), and half of the participants reporting life skills and yoga to be beneficial (50% for both). A large majority of veterans reported continuing to use life skills (89.3%) and mindfulness (85.7%). However, it was not the case that participants endorsed all skills as useful, suggesting that acquiescence bias is not a major concern. Only a minority of participants reported finding Qigong to be beneficial (35.7%), and only one veteran reported continuing to practice it. The qualitative analysis broadly confirmed the quantitative results regarding coping, with 70.4% of respondents spontaneously mentioning the benefit of coping strategies they learned from the trip. Participants expressed the value of the skills they learned and reported using them in challenging times.
We also examined the associations among our variables and, as would be expected, found that well-being was negatively associated with psychological distress, with those reporting more flourishing tending to report fewer anxiety and depression symptoms and vice versa. Fortunately, we also found that those with higher anxiety and depression symptoms tended to report more openness to treatment. Similarly, we found a significant negative correlation between well-being and continued coping, with those who rated their flourishing lower reporting continuing to practice more coping skills on their own. This is promising because individuals who report lower well-being and flourishing have a greater need for effective coping mechanisms that can help them improve in the long run. Our participants who reported less distress and greater well-being reported higher benefits from their use of coping practices.
Many of our findings about the potential benefits of wilderness therapy are likely interrelated as veterans reflect back on their trip between 6 and 21 months after the program. For example, there are several potential explanations as to why participation in a wilderness program may encourage veterans to be open to further treatment. For one, experiencing a reduction in psychopathology symptoms (as other studies have reported, e.g., Vella et al., 2023) after participation in these programs may bring the benefits of treatment into sharp relief, encouraging them to seek further care. Another potential explanation is the reexperiencing of camaraderie with fellow veterans. Many feel isolated after retiring from the military, believing others do not understand their pain and missing the tight-knit community present during active service (Wesselmann et al., 2018). Reexperiencing the bonding on these wilderness trips allows veterans to feel part of a community again and understand that others share their feelings and experiences. Participants expressed this in their open-ended written responses in the present study. One last explanation may be learning effective coping skills on wilderness trips, which in turn may help veterans see the benefit of using and perhaps enhancing those skills with others, including a therapist. For example, participating in group discussions can help veterans feel more comfortable sharing their experiences with others and realize the benefit of talking about their thoughts and feelings. Additionally, listening to the advice of others may encourage further asking for guidance, either from a trusted confidant or a trained professional. Any or all of these reasons could explain why wilderness therapy programs may encourage veterans to be more open to further treatment options.
The benefit of wilderness therapy interventions broadly may also be due to their location in nature and away from day-to-day stressors. Nature has been hypothesized as a source of healing for decades, and studies have suggested its benefit for improving mental and physical health (Berto, 2005; Bettmann et al., 2021; Bratman et al., 2012; Hansen et al., 2017; Hunter et al., 2019; Kaplan and Kaplan, 1989; Ulrich et al., 1991). Several of our participants wrote about the value of being out in nature, and some noted seeking out time in nature after the program. This suggests that the trip offered some of them a blueprint for self-care and self-reflection.
Limitations and Further Research
The results of this research should be viewed in light of its limitations. The study’s sample size of 28 participants limits generalizability and should be expanded in future research. Another potential limitation is the absence of a pretrip assessment and the retrospective nature of the data. Veterans were surveyed up to 21 months after completing the program, which offers important information about their long-term disposition, but we cannot conclusively determine changes in behaviors and cognition due to wilderness therapy participation. The time lapse between participation and the survey could produce recall bias. However, the likelihood of improvements due to HFV wilderness therapy is supported in four ways: (1) participants indicated positive changes on survey questions about changes resulting from the program; (2) participants reported improvements since pretreatment in their open-ended written responses; (3) positive psychosocial changes from HFV would be consistent with psychopathology improvements found in Vella et al. (2023) HFV pre- to post-therapy comparisons; and (4) improved treatment openness from HFV would parallel the improvements due to other wilderness therapy reported by Bettmann et al. (2020, 2023). Further research comparing wilderness therapy pre- and post-trip psychosocial functioning and attitudes toward an expanded range of treatment options would further advance our knowledge in this area.
Conclusion
Wilderness therapy programs offer promise for treating veterans. The current study found evidence that participants in the HFV program reported being open to further treatment, had positive attitudes about their mental health, experienced improved social connection and coping benefits and continuance, and grew in confidence and insight. This is particularly encouraging as participants were between 6 and 21 months out from program participation, suggesting the longevity of potential wilderness therapy program benefits.
Authors’ Contributions
A.T.D.: Conceptualization (equal), methodology (equal), data curation (lead), formal analysis (equal), writing—original draft (lead), and writing—review and editing (equal). L.L.V.: Conceptualization (equal), methodology (equal), data curation (supporting), formal analysis (equal), project administration, resources, supervision, writing—original draft (supporting), and writing—review and editing (equal).
Footnotes
Author Disclosure Statement
The authors declare that none of them have any conflicting interests regarding this study, its subject, or methodologies.
Funding Information
None of the authors received financial support for this article’s research, authorship, and/or publication.